


ABSTRACT
Thyroid dysfunction directly affects human health and overall well-being; various approaches are available for the treatment of thyroid diseases, including conservative measures and surgical interventions. Despite advancements in conservative treatment, surgery remains the preferred option. Hypoparathyroidism is the primary cause of hospitalization after thyroidectomy, leading to cost-related concerns and a detrimental impact on patients’ overall quality of life. Postoperative hypoparathyroidism can result in hypocalcemia, and these are challenging conditions that must be identified promptly to prevent immediate and long-term complications. This article focused on the presentation, risk factors, and management of hypoparathyroidism to increase awareness of the risks associated with certain variables, thereby enhancing our ability to predict the risk of this condition. Furthermore, this review highlighted the surgical techniques that may be utilized to prevent hypoparathyroidism. These considerations can help guide preoperative discussions regarding the benefits and potential risks of thyroidectomy.
Thyroid disease is the most predominant endocrine disease worldwide. Therapeutic options for this condition include pharmaceutical and surgical interventions, with thyroidectomy being the preferred treatment option. Currently, thyroid surgery is considered a safe technique due to improvements in operative techniques, surgical equipment, and anesthesia.1 However, as with other procedures, thyroidectomy is associated with potential complications. Of these, hypoparathyroidism and recurrent laryngeal nerve palsy are the most frequently observed and negatively affect the patients’ overall quality of life.1
A comprehensive understanding of thyroid anatomy, the embryological origin of the parathyroid glands (PGs), their blood supply, and the variations and relationships between the thyroid and PGs is essential to mitigate any complications related to thyroidectomy.2 Furthermore, although the PGs are typically located partially subcapsular to the thyroid lobe, they may be concealed within the fatty tissue surrounding the thyroid or among the lymph nodes (LNs). In some cases, the PGs are found entirely within the thyroid gland.3 Thus, this anatomical knowledge is crucial to ensure safety during thyroid or parathyroid procedures and reduce the risk of postoperative complications.
Most individuals have 4 PGs, although fewer than 4 and supernumerary glands have also been reported.2 The superior and inferior PGs are generally oval, vary in color from yellow to reddish brown, and are located close to the thyroid. Their positions are symmetrical in 80% and 70% of cases, respectively, with an overall relative symmetry of 60% for all 4 PGs.2 In most instances, the inferior thyroid artery serves as the primary blood supply for both the upper and lower PGs.2
The primary role of the PGs is to synthesize parathyroid hormone (PTH), which has a half-life of 3-5 minutes (min). Parathyroid hormone regulates calcium and phosphate homeostasis; it increases calcium absorption in the kidneys and intestines, stimulates vitamin D production, and facilitates bone remodeling. In addition, vitamin D reduces calcium and phosphate excretion in the kidneys and enhances bone resorption and calcium uptake from the intestines.3
Hypoparathyroidism, which leads to hypocalcemia, is the primary cause of hospitalization following thyroidectomy. This is believed to result from the unintentional removal or devastation of the PGs, leading to inadequate synthesis or a lack of PTH. This typically occurs as an iatrogenic consequence of total or completion thyroidectomies.3,4 Unfortunately, identifying hypocalcemia is not possible earlier than 24–48 hours after surgery; however, PTH levels can serve as an early indicator of hypocalcemia. Indeed, several studies have investigated the feasibility of using intact PTH levels to predict hypoparathyroidism.5
Nonetheless, post-thyroidectomy hypoparathyroidism remains a clinical surgical dilemma. This comprehensive article aimed to review the presentation, risk factors, and clinical management of this challenging condition. A particular emphasis was placed on crucial surgical techniques that can decrease the likelihood of its occurrence. Thus, this review can contribute to the prevention and management of the condition, thereby leading to positive treatment outcomes.
Definitions and incidence
Hypoparathyroidism can be either permanent or transient. Transient hypoparathyroidism persists for no more than 6 months after thyroid surgery; it is characterized by hypocalcemia, high phosphorus levels, and decreased PTH levels. In contrast, permanent hypoparathyroidism persists for more than 6 months after surgery; it is characterized by the need for calcium or calcitriol 6 months after surgery. Furthermore, some investigators have defined permanent hypoparathyroidism as a state in which the synthesis of PTH is insufficient to preserve a normal level of calcium more than 6 months after surgery.6 In cases where calcitriol is not administered, PTH levels are often low or undetectable.3,7
Hypoparathyroidism can be classified as either biochemical or clinical. Biochemical hypoparathyroidism is characterized by an intact PTH level falling below the lower threshold of the reference range (often 12 pg/mL); it is accompanied by hypocalcemia. In contrast, clinical hypoparathyroidism is a condition in which biochemical hypoparathyroidism leads to hypocalcemia.3
Hypocalcemia is defined as a serum calcium level lower than the minimum value within the reference range; however, the reference range varies by medical center. In addition, the deviation of calcium levels from the normal range may indicate fluctuations in electrolytes and hydration status rather than actual hypocalcemia.3,7 Consequently, hypocalcemia can arise separately from hypoparathyroidism, whereas untreated hypoparathyroidism always results in hypocalcemia, although the delay can vary from hours to days.
Transient hypocalcemia frequently occurs during the first postoperative phase after total or redo thyroidectomies.3,7 Typically, PG function will be fully restored within the first year after surgery, leading to the normalization of calcium levels.4 Consequently, classifying individuals with persistent hypoparathyroidism earlier than 12 months post-surgery may result in inaccurate estimates of occurrence.4
The incidence of hypoparathyroidism differs according to the definition employed.4 Thus, the reported incidences of transient and permanent hypoparathyroidism vary, with an overall risk of 1.7–68%. The incidence of transient post-thyroidectomy hypocalcemia has been reported to be 27.4%, although the occurrence ranges from 6.9–46%.8,9 For permanent post-thyroidectomy hypocalcemia, the incidence is 12.1%,with a range of 0.4–33%.8,9 As with hypoparathyroidism, these wide ranges may be attributed to the different definitions used to identify hypocalcemia.10
For a national perspective, a summary of the prevalence of post-thyroidectomy hypocalcemia in several cities in Saudi Arabia are compiled in Table 1.11-27
- Prevalence of hypocalcemia in different Saudi Arabian cities.
Presentations
Hypocalcemia may or may not be accompanied by symptoms, which typically manifest as cardiac and neurological complications. The latter includes paresthesia, which is characterized by abnormal sensations such as tingling and numbness in the extremities and perioral area, as well as muscle cramps.3 Other symptoms such as irritability, depression, disorientation, laryngospasm, bronchospasm, and seizures have also been observed. Signs of hypocalcemia include tetany, a positive Trousseau sign, or a positive Chvostek sign. Moreover, it presents with refractory congestive heart failure and an elongated QT interval.3,4,28
The long-term consequences of hypoparathyroidism include cardiac issues, posterior subcapsular cataracts, basal ganglia calcification, chronic renal disease, nephrocalcinosis, and psychiatric problems.28,29 In addition, patients may require a prolonged hospital stay owing to seizures and a higher rate of cardiovascular events. This is especially common in those with underlying cardiovascular diseases. Certain reports have also indicated an increased mortality rate.3,30,31
Pathophysiology
Hypoparathyroidism is caused by accidental damage or removal of the PGs. This damage may result from electrical or thermal injury, devascularization, or disruption of venous drainage.3 Blood flow to the PGs is complex and meticulous awareness is necessary during thyroid surgery to guarantee their protection. The inferior thyroid artery typically serves as the primary source of blood supply to the PGs; however, the superior thyroid artery and vessels within the thymothyroid cord have been reported to be more prominent in certain individuals.3 Damage to the PGs results in impaired PTH secretion, which hampers bone resorption, diminishes the renal production of 1,25-dihydroxyvitamin D, and lowers intestinal calcium absorption. Ultimately, this results in postoperative hypocalcemia.3
Risk factors
Numerous researchers have endeavored to identify factors that can predict the occurrence of post-thyroidectomy hypocalcemia. These include various clinical, biochemical, anatomical, and technical factors. Risk factors can be classified as modifiable or nonmodifiable. Modifiable risk factors include hypomagnesemia and Vitamin D deficiency; nonmodifiable factors include Graves’ disease and postoperative PTH levels.29 Establishing such factors may aid in the prompt recognition and prevention of post-thyroidectomy hypocalcemia, thus reducing its consequences, decreasing the length of hospital stay, and minimizing unnecessary laboratory investigations.3,32-34 Adjusting the method or scope of the surgical procedure may be suitable in patients classified as high risk. Alternatively, novel preventive approaches such as fluorescence imaging can be employed to identify or preserve the PGs.29
Clinical factors
Female gender, Graves’ disease, thyroiditis, concomitant diabetes, advanced age, and thyroid cancer have all been shown to increase the risk of hypoparathyroidism. Furthermore, a recent study showed that Graves’ disease and female gender were the only factors contributing to the occurrence of post-thyroidectomy hypocalcemia.3,32-34
Several studies have attempted to elucidate the correlation between female gender and post-thyroidectomy hypocalcemia. These findings indicate that gender differences may be attributed to genetic variances in cell-signaling pathways, the impact of sex hormones on PTH secretion, or anatomical variations that can result in more iatrogenic injuries due to a smaller operational field.32
Graves’ disease can cause transient and permanent hypocalcemia. The cause of the higher incidence of hypocalcemia after thyrotoxic thyroidectomies remains unclear. Nevertheless, the increased size of the thyroid gland, accelerated bone remodeling, highly vascularized glands, and existence of adhesions between the PGs and thyroid capsule contribute to the surgical complexity in these cases.10,34
Hypoparathyroidism is more prevalent in patients with diabetes; however, the precise mechanism remains unclear. One hypothesis suggests that diabetic microangiopathy temporarily renders the PGs more susceptible to hypoxia, resulting in a delay in the return to normal function.34,35
Different viewpoints have been expressed regarding the relationship between patient age and the occurrence of postoperative hypocalcemia. Some studies have identified a relationship between transient hypocalcemia and older age, whereas others have observed a correlation with younger age.34 Conversely, other investigators have found no correlations between age and hypocalcemia.34 These discrepancies may be attributed to variations in sample size, study design, and subject selection. Therefore, additional research is required to investigate whether age contributes to the development of hypocalcemia after thyroidectomy.
Lastly, thyroidectomy for cancer is considered a high-risk procedure due to the complete removal of the posterior capsule along with the glands, thereby simultaneously affecting the PGs.34
Biochemical factors
Hypoparathyroidism, hypomagnesemia, preoperative vitamin D deficiency, and preoperative calcium levels are associated with post-thyroidectomy hypoparathyroidism.32 Thus, it is advantageous to assess the preoperative 25-hydroxy vitamin D, PTH, and calcium levels when the planned thyroid surgery is bilateral.3,7
Magnesium and calcium have comparable chemical characteristics and use the same regulatory homeostasis system. Magnesium can control the production and release of PTH, influence the responsiveness of certain organs to PTH, and contribute to the formation of 1,25-dihydroxyvitamin D3, which in turn affects calcium balance.32
Preoperative vitamin D insufficiency increases the likelihood of post-thyroidectomy hypocalcemia.32 Furthermore, it leads to a decreased conversion of 1,25-dihydroxyvitamin D3 in response to PTH. Consequently, phosphorus excretion from the kidneys is blocked, preventing the absorption of calcium by both the intestines and renal tubules. Concurrently, the calcium present in the bone cannot be released, leading to an imbalance in serum phosphorus and calcium levels. Ultimately, this results in the development of hypocalcemia. Thus, closely monitoring vitamin D levels and providing vitamin D supplementation is essential to avoid post-thyroidectomy hypocalcemia.32 The approved dosage for vitamin D3 (cholecalciferol) is 50,000 IU weekly or 6,000 IU daily for 8 weeks.3
If preoperative calcium levels are higher than normal, examining PTH levels is necessary to assess for hidden primary hyperparathyroidism, which can be effectively treated during thyroidectomy. This is essential because an increased preoperative PTH level is often caused by secondary hyperparathyroidism resulting from vitamin D deficiency. Conversely, if calcium levels approach the lower limit or fall below the normal range, the chance of hypoparathyroidism is elevated. In such cases, starting planned oral calcium supplementation before surgery may be recommended.3,7
Anatomical and technical factors
Large or retrosternal multinodular goiter, gland size, total thyroidectomy, redo surgery, parathyroidectomy, modified radical neck dissection, central LN dissection, and previous gastric bypass are associated with post-thyroidectomy hypoparathyroidism.32 Regarding gland size and redo surgery, the enlargement of the thyroid and the complexity of the neck’s anatomical structure are hypothesized to result in a smaller surgical field. A smaller surgical file poses challenges in accurately detecting and safeguarding the PGs.33
Surgical tips
Ensuring preservation of all 4 PGs during total thyroidectomy is a crucial surgical objective; consequently, it is essential for surgeons to precisely identify parathyroid tissue. However, achieving this goal may not always be possible because of anatomical differences in the positions and blood supply of the PGs, as well as thyroid disease extension. Notably, the PGs are challenging to differentiate from other cervical tissues due to their diminutive size and pigmentation that is comparable to that of the thyroid, adipose tissue, and LNs. Nonetheless, the necessity of identifying all PGs during thyroidectomy and its significance in decreasing the likelihood of hypocalcemia is a subject of debate with inconsistent findings.3 Some experts have even reported that the likelihood of postoperative hypoparathyroidism increases with increasing numbers of identified PGs; patients with one or no PGs detected had the lowest likelihood of developing hypoparathyroidism. Conversely, other investigators have reported opposite observations.36 Thus, further research is warranted to definitively determine the significance and utility of identifying all PGs during thyroidectomy.
Notably, the inferior PGs are more susceptible to injury than the superior PGs. This becomes more apparent when central LN dissection is performed as most central LN metastases are observed in the lower paratracheal and pretracheal regions. Crucially, dissection of the central LN that is on the same side as the primary thyroid tumor should typically be performed as the initial step. Subsequently, to determine whether additional nodal dissection is necessary, the likelihood of contralateral central LN metastasis should be weighed against the likelihood of hypoparathyroidism.3
Energy devices used for vascular sealing play a significant role in the technical aspects of thyroid surgery. These devices create an area of thermal spread in the tissues. A distance of 3–5 mm is required between the instrument and PGs to prevent heat damage.
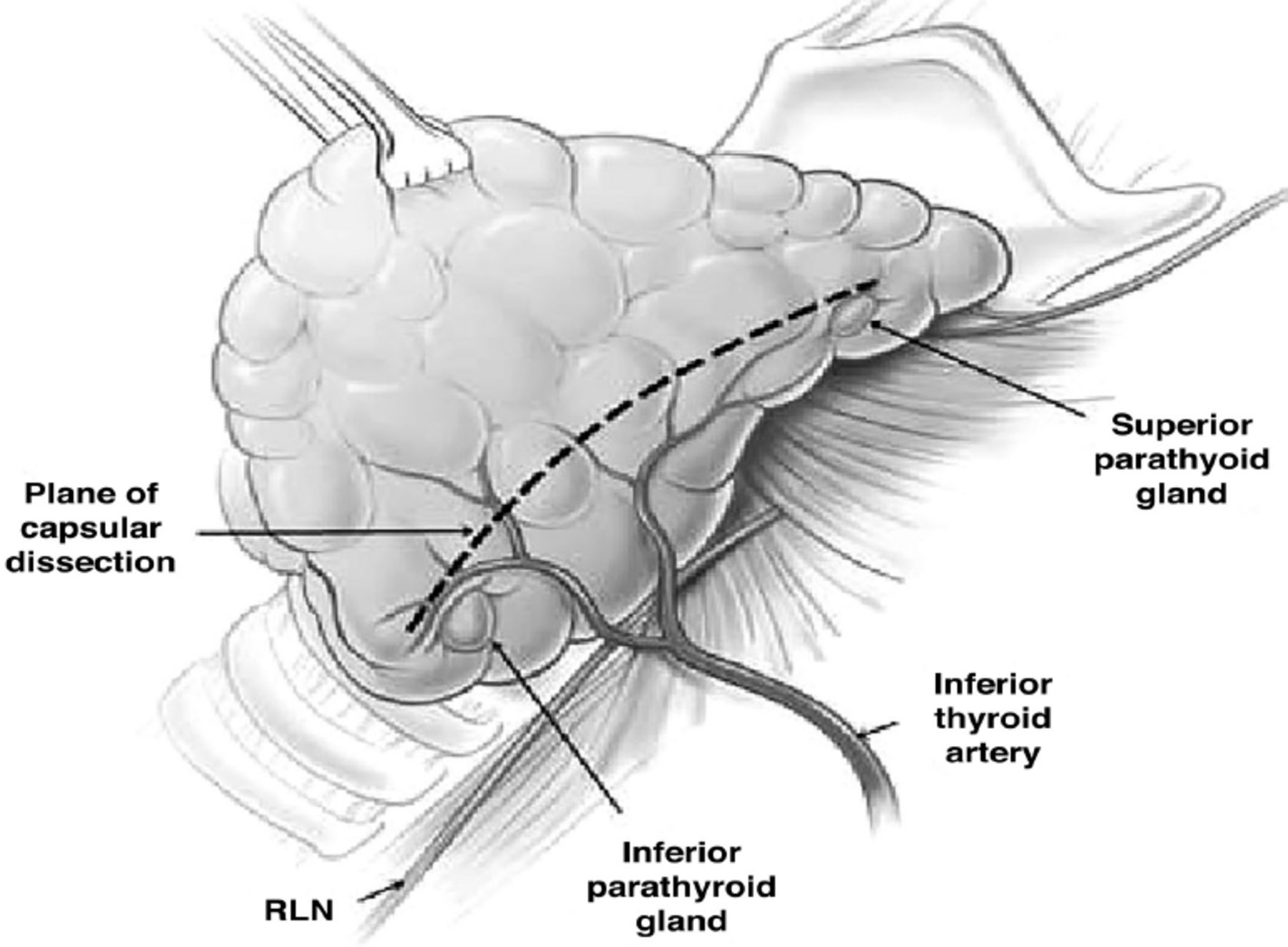
Importantly, capsular dissection, where the perithyroidal fatty tissues are removed from the thyroid surface, should be gentle and meticulous to maintain blood supply to the PGs. To ensure such a strategy, dissection should be performed immediately on the thyroid gland surface, specifically on the medial or anterior side of the PGs (Figure 1).3,29 Notably, the small inferior parathyroid vein occasionally runs laterally and anteriorly to the carotid artery. Once found, it is crucial to conserve this vessel, as it can be traced to facilitate the detection of the inferior PGs.3 Moreover, the use of a loupe at 2.5x magnification has been shown to dramatically decrease the occurrence of unintentional PG removal and reduce the rates of postoperative hypocalcemia.3

- The plane of capsular dissection used during thyroidectomy. This approach is taken to ensure the preservation of the blood supply to the parathyroid glands (reproduced with permission from Rao et al.29 RLN: recurrent laryngeal nerve.
Near-infrared fluorescence imaging
Recent advances in parathyroid identification have been achieved using near-infrared fluorescence imaging. A recent study demonstrated that near-infrared autofluorescence is a reliable technique for detecting the PGs during parathyroidectomy and thyroidectomy irrespective of the disease state.37 This indicates that PG autofluorescence is high compared with the surrounding tissues, including the thyroid, adipose tissue, trachea, and muscles.37
The mechanisms of PG autofluorescence when exposed to near-infrared fluorescence remains unknown. One hypothesis suggests that the abundance of calcium receptors in the PGs and their relationship with fluorescence intensity may be an influencing factor. Another hypothesis proposes that variations in cell density and proportions of oxyphil cells, chief cells, and adipose tissue in the PGs affect fluorescence.37
Parathyroid autotransplantation
Any identified PGs should be evaluated for devascularization. Sharp scoring of the PG capsules can effectively reduce venous congestion, leading to rapid normalization and color improvement. Nevertheless, the occurrence of ischemia in the PGs can be inconspicuous and challenging to identify.
One frequently encountered surgical challenge is determining the suitability of autotransplantation for PGs that have become discolored and show no signs of improvement. Parathyroid autotransplantation (PA) involves initially preserving the removed parathyroid tissue in chilled saline solution. A small frozen tissue section is then sent for analysis to confirm PA suitability. If appropriate, the PG is then fragmented into 1 mm pieces and transplanted into the sternocleidomastoid muscle or other suitable locations.3
The overall objective of PA is to mitigate the likelihood of persisting hypoparathyroidism.3 Although PA during thyroid surgery has been linked with a higher likelihood of temporary hypoparathyroidism, routine PA may correlate with a decreased likelihood of permanent hypoparathyroidism.3
Postoperative management
The objective of treating hypoparathyroidism, whether real or potential, is to prevent hypocalcemia-associated symptoms and complications. After completion or total thyroidectomy, many strategies can be employed to avoid, identify, and manage post-thyroidectomy hypocalcemia. For instance, calcium levels (with or without PTH) can be monitored and oral calcium supplementation may be administered with or without calcitriol depending on the results. However, patients may be discharged from the hospital before the drop in calcium levels, which typically occurs 24-72 hours after surgery.3 Hence, it is crucial to predict the likelihood of hypocalcemia occurrence, inform patients about its potential manifestations, and instruct them on the necessary measures to be taken.3
The occurrence of acute hypocalcemia after thyroidectomy has been shown to correlate with decreased PTH levels.7 Consequently, some investigators have checked PTH levels during surgery or recovery to offer guidance on calcium supplementation.
Prophylactic management
A practical preventive method for the management of potential hypocalcemia is the regular administration of oral calcium with or without calcitriol, without monitoring for PTH or calcium levels. Some studies routinely administered prophylactic calcium with or without calcitriol to all patients, resulting in a low incidence of symptomatic hypocalcemia. This method decreases the incidence of postoperative hypocalcemia by approximately 10%. Orally administered calcium carbonate is the most commonly accessible and cost-effective form of supplemental calcium. The recommended dosage is 500–625 mg to 1000–1250 mg 2–3 times daily.3
Hypoparathyroidism treatment
The recommended initial treatment for hypoparathyroidism or symptomatic hypocalcemia after thyroidectomy is oral calcium carbonate administered at a dosage of 1–2 g 2–3 times a day. Calcium citrate is the optimal substitute in specific circumstances such as atrophic gastritis, prior gastric bypass, and in patients receiving proton pump inhibitors.3,7 If hypocalcemia persists despite oral calcium intake, supplementing with oral calcitriol at a dosage of 0.25–0.5 mg twice daily is recommended. If severe, unresponsive, or life-threatening complications of hypocalcemia occur, intravenous calcium and calcitriol should be administered.3,7
Teriparatide (recombinant PTH) has been proposed as a pharmacological approach to treat post-thyroidectomy hypoparathyroidism that does not respond to oral or intravenous calcium and calcitriol.7 However, further research is needed as limited data have been reported on its clinical efficacy.
In conclusion, post-thyroidectomy hypoparathyroidism poses a considerable challenge for both endocrine surgeons and endocrinologists. This review provides detailed insights into the anatomical variances of PGs, risk factors of post-thyroidectomy hypoparathyroidism and hypocalcemia, and treatment options for these conditions. This will allow endocrine surgeons to master and refine their surgical techniques, leading to better treatment outcomes. Furthermore, by gaining a deeper understanding of these conditions, early detection of hypocalcemia is more likely. Overall, this will contribute to prevention and prompt management, thereby positively influencing patients’ quality of life, reducing hospital stay duration, and minimizing unnecessary laboratory investigations. Nonetheless, extensive multicenter prospective studies are necessary to address ongoing issues and further explore preventative measures.
Acknowledgment
The author would like to thank the Deanship of Postgraduate Studies and Scientific Research at Majmaah University for supporting this work under project number R-2024-1384. In addition, we would like to acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}