


Abstract
Objectives: To determine an optimal cuff inflation volume to achieve safe cuff pressure (20-25 cmH2O) in cuffed endotracheal tubes (ETTs) with an inner diameter of 4.5, 5.0, and 5.5 mm, which are commonly used in pediatric anaesthesia clinical practice and to create a formula to determine the optimal cuff volume.
Methods: This study was carried out between February and June 2021 in Ankara City Hospital, Ankara, Turkey. A total of 127 pediatric patients who were intubated with 4.5, 5.0 and 5.5 numbered cuffed ETTs were included in this study. The same brand of cuffed ETT was used for each patient. The diameter of the subglottic transverse airway was measured by ultrasound for selecting the appropriate tube. Cuff pressure was measured with a cuff manometer to ensure optimum cuff pressure (20-25 cmH2O).
Results: We found out that the mean ideal cuff volume inflated for 4.5 size tube was 1.7±0.3 ml, 1.9±0.3 ml for 5.0 size tube, and 2.1±0.3 ml for 5.5 size tube. Additionally we developed the “endotracheal cuff volume (ml) = 1,027 x height (m) + 0,104 x subglottic transverse diameter (mm) - 0,0191” formula to predict the most suitable inflation volume for ETT cuffs.
Conclusion: In this study, we suggested the optimal cuff volume to inflate the cuffs of ETTs 4.5, 5.0, and 5.5, which are frequently used in pediatric anaesthesia practice, in the appropriate cuff pressure range.
ClinicalTrials.gov ref. no.: NCT04948359
Selecting the appropriate endotracheal tube (ETT) size is a critical step for successful endotracheal intubation in pediatric patients.1,2 If the ETT type to be used is the cuffed ETT, it is crucial to monitor and maintain cuff pressure within the normal range. Overinflation of the ETT cuff results in diminished capillary blood flow and mucosal damage, while underinflation causes insufficient airflow and increases the risk of pulmonary aspiration.3 To avoid these complications, a safe cuff pressure range of 20-30 cmH2O has been recommended.4-6 It is possible to prevent complications by keeping the cuff pressure value within this safe range.7
The subglottic tracheal diameter is a crucial parameter guiding the selection of the appropriate ETT type and determining the optimal ETT cuff volume and pressure for pediatric patients. In previous studies, significant correlations were found between optimal cuff volume and the diameter of the subglottic trachea.8-10 In situations where a cuff manometer is unavailable, especially in emergency management, the ETT cuff is likely to be inflated much more than required, with the intent of preventing pulmonary aspiration and providing adequate tidal volume; however, this causes harm to the patient. There is an information gap regarding the optimal cuff inflation volume recommended for cuffed ETT use when the patient is of preschool or school age, which is commonly encountered in pediatric anesthesia practice.
The primary goal of this research is to ascertain the minimal and optimal cuff volumes necessary to ensure sufficient ventilation, prevent pulmonary aspiration, and mitigate mucosal damage in pediatric patients intubated with cuffed ETTs featuring inner diameters of 4.5, 5.0, or 5.5 mm. Additionally, we seek to formulate a calculation method for estimating the cuff volume within the safe range of cuff pressure for inflating cuffed ETTs in patients within the specified population. The secondary objective of this study is to explore the association between postoperative complications and cuff volume.
Methods
A total of 127 patients were recruited to this prospective observational study, comprising 42 participants who were intubated with 4.5 mm tubes, 43 participants who were intubated with 5.0 mm tubes, and 42 participants who were intubated with 5.5 mm tubes. After receiving ethical approval (approval no.: E2-21-76) from the ethical committee of Ankara City Hospital, Ankara, Turkey, this study was carried out between February and June 2021.
Pediatric patients with American Society of Anaesthesiologists (ASA) physical status I-II who were scheduled for surgery under general anaesthesia and underwent endotracheal intubation with a cuffed tube with an internal diameter of 4.5, 5.0, or 5.5 mm were included in this study. The patients were grouped into Group I, Group II, and Group III based on the sizes of cuffed ETTs used for intubation (namely 4.5, 5.0, and 5.5 mm). Patients with a history of tracheostomy, airway obstruction, or anomalies, those expected to have difficult intubation or airway hyperreactivity, patients with a history of bronchial asthma, patients with a body mass index (BMI) above 85% or below 5%, patients whose parents are unable to read, understand, and sign the consent form, and patients for whom parental consent could not be obtained were excluded from the study.
The intubation of each patient was carried out with the same brand of cuffed ETT (Wellkang Ltd., London, England, UK, or Chilecom Medical Devices Co. Ltd.). The inner diameter (ID) and outer diameter (OD) of the cuffed tube used for each participant and the diameter of their subglottic transverse airway were measured via ultrasonography (USG). Peak airway pressure, surgery duration, planned surgeries, additional diseases, previous operations, and demographic data on the patients (age, gender, weight, height, BMI, and ASA condition score) were recorded. Instances of complications, stridor, hoarseness, cough, sore throat, and desaturation (<92% SpO2) were also recorded.
Written consent was obtained from the parents for participation in the study. After standard monitoring, anesthesia was induced with sevoflurane, vascular access was established, and intravenous (IV) 0.5 mgkg-1 rocuronium was administered to the patients. A roll pad was placed under the shoulders of the patients, and when they were in the supine-neutral position with their heads slightly extended (the sniffing position), airway USG was carried out with a linear probe (40 mm, 6-13 Mhz) using a Hitachi EZU-MT2-S1 (Hitachi Medical Corporation, Tokyo, Japan). The linear probe was positioned horizontally at the front of the neck, and the width of the subglottic air column was assessed (in millimeters) at the cricoid cartilage level by scanning the probe from top to bottom. The ultrasound measurements were carried out by an experienced, certified anesthesiologist, while another experienced anesthesiologist, blinded to the ultrasound measurements, carried out the intubation.
The ETT number for each patient was calculated using formulas recommended by previous studies, as well as the traditional age-based Motoyama formula.8-10 Guided by these formulas, tube selection was determined by assessing the subglottic airway’s transverse diameter using ultrasound and relying on the clinical expertise of the anesthesiologist.
The cuff of the ETT to be used was checked before intubation. The study participants were intubated via direct laryngoscopy while in the sniffing position. When resistance was encountered during the passage of the tube into the trachea, this situation was recorded, and the ETT was replaced with a tube 0.5 mm smaller. A leak test was carried out on the cuff before it was inflated with air. The cuff leak test was carried out as follows: I) if there was no leakage sound when the lungs were inflated with an airway inflation pressure of 20-30 cmH2O; II) the tube diameter was considered large; and III) the ETT was replaced with another ETT that was 0.5 mm smaller. However, in cases where there was an audible leakage sound when the lungs were inflated with 10 cmH2O or lower, the ETT was replaced with a tube that was 0.5 mm larger. In cases where minimal tracheal leakage was detected when the lungs were inflated with an inflation pressure of 10-20 cmH2O, the tube size was considered optimal.10 When the appropriate ETT was thought to have been placed in the patient, a stethoscope was placed on the thyroid cartilage to listen to the leakage sound, and the ETT cuff was further inflated by administering air with a 5-ml injector. After volumizing, cuff pressure was assessed using a cuff monometer (VBM Medizintechnik GBMH, Sulz am Nectar, Germany) and then recorded. The most appropriate cuff volume was determined by applying 0.2 ml volume increases or decreases in such a way as to ascertain the optimal pressure (20-25 cmH2O), and the determined pressure was recorded.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences, version 25.0 (IBM Corp., Armonk, NY, USA). In addition to descriptive statistical methods (frequency, percentages, mean, standard deviation [SD], median, min-max), the Chi-square (χ2)test was used to compare the qualitative data during the evaluation of the study data. The conformity of the data to the normal distribution was evaluated by carrying out the Kolmogorov-Smirnov test and Skewness-Kurtosis test, and using graphical methods (histogram, Q-Q Plot, stem and leaf, Boxplot). In the study, the independent samples t-test and One-way ANOVA were used for the evaluation of the quantitative data showing normal distribution, and repeated measures ANOVA was carried out for in-group comparisons. In cases where differences were found in multiple comparisons, the post-hoc Tukey HSD and Bonferroni tests were carried out to identify the source of the difference. Relationships between the variables were analyzed with the Pearson correlation test. Multivariate linear regression analysis was carried out to estimate the variables. A p-value of 0.05 was considered significant.
Before setting up the regression model, which would be capable of predicting the ETT volume, the data were randomly divided into 2 parts: the test set (n=90, 71%) and validation set (n=37, 29%). In the test set, stepwise linear regression analysis was carried out to estimate ETT volume. The independent variables were determined as age, height, weight, and subglottic diameter for the ETT volume. The adequacy of the established regression models was shown with R2. Cross-validation was carried out for the validity of the regression model. For this purpose, the correlation between the actual value and the predicted value, which was obtained by applying the regression model obtained in the test set to the validation set, was analyzed.
Power analysis was carried out using the *Power 3.1.9.7 statistical package program by calculating ETT cuff volume; and power was 93% (where group=3, n=127 [n1=42, n2=43, and n3=42], p=0.05, effect size (f)=0.34).
Results
This study recruited a total of 127 participants, comprising 42, 43, and 42 patients for each tube size used for intubation. The demographic data of the patients are presented in Table 1. As the ETT number increased, the mean age, weight, and BMI values significantly increased in a statistical manner among the groups.
- Demographic characteristics of the patients by group.
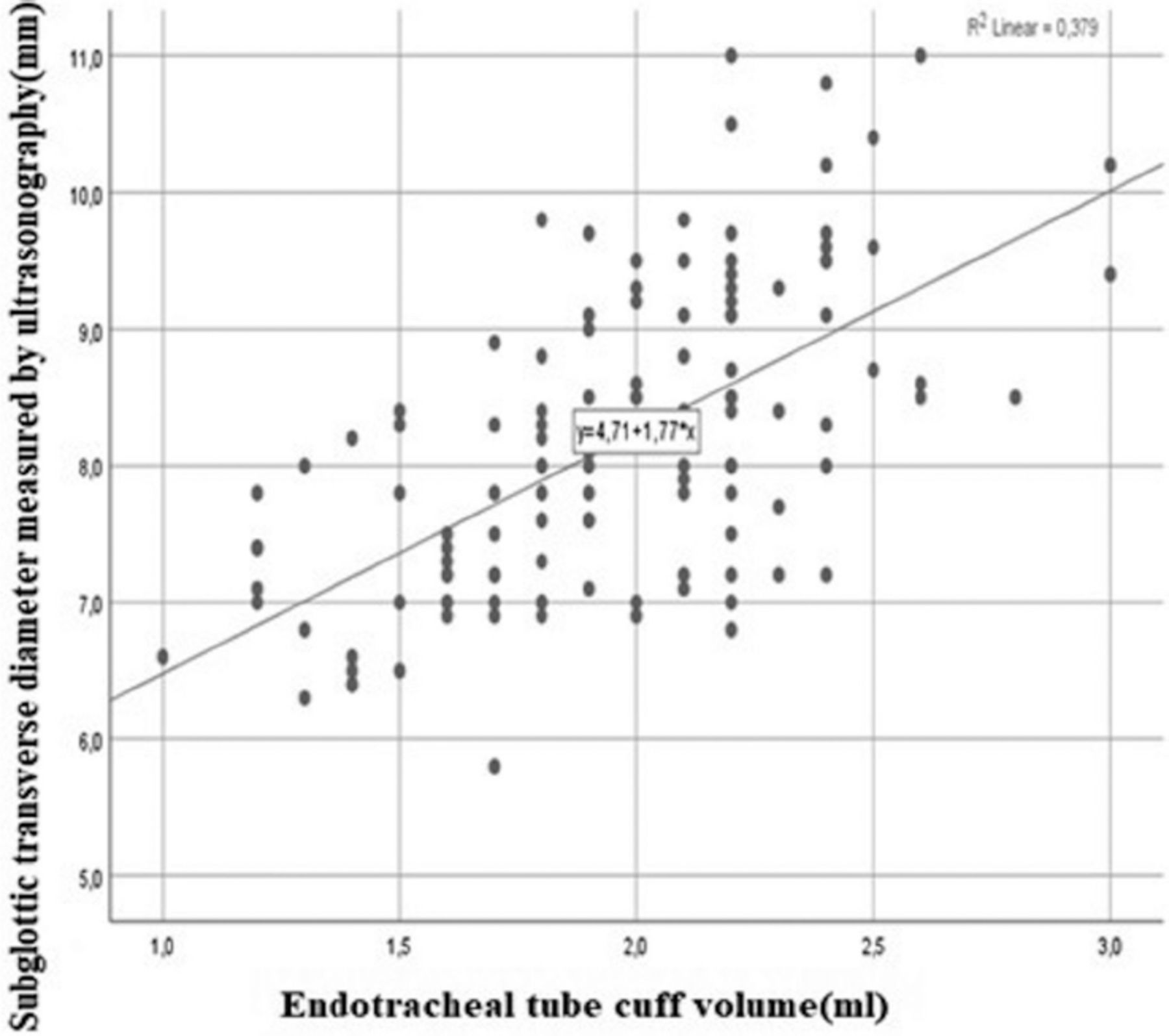
The recommended cuff volume for inflation was 1.7±0.3 ml for Group I, 1.9±0.3 ml for Group II, and 2.2±0.3 ml for Group III. The subglottic transverse diameters, as measured via USG was 7±0.5 mm for Group I, 8.1±0.5 mm for Group II, and 9.4±0.7 mm for Group III. It was found that the ideal cuff volume to which the cuff should be inflated and the subglottic transverse tracheal diameter measured via USG increased as the ETT number increased between the groups, in a statistically significant manner (p<0.001). Multiple comparison tests (post-hoc) were used to determine the study groups with the between-group difference; all group values were found to be different from each other. In addition, a positive correlation was found at the level of r=0.616 between ETT cuff volume and subglottic transverse diameter (as measured via USG, and these relations were statistically significant (p<0.05, Figure 1).

- Relationship between endotracheal tube cuff volume and subglottic transverse diameter measured by ultrasound
To create a predictive mathematical model for estimating ETT volume, stepwise linear regression analysis was carried out. The independent variables were determined to be age, height, weight, and the subglottic diameter for the ETT volume. The significant independent predictors of ETT volume were height (p=0.001) and subglottic transverse diameter (p=0.023).
Estimated ETT cuff volume (ml) = 1.027 × height (m) + 0.104 × subglottic transverse diameter (mm) - 0.191
This model presented with a R2 of 0.50 and a p-value of <0.05 for both independent variables. When subjected to univariate ANOVA, subglottic transverse diameter had R2 value of 0.37 and height had R2 value of 0.44, and the regression model that explained the 50% change in ETT cuff volume was statistically significant. This shows the strong predictive power of height (Table 2).
- Factors predicting the endotracheal tube cuff volume (n=90).
Before setting up the regression model for predicting the ETT cuff volume, the data were randomly divided into 2 sets: a test set comprising 90 (71%) participants, and a validation set comprising 37 (29%) participants. A statistically significant, positive relationship was found between the ETT cuff volume predicted by the regression model and the actual volume (Table 3).
- Correlation of the endotracheal tube cuff volume predicted by the regression model with the actual volume in the validation group (n=37).
There was no statistically significant difference among the groups in terms of the presence of comorbidities, previous surgeries, duration of surgery, airway peak pressure values, and postoperative complications (p>0.05). In patients with complications, a statistically significant relationship was found between subglottic transverse diameter (measured by USG) and operation time. Furthermore, operation duration was longer for participants who developed complications, while subglottic transverse diameter (as measured via USG) was wider in participants who did not develop complications. The only complication observed was sore throat.
Discussion
This prospective observational study determined that the ideal cuff volumes that ensure airway safety in pediatric patients intubated using cuffed ETTs were achieved with cuffed tubes with IDs of 4.5, 5.0, and 5.5 mm, which are frequently employed in clinical practice for pediatric anesthesia. The pilot balloon in cuffed ETTs is an important marker of cuff inflation. Cuffs with low pressure and high volume are typically the most commonly used because they cause relatively minimal mucosal damage. Cuff pressure depends on many factors, such as inflation volume, cuff compliance, intrathoracic pressure, and the relation between cuff diameter and the trachea.2,11 Inflating the ETT cuff with the least amount of pressure that can close the trachea reduces the blood flow to the trachea in the cuff region by approximately 75%. If the cuff is inflated slightly more or in an individual with hypotension, mucosal blood flow is likely to stop completely.2,12
The ETTs used in this study were obtained from the same company, and these ETTs had cuffs with low pressure and high volume. As expected, the inflation volumes needed to ensure optimal cuff volume were higher for a higher average age in all 3 study groups. The mean optimal inflated cuff volumes for Group I was 1.7±0.3 ml, 1.9±0.3 ml for Group II, and 2.1±0.3 ml for Group III. Although these values seem to have only a small margin of difference between each other, it should be noted that a small increase in cuff volume causes significant changes in cuff pressure. Even small differences in the tracheal diameter of a patient can have a significant impact on cuff pressure.
In emergencies, the cuff pressure for a cuff manometer is typically assessed via manual palpation of the pilot balloon in routine practice at medical centers. This method often results in over-inflation of the cuff.13 This study was carried out to determine and recommend a standard that would prevent this undesirable outcome and to develop a formula for the optimal cuff volume for pediatric patients. The regression model created in this study is significant. In the regression model established with the cuff volume data of 90 randomly selected pediatric patients from among the 127 participants in this study, a formula was developed for predicting the optimal cuff volume to which ETT cuffs should be inflated. We found that the height of the patients and their subglottic transverse airway diameter (determined via real-time USG measurement) were the parameters that best explained the predicted endotracheal cuff volume in our study. When the recorded volume was compared with the calculated cuff volume determined as optimal for 37 patients in the validation group, based on the formula, we found that the data exhibited a statistically positive relationship (R2=0.343). This supports the idea that the newly created formula is suitable for use in clinical practice. Shibasaki et al14 aimed to estimate optimal cuff volume using sociodemographic data, such as the age and height of patients and the tracheal diameters obtained directly from the graph. They found the optimal cuff volume to be well correlated with tracheal diameter and moderately correlated with age and height. It is believed that the calculated subglottic transverse trachea diameter of pediatric patients will be especially useful for selecting the correct tube size and determining the optimal cuff volume using the cuff volume formula developed in this study. We concluded that it is appropriate to use ETTs with ID of 4.5 in patients with subglottic transverse airway diameter of 7.0±0.5 mm, ETTs with ID of 5.0 in patients with subglottic transverse airway diameter of 8.1±0.5 mm, and ETTs with ID of 5.5 mm in patients with subglottic transverse airway diameter of 9.4±0.7 mm.
In this study, there was no relationship between cuff volume and postoperative airway complications. The incidence of postoperative sore throat was 5.5%, which is lower than that reported in a previous study.15 We believe that this was because the cuff pressures were kept within 20-25 cmH2O, which is a safer and lower range than the recommended range. Another reason may be the possibility that the study participants, who are in the pediatric age group, were unable to communicate that they had a sore throat.
Study limitations
It was concluded that the cuff volumes to which cuffs were inflated were appropriate just by keeping the cuff manometer measurement within the ideal range and observing that the patients were adequately ventilated. In cuff manometers, it was not possible to calculate the dead space volume during the air inflation phase. In this study, it was possible to carry out a bronchoscopic examination to evaluate whether there was mucosal ischemia and mucosal damage in the patients; however, it was neither appropriate nor practical to carry out the examination on 127 patients or under the conditions in our operating room. In this study, the same brand of ETT was used for all participants. Fischer et al16 compared the cuff volumes of pediatric ETTs with IDs ranging from 3.0-7.0 (which were produced by 5 different companies) at a cuff pressure of 20 cmH2O, and they obtained different volumes in the products of different companies and in tubes with different IDs. They concluded that appropriate and standardized ETT ODs and cuff diameters should be determined in ETT production using pediatric airway data. They state that this increases tracheal intubation success and is essential for reliable pediatric airway management. In our study, pediatric ETTs of different brands were not compared, and only ETTs with 3 different IDs were studied. These are the ETT sizes most commonly used in pediatric practice. It is our belief that more prospective studies are needed on ETTs produced by other brands and ETTs with different IDs.
In conclusion, in pediatric patients, selecting the optimal cuffed ETT and inflating the cuff to create the most appropriate pressure and volume are crucial to ensure adequate ventilation while preventing the risk of pulmonary aspiration. The mean cuff volumes recommended for pediatric patients who are intubated with 4.5, 5.0, and 5.5 mm cuffed ETTs in our study will be helpful and useful in emergencies and in clinics where a cuff manometer is not routinely used. Routine use of a cuff manometer and maintaining the cuff pressure between 20-25 cmH2O is also recommended to prevent airway complications that may develop due to unwanted high cuff pressure in the postoperative period and to improve postoperative patient comfort.
Acknowledgment
The authors gratefully acknowledge Scribendi (www.scribendi.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 3, 2023.
- Accepted December 11, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.