


Abstract
Objectives: To determine the effect of elevated supine position with back support on back pain, anxiety and comfort in patients undergoing coronary angiography.
Methods: This randomized-controlled, experimental study was conducted in the Coronary Intensive Care Unit between September 2021 and January 2022, with an intervention group of 51 patients and a control group of 53 patients. Data were collected using a patient information form, a visual analog scale, the anxiety state inventory and the immobilization comfort questionnaire. Following angiography, the intervention group received pillow support to the back and the bedhead was elevated to 30 degrees. Routine nursing care was applied to the control group. In both groups, the severity of back pain was measured at 0, 2, and 4 hours, and anxiety and comfort at 0 and 4 hours.
Results: The pain severity at 2 and 4 hours after the procedure was determined to be significantly lower in the intervention group than in the control group (p<0.001, p<0.001). At 4 hours, the anxiety levels were similar in both groups (p<0.05), and the comfort level was higher in the intervention group (p<0.001). The mean pain value was 6.003 points lower and the comfort level was 20.499 points higher in the intervention group than in the control group.
Conclusion: The elevated supine position with back support was seen to reduce back pain, increase comfort, and did not change anxiety levels.
Clinical Trials No: NCT05546216
Cardiovascular system diseases (CVD) have been reported by the World Health Organization (WHO) to be the leading cause of the 10 most common causes of death and of these, coronary artery disease (CAD) is the most frequently seen.1,2
Coronary angiography (CAG) is currently the gold standard method for examination of coronary arteries, diagnosis and treatment.3 Following CAG, complications may develop such as bleeding from the femoral artery, hematoma, thrombosis, etc. To reduce these risks to a minimum, patients are instructed to lie supine and remain straight and immobile for 6 hours after CAG.4 This has been reported to be very uncomfortable for patients.4 Back pain has been reported to be the most common complaint following CAG and back pain after CAG can increase sympathetic stimulation.5 As this can increase the cardiac workload, myocardial ischaemia can be exacerbated.4,6,7
The CAG procedure itself and the outcomes are a source of anxiety for patients. Anxiety exceeding a normal level is a cause of many complications.8 The presence of anxiety increases the frequency of acute coronary events and can increase mortality.9 There are also studies that have reported that lengthy bedrest in a supine position is a source of anxiety and decreases patient comfort.10,11 A modified position is very important for patient comfort. It has been reported in the literature that a modified position after CAG reduces back pain and increases patient comfort.12
Pharmacological and non-pharmacological methods are used in the control of back pain and anxiety. One of the non-pharmacological methods is a modified patient position. Supportive pillows are used in patient positions to reduce pain.13,14 Prommanon et al15 recommended that the placement of a supportive pillow behind the back of patients with back pain could reduce back pain. In another study it was reported that changing the bed position and using a supportive pillow after CAG reeduced pain.10 No study could be found in the national or international literature that has examined pain, anxiety, and comfort together when an elevated back position and back support are given to patients after CAG. Therefore, this study can be considered to be specific in this respect and to contribute to this field and future research.
Purpose. The aim of this study was to determine the effect on back pain, anxiety, and comfort of an elevated supine position with back support applied to patients undergoing CAG.
Study Hypotheses. The following hypotheses were tested: H1- Patients in the elevated supported supine position group will have a statistically significant reduction in back pain compared to patients in the control group. H2- Patients in the elevated supported supine position group will have a statistically significant reduction in anxiety level compared to patients in the control group. H3- Patients in the elevated supported supine position group will have a statistically significant increase in comfort level compared to patients in the control group.
Methods
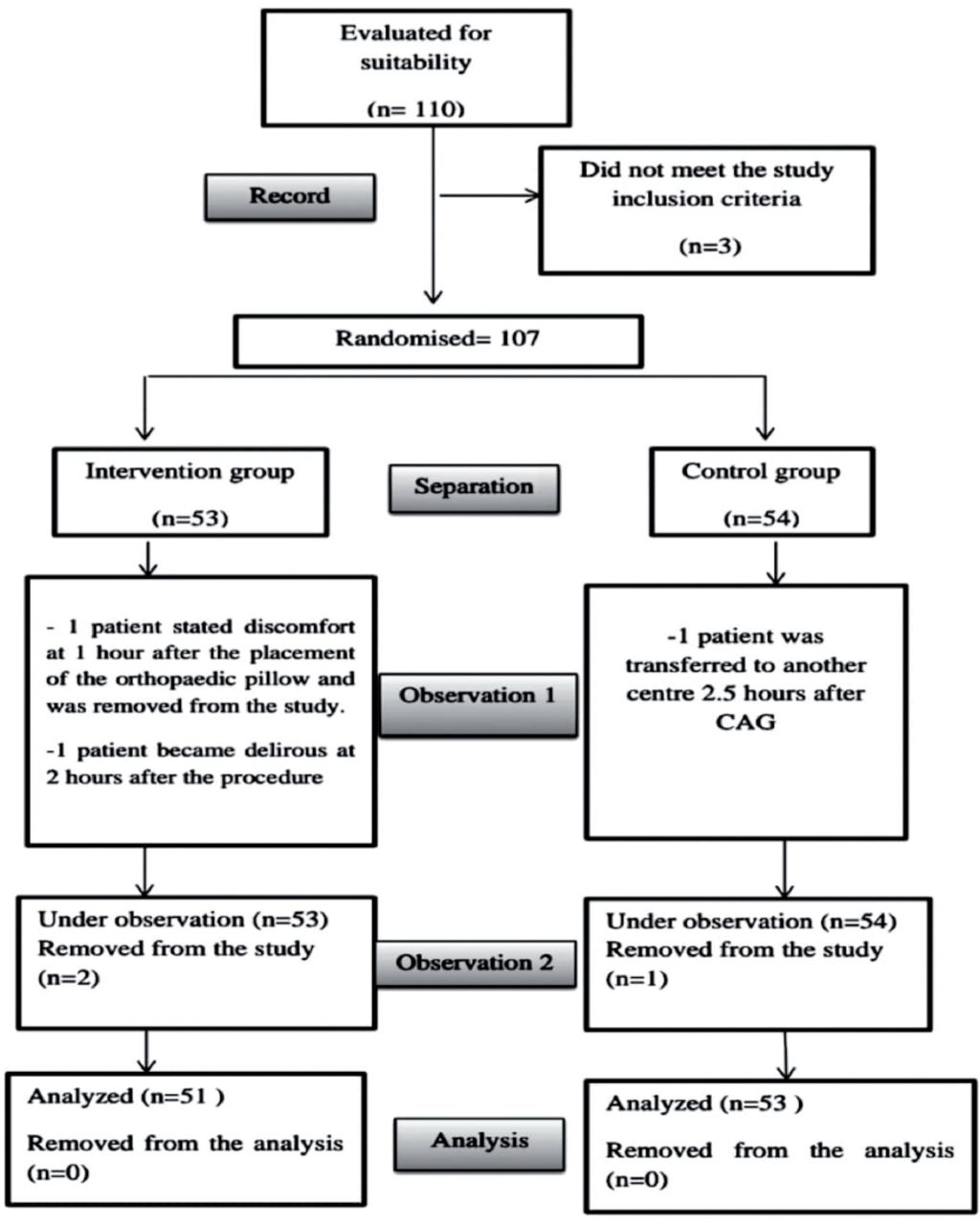
The study was conducted between September 2021 and January 2022 at the Coronary Intensive Care Unit (ICU) of Kahramanmaraş Sütçü İmam University Health Practice and Research Hospital in Turkey. The sample size for the study was determined using G*Power 3.0.10 program. The time difference used was 2 hours, as defined in the study by Sarabi et al16 as the first measurement of back pain after positioning. It was calculated that a total of 46 patients was required as 23 in each group to provide effect size of 1.089, and error margin of 5% in a 95% confidence interval. Considering the risk of losses, more patients were inccluded and the study was completed with 51 patients in the intervention group and 53 patients in the control group (Figure 1, CONSORT diagram).

- Consort diagram of the study.
Study inclusion criteria were defined as age ≥18 years, undergoing femoral angiography procedure, with no psychiatric diagnosis, and no communication problem which would affect cognitive processes. While the exclusion criteria were excluded from the study if they had a history of back surgery, or current presence of hernia, or chronic back or low back pain.
The 107 patients included in the study were randomly separated into 2 groups as the intervention group and the control group. A computer program that generates random numbers was used for the randomization process. Using the randomization list, the patients were randomly separated into the intervention group and the control group in order of admission to the hospital.17 The single blinded technique was used so that patients did nor know which group they were in.17
Independent variables were defined as the patient descriptive characteristics, and in the intervention group, the 30° elevated supine position and the back support. Dependent variables were defined as the mean points of back pain, anxiety, and comfort. Data were collected using a Patient information form, Visual analog scale (VAS), State anxiety inventory (SAI), and Immobilisation comfort questionnaire (ICQ). The Patient Information Form is a 14-item form that includes patient characteristics.10,16,18 Pain intensity was measured using VAS. Visual Analog Scale pain scale has been used in many studies in Turkey.18,19 Anxiety was measured with the SAI. This scale has been used in many studies.19,20 In this study, SAI Cronbach’s alpha value was calculated as 0.983. The validity and reliability of the ICQ in Turkey was tested by Tosun et al21 with a Cronbach alpha value of 0.82. In this study, the Cronbach alpha value of the scale was calculated to be 0.952.
Before the main study, the procedures were applied to 10 patients, as 5 in the intervention group and 5 in the control group. Elevation of the bedhead to 30°, 45°, and 60° has been recommended in literature. These elevations were tested in the pre-application and it was seen that at 45° and 60°, the sandbags shifted in obese patients. Therefore, considering that there could be a risk of bleeding at higher elevations, it was decided that bedhead elevation would be 30° for the study.10,12
The following procedure was applied to the intervention group.10,16 i) Before starting the procedure, the hands were washed then dried with a single-use, z-folded, paper towel. ii) At the end of the CAG the patient was positioned supine on the bed. iii) The patient was monitored. iv) Bleeding at the CAG entry site was checked. v) The hemodynamics of the patient were evaluated. vi) The patient was informed about the study and written informed consent for participation was obtained. vii) Before the procedure, at 0 hour, pre-test data were collected with the Patient Information Form, VAS, SAI, and ICQ. viii) The sheath was fixed to the groin of the patient with a plaster. ix) Before the procedure, the silicon pillow for each patient was wrapped in a clean, non-sterile, single-use bed protector to prevent the spread of infection. x) The patient was moved into a left lateral position for a very short time by 2 nurses and a no-sweat, gel, orthopaedic silicon pillow (a 36 x 33 x 10 cm) was placed in the lower back gap of the patient.22,23 xi) The patient was then immediately placed in the supine position. xii) The bedhead was elevated to be at 30°. xiii) Communication with the patient was maintained throughout the procedure. xiv) Pain was measured with the VAS at 2 and 4 hours after positioning the patient. The SAI and ICQ were applied again after 4 hours. xv) The patient lay in the same position for 4 hours. xvi) The patient was observed for 5 hours in respect of complications. xvii) Patient confidentiality was maintained in all the procedures applied to the patients.
At the end of CAG, patients in the control group were bed in a supine position and their vital signs were evaluated. They were monitored for complications. Control group data were collected at the same time as the intervention group.10,16
The position of the sandbag was checked every 30 minutes, and all patients were evaluated every hour in respect of complications such as bleeding and hematoma. The lower extremities of each patient, especially the right leg where the sandbag was placed, were evaluated in respect of temperature, heat, and color. Capillary refilling time was evaluated in each patient. Communication was maintained with the patients throughout the intervention.
Statistical analysis
Data obtained in the study were analyzed statistically using Statistical Package for the Social Scienced, v. 26 software (IBM Corp., Armonk, NY, USA). Descriptive statistics were stated as number (n), percentage (%), mean values in a 95% confidence interval (CI), median and interquartile range (IQR) values. Conformity of numerical variables to normal distribution was evaluated with the Shapiro Wilk test. Variance homogeneity was evaluated with the Levene test. In the comparisons of categorical variables between groups, the Fisher Exact test was applied. Two-way variance analysis was used to compare the repeated measurements of SAI and ICQ at 0 and 4 hours between the groups. In the evaluation of the VAS scores at 0, 2, and 4 hours, the Mann Whitney U-test was used for comparisons between the groups and Friedman analysis for comparisons within the groups. When significant differences were found between the measurements, Bonnferroni correction was applied in the multiple comparisons. Relationships between the VAS, SAI, and ICQ points were evaluated with Spearman correlation and partial correlation analyses. The effect of the groups on the VAS, SAI, and ICQ points was evaluated with linear regression analysis using the “enter method”. A value of p<0.05 was accepted as statistically significant.
Approval for the study was granted by the Non-Invasive Clinical Research Ethics Committee at İnönü University, Malatya, Turkey (Decision No: 16, dated: 10/08/2021). Permission to conduct the study was obtained from the institution. Written informed consent was provided by all the patients. All procedures were in compliance with the Helsinki Declaration.
Results
The sociodemographic characteristics were determined to be similar in the intervention group and the control group (Table 1). Evaluation was made of a total of 104 patients, as 53 (51%) patients with a mean age of 59.0±12.5 years in the control group and 51 (49%) with a mean age of 57.9±13.1 years in the intervention group. There was statistically similar age distribution in the 2 groups (p>0.05). Gender distribution was similar in both groups with 32 (60.4%) male patients in the control group and 38 (74.5%) male patients in the intervention group (p>0.05). There were seen to be 48 (90.6%) married patients in the control group and 47 (92.2%) in the intervention group, with no significant difference determined in respect of marital status (p>0.05). The education level of the patients was similar in both groups with 30 (56.6%) patients in the control group and 23 (45.1%) in the intervention group with an education level of primary school (p>0.05). Employment status showed similar distribution in both groups with 37 (69.8%) control group patients and 43 (84.3%) intervention group patients who were not employed (p>0.05). The number of retired patients was 15 (28.3%) in the control group and 19 (37.3%) in the intervention group, and the occupational distribution was similar in the 2 groups (p>0.05). The distribution of social security status was similar in both groups with 35 (66%) patients in the control group and 32 (62.7%) in the intervention group with national insurance coverage (p>0.05).
- Comparisons of the sociodemographic characteristics of the groups.
In the control group, 46 (86.8%) patients and in the intervention group, 45 (88.2%) patients reported an income level less than outgoings, showing similar distribution of income level in both groups (p>0.05). The place of residence was similar in both groups as 26 (49.1%) control group patients and 28 (54.9%) intervention group patients lived in a city (p>0.05). In respect of the people with whom the patient lived, there were no significant difference between the groups as 37 (69.8%) in the control group and 35 (68.6%) in the intervention group lived with their spouse (p>0.05).
In the control group, 13 (24.5%) patients and in the intervention group, 12 (23.5%) patients stated that they were active smokers. Alcohol was consumed by 2 (3.8%) patients in the control group and by 3 (5.9%) patients in the intervention group. There was seen to be similar distribution of smokers and alcohol consumption in both groups (p>0.05).
The number of stents and balloons applied to the patients in the intervention group was statistically significantly greater than in the control group (62.7% versus 35.8%, p=0.010).
The comparisons of the VAS pain values of the groups at 0, 2, and 4 hours are shown in Table 2. The VAS values at 0 hour were statistically significantly higher (p=0.022) and statistically significantly lower at 2 and 4 hours in the intervention group than in the control group (p<0.001). In the within group comparisons, statistically significant differences were determined between the values at 0, 2, and 4 hours in the control group (p<0.001). The lowest VAS value in the control group was at 0 hour and the highest VAS value was at 4 hours. In the intervention group, the VAS values at 2 and 4 hours were statistically significantly lower than the value at 0 hour (p<0.001).
- Comparisons of the pain evaluations at 0, 2, and 4 hours.
No statistically significant difference was determined between the groups in respect of the SAI values at 0 and 4 hours (p>0.05) (Table 3). In the control group, the mean SAI value was 46.0 at 0 hour and 45.3 at 4 hours, and In the intervention group, these values were 45.8 at the 0th hour and 44.1 at the 4th hour. In the comparisons within the groups, there was no significant difference in the SAI values from 0 to 4 hours (p>0.05).
- Comparisons of the SAI and ICQ Points of the groups before and after the procedure.
In the comparisons between the groups of the ICQ values at 0 hour, there was no significant difference (p>0.05). At 4 hours, the ICQ values of the intervention group were significantly higher than those of the control group (p<0.001). In the within group comparisons, the ICQ value at 4 hours was significantly lower than at 0 hour in the control group (p<0.001). The increase in the 4-hour ICQ values of the intervention group was not statistically significant (p>0.05).
The correlations of the values are shown in Table 4. A statistically significant but weak level negative correlation was determined between the VAS values and the ICQ values at 0 hour in both groups (control: r= -0.304, p=0.002; intervention: r= -0.863, p<0.001). A statistically significant strong positive correlation was determined between the VAS values and the SAI values at 4 hours in both groups (r=0.817, p<0.001), and a strong negative correlation between the VAS values and ICQ values (r= -0.863, p<0.001). In the control group at 4 hours, there was determined to be a moderate level positive correlation between the VAS values and the SAI values (r=0.521, p<0.001), and a good level negative correlation between the VAS values and the ICQ values (r= -0.751, p<0.001). In the intervention group at 4 hours, there was determined to be a moderate level positive correlation between the VAS values and the SAI values (r=0.433, p=0.002). In both groups there was found to be a good level negative correlation between the ICQ 0-hour values and the SAI values (r= -0.602, p<0.001). In both groups there was found to be a low level negative correlation between the ICQ 4-hour values and the SAI values (r=-0.381, p<0.001). A statistically significant negative correlation at a good level was determined in the intervention group between the 4-hour ICQ values and the SAI values (r= -0.684, p<0.001). The other correlation coefficients were not determined to be statistically significant (p>0.05) (Table 4).
- Correlations between the VAS, SAI, and ICQ points before and after the procedure.
The results of the linear regression analysis using the Enter method are shown in Table 5. According to the analysis results, the groups explained 82.2% of the VAS values (R2=0.828) (p<0.001) and 91% of the ICQ values (R2=0.917) (p<0.001). As seen in Table 5, the VAS values of the intervention group at 4 hours were 6.00 units lower than those of the control group (p<0.001). The SAI values at 4 hours showed no statistically significant difference between the groups (p>0.05). The ICQ values of the intervention group at 4 hours were 20.49 units higher than those of the control group (p<0.001).
- Linear regression analysis results for the VAS, SAI, and ICQ values at 4 hours.
Discussion
The results of this study showed that the VAS value at 0 hour was statistically significantly higher in the intervention group than in the control group (p=0.022). This higher VAS value at 0 hour in the intervention group was thought to be due to the type of procedure. As the duration of the procedure increases, so does the time spent in the supine position and this can increase the severity of the back pain of the patient.5,24
In this study, the VAS values of the intervention group were lower than those of the control group at 2 and 4 hours (p<0.001). The VAS values of the intervention group were 6.00 points lower than those of the control group (p<0.001). According to these findings, Hypothesis H1= “Patients in the elevated supported supine position group will have a statistically significant reduction in back pain compared to patients in the control group.” was accepted. These data showed that changing patient positions with back support decreased back pain after CAG. There is similar evidence in the literature. Yilmaz et al12 reported that elevating the bedhead of CAG patients to 30° or 45° decreased back pain. Olson25 also reported that elevation of the bedhead after CAG reduced the pain of patients. In a study by Mert et al10 it was determined that the lowest level of back pain occurred when the bedhead was raised to 45-60° after CAG. A modified position was reported to be effective in reducing back pain in another study.24
In the comparisons within the groups in this study, the SAI values at 4 hours were not determined to be different from the values at 0 hours (p>0.05). Anxiety was seen to be at a moderate level at 0 and 4 hours in both groups. According to these findings the H2 hypothesis= “Patients in the elevated supported supine position group will have a statistically significant reduction in anxiety level compared to patients in the control group” was rejected. These results suggested that a modified position alone was not sufficient to reduce anxiety. The anxiety level of patients can be affected by conditions such as the intensive care environment, uncertainty on the current situation, having insufficient flexibility in mobilisation, and dependency in meeting personal needs.26,27 In contrast to the current study findings, Pornratanarangsi et al28 reported that the modified position eliminated back pain and therefore reduced anxiety. In another study, the modified position was also found to reduce anxiety.29 These differences can be attributed to study design, the measurement tools used, the environment in which the research was conducted, and the sample sizes of the studies. Anxiety can cause several complications after CAG and so must be kept under control. There is therefore a need for new applications to be developed with a high level of evidence.30
The results of the current study showed that the mean ICQ points at 4 hours were significantly higher in the intervention group than in the conttrol group (p<0.001). The ICQ points of the intervention group were 20.49 points higher than those of the control group (p<0.001). According to these findings, Hypothesis H3=“Patients in the elevated supported supine position group will have a statistically significant increase in comfort level compared to patients in the control group.” was accepted. Yilmaz et al12 reported that a position change in patients undergoing CAG reduced back pain and increased comfort. In a study of patients undergoing radial and femoral angiography, Çıracı et al30 reported that the comfort of the radial angiography patients was higher. As there is positional freedom in radial angiography, patient comfort has been found to be high.27 Positional comfort is extremely important in respect of the overall patient comfort. From the results of the current study, it was thought that an elevated position with back support to decrease patient pain increased patient comfort.
In the analyses of the current study, the 4-hour VAS values in the control group were determined to be significantly positively correlated with SAI values (r=0.521, p<0.001) and significantly negatively correlated with the ICQ values (r=-0.751, p<0.001). In the intervention group, there was determined to be a significant positive correlation between the 4-hour VAS values and the SAI values (r=0.433, p=0.002). Dağlı et al31 determined a negative correlation between the comfort and anxiety points of patients presenting for CAG. In another study, Çakır et al32 also determined a negative relationship between comfort and anxiety. The findings of the current study are in parallel with the literature. It can be considered that comfort will be increased in patients with pain and anxiety under control.
Study limitations
The first limitation of the study is that more patients in the intervention group had balloons or stents applied to than patients in the control group. The second limitation is that it prolonged the duration of balloon and stent angiography, which was applied to mostly on patients in the intervention group. The third limitation is that angiography studies of all groups were not performed by a single physician.
In conclusion, the results of this study demonstrated that an elevated position with back support reduced the back pain of patients, did not change the anxiety level, and increased comfort. Therefore, it can be recommended that after CAG, an elevated bedhead position and back support can be used to decrease the back pain of patients and increase comfort.
Acknowledgment
The authors gratefully acknowledge Carolinejwalker for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 9, 2024.
- Accepted June 2, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.