


Abstract
Objectives: To assess the clinical course and long-term outcomes of complicated and uncomplicated AM in Saudi Arabia. Acute myocarditis (AM) can have different presentations and outcomes based on different factors, one of which is left ventricular ejection fraction (LVEF).
Methods: Data from 382 patients with suspected AM, admitted between January 2016 and October 2023, were reviewed. Clinical course, in-hospital complications, and all-cause mortality were evaluated in both the acute and follow-up phases. Outcomes were compared between 2 groups: LVEF <50% (n=43); and normal LVEF (≥50% [n=41]) at presentation.
Results: Data from 84 patients (mean [±SD] age, 33.5±10.2 years; 26.2% female) who fulfilled the inclusion criteria were analyzed. The most common symptom was chest pain (83.3%) and 11 (13.1%) patients had fulminant presentation. ST-T changes were found on electrocardiography in 45.2% of patients. The mean LVEF was 46±12.4% at presentation. Patients in the LVEF <50% group were significantly more likely to experience a first-time cardiac-related adverse event (CRAE) (hazard ratio 2.6 [95% confidence interval 1.1–6.2]; p=0.031) with a mean time of 38.8±3.8. The all-cause in-hospital and follow-up mortality rates in the LVEF <50% group were 4.7% (one-half cardiac-related) (p=0.494) and 4.7% (all cardiac-related) (p=0.494), respectively.
Conclusion: Of 84 patients diagnosed with AM, those with LVEF <50% were more likely to experience first-time CRAEs and exhibited low short- and long-term mortality rates.
Myocarditis is an inflammatory condition that affects the heart muscle, primarily impacting young individuals and is often triggered by viral infections, including parvovirus B19, Coxsackie B virus, and coronavirus disease 2019 (COVID-19).1,2 The Global Burden of Disease Report (2019) estimated its prevalence at 6.1 cases per 100,000 people. Globally, the incidence of myocarditis is estimated to range from 10 to 22 cases per 100,000 individuals, with around 1.5 million cases reported worldwide in 2013.3 As highlighted in research by Lampejo et al,1 myocarditis presents with diverse symptoms, the most prevalent being chest pain, which is reported in 85–95% of cases and often requires differentiation from conditions such as acute coronary syndromes or pericarditis. Fever occurs in approximately 65% of patients, while dyspnea, particularly in those with left ventricular dysfunction, is reported in 19–49% of cases. Other symptoms include palpitations, syncope, and fatigue, with flu-like, respiratory, or gastrointestinal prodromal symptoms seen in up to 80% of cases. Severe cases may manifest as ventricular arrhythmias, heart failure (observed in 26%), cardiogenic shock, or cardiac arrest. Additionally, 80% of patients present with elevated inflammatory markers like CRP or ESR, and 26% exhibit left ventricular systolic dysfunction or other complications.1 Myocarditis is classified as acute when symptoms last less than one month, while chronic myocarditis involves symptoms persisting beyond this period. Fulminant myocarditis refers to cases with life-threatening symptoms, such as cardiogenic shock, rapidly progressive acute heart failure, or severe arrhythmias.4 Complications include dilated cardiomyopathy, pericarditis, heart failure, arrhythmias, and cardiac tamponade.5 In Saudi Arabia, research has primarily focused on pediatric myocarditis. For instance, a study by Albuali et al6 reviewed the medical records of 80 pediatric myocarditis patients, highlighting that delayed presentation (defined as occurring more than 72 hours after symptom onset) was associated with increased shock, multisystem organ failure, higher in-hospital mortality, and longer stays in the pediatric intensive care unit. However, limited research exists on myocarditis in adults, particularly within the Saudi population. This retrospective, single-center study therefore aimed to explore the clinical progression and long-term outcomes of myocarditis in Saudi adults.
Methods
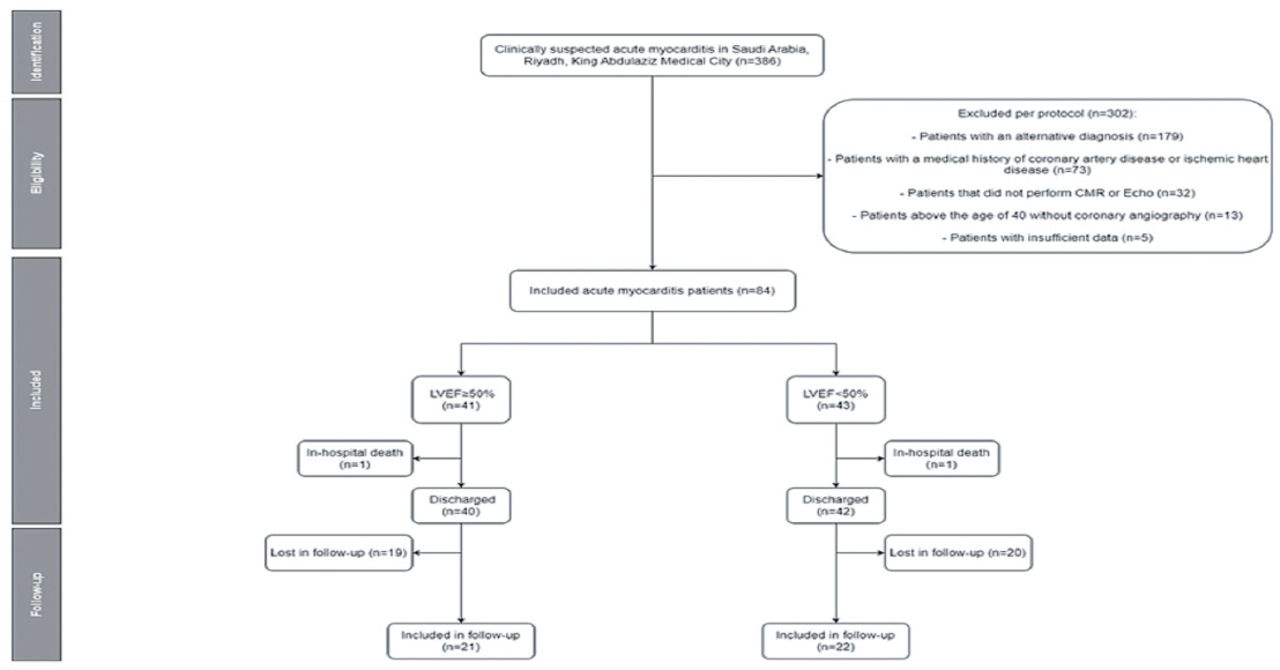
The present investigation was a retrospective case-control of patients diagnosed with AM and admitted to a single tertiary care center between January 2016 and October 2023 in King Abdulaziz Medical City, Riyadh, Saudi Arabia. Data from all patients >18 years of age who presented to the emergency department with clinical manifestations of suspected myocarditis within the previous 4 weeks were included. Patients were identified according to International Classification of Diseases, 10th Revision diagnostic codes (I01.2, I09.0, I40.0-40.9, I41.0) from medical records housed in the hospital. Inclusion criteria were as follows: positive cardiac markers (troponin I, creatine kinase [CK], or creatine kinase-myoglobin binding [CK-MB]); and positive cardiac magnetic resonance (CMR) findings according to the Revised Lake Louise Criteria. The main criteria included myocardial edema on T2-mapping or T2-weighted images and non-ischemic myocardial injury (evidenced by abnormal T1 extracellular volume or late gadolinium enhancement [LGE]). Supportive criteria included pericarditis (evidenced by effusion in cine images or abnormal LGE, T2, or T1 images) and systolic left ventricular dysfunction (evidenced by regional or global wall motion abnormality).7 As per protocol, Patients >40 years of age were required to undergo coronary angiography to rule out coronary artery disease. Patients with a previous diagnosis or evidence of ischemic heart disease or coronary artery disease were excluded. Patients with alternative diagnoses were also excluded (Figure 1). Regarding the main outcome of this study, patients who experienced a first-time, cardiac-related adverse event (CRAE) were assessed. Cardiac-related adverse events included all-cause and cardiac death, heart transplant (Htx), venoarterial extracorporeal membrane oxygenation (VA-ECMO), cardiogenic shock, and new-onset HF. Outcomes were compared between groups with left ventricular ejection fraction (LVEF) <50% versus normal LVEF (≥50%) at presentation. Echocardiography was performed by a cardiology consultant, and LVEF was calculated by a cardiology consultant using Sampson method. During follow-up, CRAE data were extracted from appointments in the medical records for 5 years from admission. The last follow-up appointment was October 2023. This study was approved by the Institutional Review Board Committee of King Abdullah International Medical Research Center and was conducted in strict adherence with the established institutional protocols, national legal obligations, and revised principles outlined in the Declaration of Helsinki. The dataset supporting the information presented in this research article will be made available upon reasonable request to the corresponding author.

- Flowchart of exclusion criteria and follow-up.
The literature search to find prior related research was conducted using 3 databases: web of Science, ScienceDirect, and PubMed. Further searches were done on google scholar using the keywords “myocarditis complications” and “acute myocarditis”, but it was limited to the English language only.
Statistical analysis
Continuous variables are expressed as mean (±standard deviation [SD]) or as median (interquartile range [IQR]) based on the normality of distribution, which was assessed using the Shapiro–Wilk test. The paired Student’s t-test or Wilcoxon matched-pair signed-rank test was used to compare related continuous variables, as appropriate. The unpaired Student’s t-test or Mann–Whitney U test was used to compare independent continuous variables, as appropriate. Categorical variables are expressed as frequency and percentage. Pearson’s chi-squared test or Fisher’s exact test were used for categorical variables, when applicable. Kaplan–Meier curves were assessed using log-rank statistics. Multivariate analysis of CRAEs was performed using Cox regression analysis. Statistical analysis was performed using SPSS Statistics for Windows, version 23.0 (SPSS Inc., Chicago, Ill., USA). All statistical tests were 2-tailed and differences with p<0.05 were considered to be statistically significant.
Results
The mean (± SD) age of patients was 33.5 ± 10.2 years and 26.2% were female. HF (20.2%) and hypertension (16.7%) were the most common comorbidities observed. Chest pain was experienced by 83.3% of patients, while 40.5% experienced dyspnea,, and the mean onset of symptoms was 3.2 ± 3.4 days. Of the patients included, 27.4% tested positive for respiratory tract infections, while 10.7% tested positive for COVID-19. 45.2% of patients had ST-T changes on electrocardiography and only 2.4% had an atrioventricular block. All patients exhibited increased troponin I levels. Also, 76.2% of patients exhibited increase in either CK-MB or CK, while 23.8% exhibited increased BNP. On echocardiography, the mean LVEF was 46 ± 12.4% and 1.2% of patients exhibited pericardial effusion (Table 1).
- Baseline demographics at admission in acute myocarditis patients.
Cardiac-related adverse event
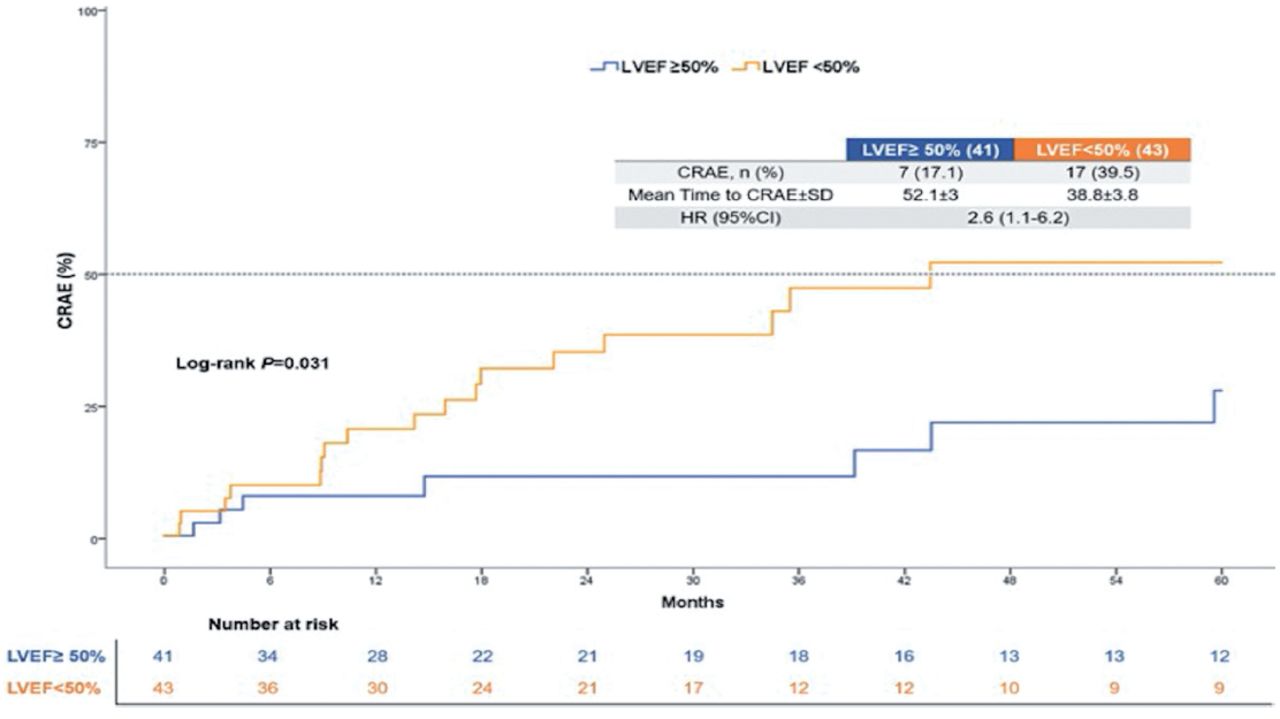
A statistically higher percentage of patients in the LVEF <50% group experienced CRAEs compared with those in the LVEF ≥50% group (39.5% versus 17.1%; hazard ratio [HR] 2.6 [95% confidence interval (CI) 1.1–6.2]; p=0.031). The mean time for CRAEs was found to be 38.8 ± 3.8 for the LVEF <50% group and 52.1 ± 3 for the LVEF ≥50% group (Figure 2). Multivariate analysis revealed that that those in the LVEF <50% group were still more likely to experience CRAEs (HR 3.7 [95% CI 1.4–9.6]; p≤0.01) (Table 2).

- Kaplan Meier curve for cardiac related adverse events.
- Univariate and multivariate analysis of confounding factors.
No statistically significant differences were observed in any of the adverse events between the groups. The in-hospital all-cause mortality rate was 4.7% in the LVEF <50% group, one-half of which were cardiac-related deaths. Htx was not performed in any group during the study period. During the hospital stay, 20.9% of the LVEF <50% group later progressed to cardiogenic shock, while only 4.9% of the LVEF ≥50% group progressed to cardiogenic shock and VA-ECMO was performed only in those in the LVEF <50% group (7%). The mean follow-up duration was 29 ± 22.1 and 39 patients were lost to follow up. All-cause death was experienced by 4.7% in the LVEF <50% group, all of which were cardiac-related.Newly developed HF was observed in 25.6% of the LVEF <50% group, compared to only 7.3% in the LVEF ≥50% group (Table 3).
- Cardiac related adverse events after acute event.
Discussion
In this study, patients presenting with left ventricular ejection fraction (LVEF) below 50% were more likely to experience cardiac-related adverse events (CRAEs) compared to those with LVEF above 50%. Similarly, Younis et al8 (2019) evaluated 322 acute myocarditis (AM) patients and found that LVEF was significantly linked to in-hospital cardiac complications (HR 4.30 [95% CI 1.59–11.49]; p≤0.001). Additionally, Ammirati et al9 reported a higher risk of adverse cardiac events in patients with complicated presentations, such as those with LVEF <50%, compared to uncomplicated cases. In another study, Ammirati et al9 compared 55 patients with fulminant AM to 132 with non-fulminant AM, finding that in-hospital adverse events occurred more frequently in the fulminant group (p≤0.0001).10 Furthermore, data from a 2018 multicenter Lombardy Registry of 443 AM patients indicated that fulminant presentations were associated with more complicated hospital stays (p<0.0001).9 Bohbot et al11 (2022) also demonstrated that reduced LVEF, greater late gadolinium enhancement (LGE), and absence of myocardial edema were strong predictors of early adverse outcomes in AM patients. Lower LVEF and extensive LGE were indicative of severe myocardial damage and dysfunction, correlating with increased risks of both short- and long-term adverse outcomes.
The elevated occurrence of CRAEs in patients with reduced LVEF highlights the critical role of cardiac function impairment in determining outcomes. A lower LVEF results in decreased cardiac output, reduced organ perfusion, and heightened vulnerability to arrhythmias and severe cardiac events. These factors underscore the need for meticulous monitoring and management of patients with reduced LVEF.
The overall in-hospital and follow-up mortality rate for all AM patients in this study was 2.4%, with no heart transplant (HTx) required. Notably, all mortality cases occurred in patients with LVEF <50%. Younis et al8 and Sanguineti et al12 similarly reported no in-hospital or follow-up mortality in their studies. Ammirati et al9 (2018) also reported low in-hospital mortality and HTx rate (3.2%), and a low 5-year mortality and HTx rate (4.1%). Earlier studies, however, documented higher mortality and HTx rates compared to recent findings.13-16 Differences in outcomes between older and newer studies may stem from variations in patient populations, diagnostic criteria, and study designs. Older studies often included smaller sample sizes and relied on endomyocardial biopsy (EMB) or CMR for severe cases, excluding milder clinical presentations.13,15-17 With advancements like high-sensitivity troponin assays, early detection and diagnosis of mild AM cases have become possible, leading to better outcomes in recent studies. Hang et al18 highlighted the importance of comprehensive monitoring and management for patients with low LVEF, as extensive LGE and reduced LVEF strongly predict adverse outcomes, reinforcing the need for timely intervention in high-risk groups.
The increased CRAE incidence in patients with low LVEF underscores the profound effect of impaired cardiac function. Advances in diagnostics and treatments continue to improve the prognosis for AM patients, emphasizing the critical importance of early intervention and individualized care strategies.
Numerous studies have examined myocarditis risk associated with COVID-19 infection and vaccination. Knudsen et al19 (2022) reviewed 29 studies on myocarditis after COVID-19 vaccination, revealing that studies with 4 stratifiers (age, gender, vaccine type, dose) provided incidence rates of 8.1–39 cases per 100,000 males under 40 after a second mRNA vaccine dose, while those with fewer stratifiers reported rates of 0.2–7.8 cases per 100,000. Similarly, the Nordic Cohort Study identified the highest myocarditis risk in males aged 16–24, with 4–7 excess cases per 100,000 for BNT162b2 and 9–28 for mRNA-1273 after the second dose.20 Boehmer et al21 found that COVID-19 infection increased myocarditis risk by 15.7 times compared to non-infected populations, particularly in younger and older age groups. Patone et al22 noted an elevated myocarditis risk post-vaccination but emphasized that it was significantly lower than the risk associated with COVID-19 infection. Lai et al23 observed that vaccine-associated myocarditis had better outcomes compared to viral myocarditis, with lower mortality rates. Voleti et al’s24 meta-analysis highlighted a sevenfold higher myocarditis risk from COVID-19 infection than vaccination. Overall, while young males and individuals with COVID-19 are at increased myocarditis risk, vaccine-related cases typically have a less severe prognosis.
Study limitations
This study was its retrospective design, which may have been a source of potential bias. Because this was a single tertiary care center study in Saudi Arabia, the limited sample size and practice of the center may have affected the outcomes and may not necessarily be representative of populations in different regions. In addition, from March to June 2020, Saudi Arabia underwent several curfews due to the COVID-19 pandemic, affecting access to care centers, which may have caused delayed presentations of AM. Finally, the tertiary center’s database encompasses >6 years, the availability and the use of EMB and CMR likely underwent changes and developments during this time. Also, EMB was not performed as per hospital policy, which limited our discovery of the aetiologies leading to the AM of sample. Despite these limitations, our study’s in-hospital outcomes and long-term mortality rates were found to be consistent with the recent literature and current clinical practice compared with older reports requiring EMB for the diagnosis of AM.
In conclusion, the results of this retrospective study highlighted that patients with LVEF <50% at presentation were at a significantly higher risk for CRAE compared to those with an LVEF ≥50%. Our findings are consistent with those of the existing literature, indicating that a lower LVEF is strongly associated with increased in-hospital cardiac complications and adverse events. This study also observed that all in-hospital and follow-up all-cause mortalities occurred in the LVEF <50% group, reinforcing the critical importance of early and accurate diagnosis. Despite its limitations, including the retrospective design, single-center focus, and potential impact of the COVID-19 pandemic on patient presentation, the outcomes of our study are consistent with recent clinical practices and the literature. These findings highlight the necessity for early identification and intervention in patients with AM particularly those with reduced LVEF to improve short and long-term outcomes.
Acknowledgment
We would like to thank all who took a part in this study. We also acknowledge Editage (Editage.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 23, 2024.
- Accepted December 11, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.



{kind=link}
{kind=link}