


Abstract
Objectives: To evaluatethe effectiveness of social skills training (SST) interventions for children with autism spectrum disorder (ASD).
Methods: A systematic review and meta-analysis were carried out to identify relevant studies published between 2000-2023. The study was conductedin accordance with the PRISMA guidelines. Studies were included if they met the following criteria: randomized controlled trials (RCTs) or quasi-RCTs, participants were children with ASD aged 3-18 years, SST interventions were delivered individually or in groups, and social skills were assessed using standardized measures. Effect sizes were calculated using Cohen’s d, and meta-analyses were carried out using a random-effects model.
Results: A total of 17 studies were included in the meta-analysis. The overall effect size for SST interventions was 0.28-0.60 (95% confidence interval: [0.23-0.41]), indicating a small to moderate effect. Social skills training interventions were effective in improving a range of social skills, including social communication, reciprocity, and joint attention.
Conclusion: Social skills training interventions demonstrate modest to moderate effectiveness in improving social skills in children with ASD, with outcomes varying depending on intervention type, participant characteristics, and implementation fidelity. While SST interventions offer potential benefits, they should be considered as one component of a broader, individualized treatment plan for children with ASD, rather than a standalone solution.
PROSPERO No. ID: CRD42024578682
Autism spectrum disorders (ASDs) are characterized by a range of behavioral difficulties, including considerable impairments in social interaction and communication.1 Autism spectrum disorder is a significant neurodevelopmental disorder characterized by restricted and repetitive patterns of behavior, interests, or activities, as well as difficulties with social communication and interaction.2 Children with ASD often struggle with forming and maintaining friendships, understanding and reacting to social cues, and participating in social activities. These social challenges can considerably impact a child’s quality of life, academic performance, and social (emotional well-being).3 Children with ASD can acquire essential social skills for more effective interactions through social skills training (SST), which is a type of intervention. While the approach and content of SST programs can differ, they typically focus on teaching skills such as conversation and problem-solving.
Social skills are the practical abilities in interpersonal interactions that allow a child to communicate effectively, both verbally and nonverbally, and adjust to their environment.4 Social skills training is a therapeutic method designed to systematically teach individuals with ASD essential skills for managing social interactions. This evidence-based intervention addresses core social challenges associated with ASD using techniques based on cognitive - behavioral principles. Social skills training involves explicit instruction in specific social skills, such as nonverbal communication, conversational abilities, perspective-taking, and emotional regulation. The approach is structured and systematic, using methods such as modeling, role-playing, and feedback to improve skill generalization and retention. It can be adapted to individual or group settings and implemented across clinical, school, or community environments.5 Additionally, SST programs can differ in duration and intensity, ranging from brief interventions to more comprehensive, long-term approaches. The primary aim of SST is to improve social functioning and enhance the quality of life for individuals with ASD by providing them with the tools needed to form and sustain meaningful social relationships.6
There are various forms of SST, such as group-based SST (GSST) and individual SST. Group-based SST programs usually involve a group of children with ASD who regularly meet to learn and practice social skills.7 Individual SST programs are designed to address the specific needs of each child and can be delivered by therapists, teachers, or parents. Kjobli et al8 found that individual SST alone did not result in a reduction of problematic behaviors in children. They suggested that addressing behavioral issues required more comprehensive approaches beyond just individual SST. Social skills training programs can be implemented in various settings, including schools, clinics, and community centers. Typically lasting several weeks or months, these programs often include didactic instruction, role-playing, and practical application of social skills. Social skills training therapies frequently involve practicing these skills in diverse contexts, such as interactions with peers, family members, and teachers. In a randomized controlled trial, Dekker et al9 found that despite increased involvement from both teachers and parents, there was no additional benefit compared to SST delivered to children alone, as reported by parents. Moreover, they observed no considerable improvement or decline in outcomes after a 6-month training period.6,9 A recent meta-analysis by Soares et al10 revealed a substantial effect size, ranging from medium to large, for both face-to-face and behavioral intervention technologies (BIT) in SST aimed at improving social skills in children and adolescents. Notably, no considerable differences were found between the 2 intervention modes. These findings suggest that technology platforms could be a promising method for delivering SST to children and young adults with ASD.10 In their randomized controlled trial, Choque et al11 found that social skills group training (SSGT) was a safe and practical intervention for children and adolescents with ASD who were undergoing regular mental health treatments. However, the inconsistent results underscore the need for continued efforts to refine and improve SSGT beyond current standards.
However, the absence of extensive group studies has led to criticism regarding the empirical validity of SST for individuals with ASD in several research studies. A systematic review and meta-analysis can be useful in providing an overview of the literature regarding the efficacy of SST therapy for children diagnosed with ASD. The purpose of this review and meta-analysis is to appraise the quality of the evidence offered in the included studies and to determine how effectively SST therapies work in enhancing social interaction and communication skills in children with ASD. The recommended reporting elements for systematic reviews and meta-analyses (PRISMA) guidelines will be followed in this systematic review and meta-analysis. The results will give doctors, researchers, and legislators important information on how well SST therapy works for people with ASD.
Rationale for systematic review and meta-analysis
Social skills training is one of the most widely used interventions for children with ASD. However, there is conflicting information regarding its effectiveness in managing ASD therapeutically. This systematic review aims to provide a comprehensive approach to evaluating the efficacy of SST therapies for children with ASD. Carrying out a systematic review and meta-analysis is essential owing to the lack of consensus on methodology, participant characteristics, and outcome measures in the existing research on SST therapies. Drawing clear and concise conclusions regarding the efficacy of SST therapies from study results can be challenging. Additionally, a systematic review and meta-analysis can identify the pediatric characteristics that are most likely to benefit from SST interventions, as well as the most effective types of SST therapies. Clinicians can use this information to make informed decisions on which SST therapy to recommend for their patients.
Aims and objectives
To identify and evaluate the effectiveness of SST interventions in enhancing social interaction and communication skills in children diagnosed with ASD and to assess the quality of evidence presented in the studies included in the meta-analysis.
Methods
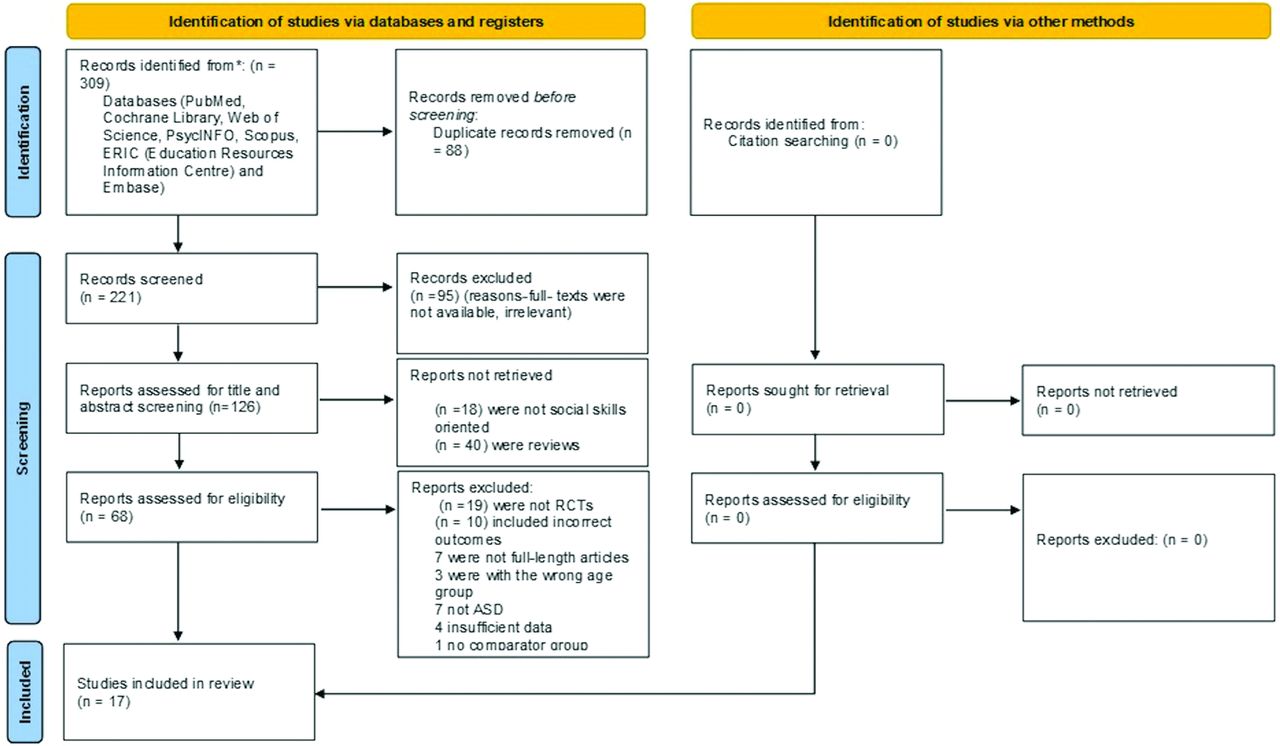
The study was carried out in accordance with the PRISMA criteria. The methodology summary, including the number of studies from various databases, the search strategy used for article selection, and the reasons for study exclusion, is depicted in the PRISMA flowchart (Figure 1).

- The preferred reporting items for systematic reviews and meta-analyses flowchart. RCTs: randomized controlled trials, ASD: Autism spectrum disorder
Data collection and search methodology
The first step in assessing the evidence for social interaction therapy for adolescents with ASD in educational settings involved a comprehensive search of published studies from 2013 onward. This search included multiple electronic databases such as PubMed, Cochrane Library, PsycINFO, Embase, Scopus, Web of Science, and Education Resources Information Center (ERIC). The goal was to identify relevant studies published up to September 2023. The search strategy used a combination of keywords and controlled vocabulary terms related to “autism spectrum disorder”, “social skills training”, “communication skills”, “social interaction”, “randomized controlled trials”, “children”, and “intervention effectiveness,” with Boolean operators (AND, OR) used to refine the queries.
Inclusion and exclusion criteria
This systematic review included research published in peer-reviewed journals that focused on interventions targeting SST in children with ASD. The inclusion criteria encompassed randomized controlled trials (RCTs) or quasi-experimental studies with comparison groups that provided adequate data for effect size calculation. The search used both free text and controlled vocabulary, examining titles and abstracts with Boolean expressions. The review considered both published and unpublished studies, such as peer-reviewed journal articles. To minimize publication bias, the review also considered conference proceedings, dissertations, and reports. Studies were excluded if they were non-randomized, published in languages other than English, evaluated interventions other than SST, lacked a comparison group, did not report outcome measures related to improvements in social interaction and communication skills, did not focus specifically on SST interventions, or had insufficient data or inadequate study design.
Study screening and data extraction
Articles with unrelated titles were disqualified during the initial round of the research selection process. The entire texts and abstracts that met the inclusion criteria were examined in the second phase. To arrange, evaluate, and find duplicate entries in the titles and abstracts, Endnote X8 was utilized. To guarantee excellent findings, a double screening procedure was employed: one review was carried out for titles and abstracts, and another for entire texts. Data on the study period, design, sample size, region, intervention and control groups, gender, and age distribution were gathered using a prototype data-extraction sheet. The data extraction was carried out by 2 separate investigators, and disagreements were settled by consensus rather than using presumptions or oversimplifications.
Quality assessment
For every study, an independent risk of bias evaluation was carried out by 2 reviewers. Using the Cochrane risk of bias tool for RCTs, we evaluated the risk of bias in the included studies.12 By detecting potential biases in study design and reporting, this technology promotes evidence-based decision-making and guarantees transparency and reproducibility. Funnel plots and statistical tests (like Egger’s test) were employed to evaluate publication bias and look for any indications of selective reporting.
Statistical analysis
R software 4.2.2 was used to carry out statistical analysis. For binary outcomes, risk ratios (RR) with 95% confidence intervals (CI) were computed; for continuous outcomes, mean differences ± standard deviation (SD) with a 95% CI were used for assessment. The Cochrane Q p-value and I2 statistic were used to assess heterogeneity across studies by utilizing both fixed-effects and random-effects models. Using Egger’s regression test and funnel plots, publication bias was investigated. For every research that was considered, effect sizes were computed to determine how much the intervention improved social skills.
Ethical considerations
Because this meta-analysis involves the synthesis of existing data from published studies, ethical approval was not required.
Results
The meta-analysis included 17 studies exploring various interventions designed to enhance social skills in children with ASD. These studies encompassed a wide array of interventions, sample sizes, age groups, and durations, offering a thorough overview of the current literature in this area.
Participant information, including age, gender, ASD diagnostic criteria, and relevant baseline characteristics, was collected. Sample sizes were recorded to evaluate their adequacy for meaningful analysis, noting the total number of participants in both intervention and control groups, along with demographic details impacting SST outcomes (Table 1).
- Baseline characteristics of the included studies.
The diverse designs and focus areas of the studies highlighted the variety of SST programs available for children with ASD, including group-based SST, individual SST, and hybrid formats combining both approaches. Some programs were delivered in clinical settings, while others took place in schools or community centers, each with different levels of involvement from parents, teachers, or peers. Furthermore, SST programs varied in intensity and duration, from short-term interventions lasting a few weeks to long-term programs extending several months.
Outcome measures
Information on both primary and secondary outcome measures was carefully retrieved, including pre- and post-intervention scores for each study group. The extracted data, detailed in Table 2, offers a thorough overview of interventions, control conditions, and outcomes across 17 studies. This summary highlights the crucial role of treatment in enhancing social skills and underscores its importance in the examined research context.
- Outcome measures of included studies.
Meta-analysis of the social responsiveness scale
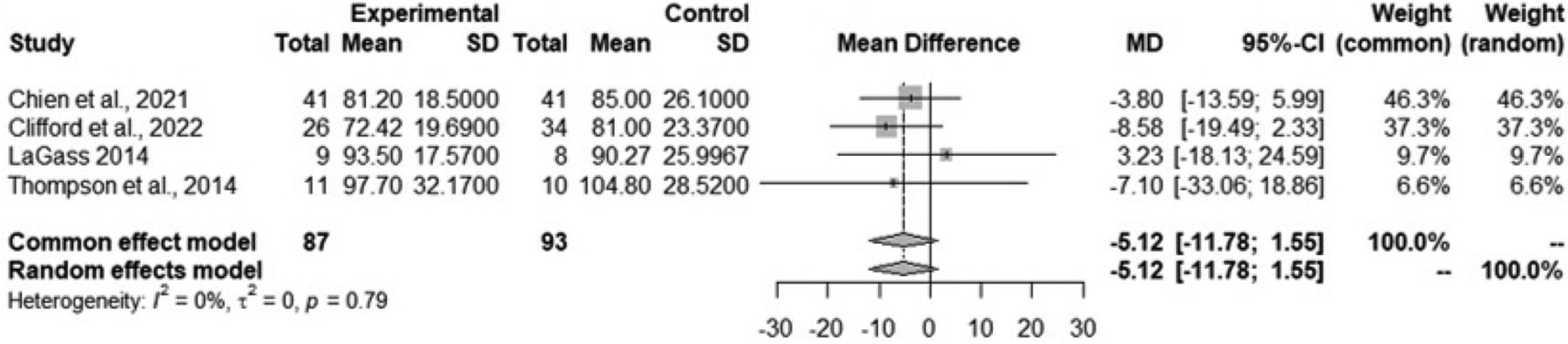
Four studies assessed the social responsiveness scale (SRS), and we combined their results through a meta-analysis to illustrate the overall effect sizes and emphasize the value of using the SRS in our analysis. The SRS is extensively used to evaluate social functioning and behavior, especially in individuals with ASD. As a quantitative measure, it assesses social communication, reciprocal social behavior, and stereotypical behaviors. The SRS is an essential tool in both clinical and research settings, providing a standardized approach to quantifying and analyzing social responsiveness.
The meta-analysis examined a continuous outcome measure, specifically the mean difference (MD) between treatment and control groups. The combined data, analyzed using both common effect and random effects models, yielded an MD of -5.1175, with a 95% CI: (-11.7830, 1.5480). However, the p-value of 0.1324 was not statistically significant, suggesting no meaningful difference between the treatment and control groups (Figure 2).

Assessments of heterogeneity showed a t2 estimate of 0, indicating no observed variability among the studies. The I2 value of 0.0% confirmed the absence of significant inconsistency, and the p-value for the heterogeneity test (Q-test) was 0.7853, which is not statistically significant. This supports the notion of homogeneity across the studies. Although the combined effect size did not achieve statistical significance, the detailed analysis of heterogeneity and consistency provides important context for interpreting the overall findings (Figure 2).
Publication bias
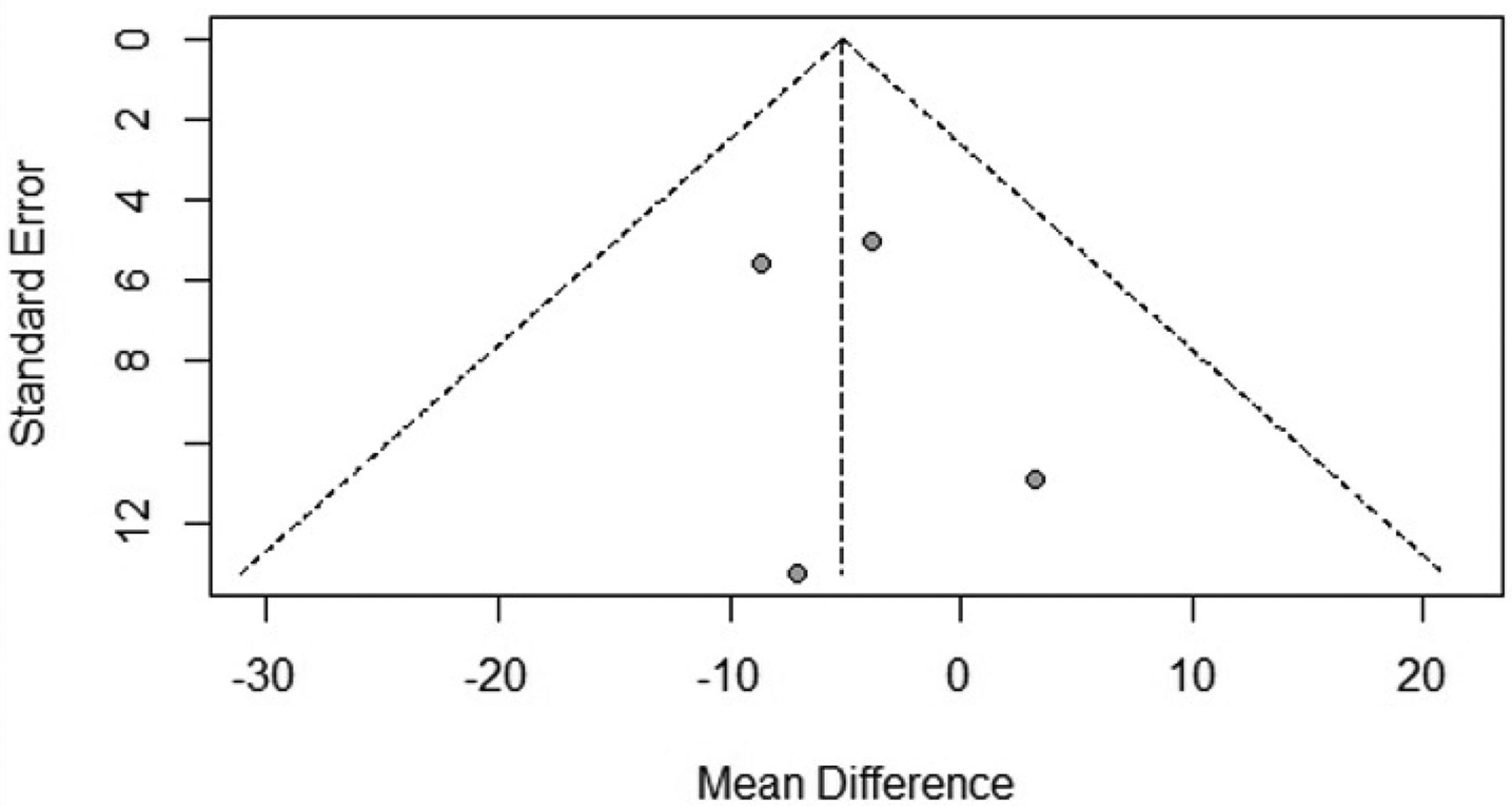
Our meta-analysis’s regression test for funnel plot asymmetry produced a p-value of 0.7250 using a mixed-effects meta-regression model with the standard error as the predictor. This non-significant p-value shows that there may not be a major publication bias associated with the standard error, suggesting that there is not enough data to reject the null hypothesis.
The limit estimate, which assesses potential bias as the standard error approaches zero, is -8.1508 with a CI: (-26.3187, 10.0170). Although this estimate suggests a potential bias toward smaller studies, the wide confidence interval underscores the uncertainty associated with this estimate (Figure 3).

Quality assessment
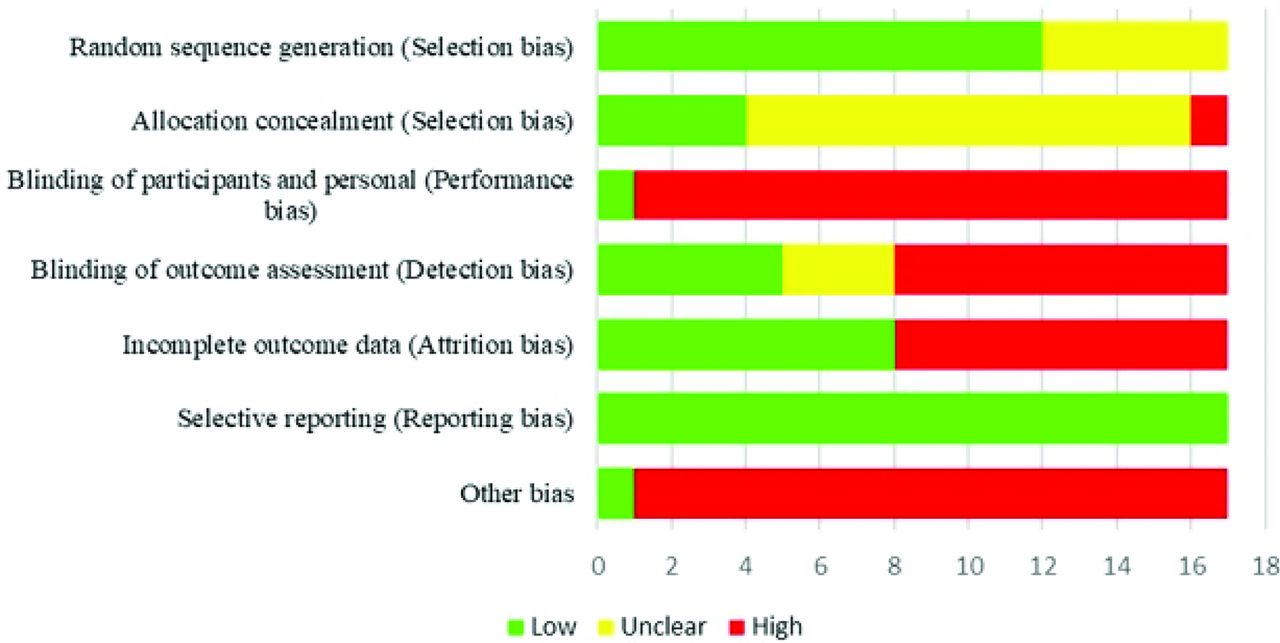
A thorough evaluation of the bias risk for each study that was a part of our systematic review and meta-analysis is shown in Figure 4. Several bias categories, such as reporting bias, attrition bias, detection bias, performance bias, and selection bias, are depicted in this visual summary. The evaluation of bias across the 17 studies in the systematic review and meta-analysis reveals varying levels of methodological rigor. High risks are consistently identified in categories such as blinding of participants and personnel, blinding of outcome assessment, and other biases. These findings highlight the need for cautious interpretation because such biases can considerably affect the validity and reliability of study outcomes. Researchers and practitioners should consider these methodological limitations when applying the results to inform decisions or interventions related to SST in children with ASD. A nuanced understanding of these biases is essential for accurately assessing intervention effectiveness and guiding future research in this area (Table 3).

- Risk of bais assessment of all included studies.
- Cochrane risk of bias assessment for included studies.
Discussion
This review offers a comprehensive and up-to-date assessment of the effectiveness of SST therapies for children with ASD. The findings are consistent with other similar studies, which have shown that SST can be an effective intervention for improving social skills in children with ASD. The current meta-analysis included 17 studies that explored various interventions aimed at enhancing social skills in these children. The results suggest that SST therapies are beneficial for developing social skills in children with ASD.
The meta-analysis findings suggest no considerable difference between the treatment and control groups in SRS, as indicated by a p-value of 0.1324. Heterogeneity analysis shows consistency across studies, with a p-value of 0.7853. Additionally, the assessment for publication bias reveals no strong evidence of bias, with a p-value of 0.7250. However, the quality assessment identified varying levels of methodological rigor, particularly concerning blinding procedures. Therefore, while the results do not show a significant difference between groups, the variability in methodological quality underscores the need for careful interpretation and consideration of potential biases in future research. A number of previous studies have shown that SST can be effective in improving social skills, communication skills, and behavioral issues in children with ASD. These studies included a meta-analysis by Soares et al,10 their results highlight SST as an important intervention for children with ASD. Both studies, including the current meta-analysis, agree that SST interventions effectively improve social skills in individuals with ASD. While our meta-analysis encompasses a wider range of SST interventions, the Soares et al10 meta-analysis focuses specifically on face-to-face SST (F2F-SST) and behavioral intervention technologies SST (BITs-SST). Notably, Soares et al10 suggest that BITs-SST may be as effective as F2F-SST, proposing it as a viable alternative for delivering SST to individuals with ASD. Differences in effect sizes between the 2 analyses may be attributed to variations in studied populations or methodologies. Our meta-analysis, with its inclusion of a larger number of studies, provides broader generalizability of the findings to a wider population of children with ASD. The common incorporation of BITs-SST in both meta-analyses underscores the promise of these interventions as a novel and effective approach for delivering SST to children with ASD.
Another study by Dekker et al,6 supported by its use of a large sample size and follow-up measures in an RCT, provides strong evidence supporting the effectiveness of involving parents and teachers. However, our meta-analysis provides a more comprehensive overview of SST interventions by encompassing a wider array of intervention types.6
This meta-analysis provides a modest but important body of evidence on the effectiveness of SST interventions for enhancing social skills in children with ASD, with varying degrees of success depending on the intervention type and study design. In contrast, the study by Russo-Ponsaran et al31 examine a novel tool for testing special incidence portion (SIP) skills in both ASD and non-ASD populations using the virtual environment for social information processing (VESIPTM). The VESIPTM is an simulation-based evaluation that immerses youngsters in social decision-making scenarios. While the Russo-Ponsaran et al31 study presents preliminary evidence on the potential value of VESIPTM as an evaluation instrument for SIP skills in children, regardless of ASD status, our meta-analysis provides a comprehensive summary of SST intervention effectiveness across diverse studies. In summary, our review provides comprehensive evidence regarding the effectiveness of SST interventions in improving social skills among children with ASD. In contrast, the Shuai et al32 study protocol outlines a systematic review and meta-analysis designed to specifically evaluate the effectiveness and safety of social skills interventions for children with ASD. While our review provides a comprehensive overview of SST intervention effectiveness across multiple studies, the Shuai et al32 protocol, which has not yet been carried out, does not currently provide any findings.
The study protocol by Chen et al33 details a systematic review and meta-analysis specifically designed to explore the effectiveness of social skills (SS) interventions for children and adolescents with ASD. In contrast, our meta-analysis provides a comprehensive overview of the effectiveness of SST interventions across various studies. It is important to note that the Chen et al33 study protocol has not yet been carried out; thus, its findings are not available, we have only referred these protocols to gain insights into the methodological approach for evaluating social skills interventions.
Additionally, while the Chen et al33 protocol focuses specifically on SS interventions (a subset of SST interventions) its planned assessment will cover behavior, social skills, and communication effectiveness. However, our meta-analysis primarily focuses on social skills.
The study by Tachibana et al34 provides detailed insights into the effectiveness of different SST interventions specifically designed for preschool-aged children with ASD. Their research highlights statistically significant improvements in parental synchronization and the reciprocity of social interactions, suggesting these areas as potentially valuable targets for therapies aimed at preschool-aged children with ASD. Tachibana et al’s34 study contributes more specific evidence regarding the efficacy of both individual and group interventions for this age group. In contrast, our meta-analysis provides a more comprehensive overview, evaluating the effectiveness of SST interventions across a range of age groups and various intervention types.
An intriguing study by Freitag et al,7,35 provides detailed evidence of the efficacy of comprehensive developmental interventions and low-intensity training targeting parental synchrony and child reciprocity. In contrast, our systematic overview of SST intervention effectiveness across various age groups and types. Overall, our meta-analysis offers an extensive overview of SST interventions for improving social skills in children with ASD. The findings suggest that SST interventions can improve various social skills, including social communication, reciprocity, and joint attention.
Nonetheless, the majority of the impact sizes were modest to moderate, suggesting that SST therapies have to be regarded as a single element of an all-encompassing therapy strategy for kids with ASD. The precise type of intervention, participant characteristics, and implementation fidelity can all affect how effective SST therapies are. Future studies ought to concentrate on assessing the efficacy of various SST therapies for kids with ASD and investigating their long-term consequences. To better understand how SST therapies function, it’s also critical to look into their mechanisms of action.
Practical implications
The findings of this meta-analysis have important implications for clinicians, educators, and families of children with ASD: I) clinicians: SST interventions demonstrate modest to moderate effectiveness and should be considered as one component of a broader treatment plan for children with ASD. Tailoring SST interventions to individual needs, carefully monitoring progress, and addressing potential variability in outcomes are critical to achieving meaningful improvements in social skills; II) educators: integrating evidence-based SST principles into classroom settings can provide children with ASD opportunities to practice and generalize social skills. Recognizing the variability in the effectiveness of these interventions, educators should provide individualized accommodations and support while fostering inclusive social interactions; and III) Families play a key role in supporting their child’s social development. Actively participating in SST interventions, reinforcing learned skills at home, and maintaining communication with clinicians and educators can enhance the generalization of skills. However, families should remain aware that outcomes may vary based on factors such as the child’s individual characteristics and the consistency of intervention implementation.
While SST interventions show promise in improving specific areas of social functioning (namely, social communication and reciprocity), their overall impact is modest and context dependent. Effectiveness may vary due to factors such as the child’s age, severity of ASD symptoms, intervention type, and implementation fidelity. It is crucial to view SST as part of a comprehensive, individualized approach rather than a standalone solution.
Implications for future research
Future research must concentrate on several critical variables to enhance the comprehension and efficacy of SST interventions for children with ASD. Longitudinal studies are essential to assess the lasting impacts of SST therapies on social skills, adaptive behaviors, and quality of life. Furthermore, examining early intervention with SST and its prospective long-term advantages is essential. Research must investigate the fundamental mechanisms by which SST therapies enhance social skills, examining cognitive, behavioural, and neurological aspects that impact therapy outcomes.
Recognizing critical aspects that influence the efficacy of SST therapies, such as age, severity of ASD symptoms, cognitive capabilities, and motivation, will facilitate the creation of customized SST programs designed to meet individual requirements. It is crucial to ascertain the ideal intensity and duration of SST interventions to maximize outcomes and to evaluate the efficacy of various delivery modes, including individual, group, and hybrid approaches. The advancement of ways to facilitate the generalization and maintenance of social skills acquired in therapeutic environments to real-world contexts, as well as investigating the impact of parent and teacher training on promoting skill generalization, is essential.
Evaluating the effectiveness of technology-driven social skills training (SST) interventions, such as virtual reality and teletherapy, in improving social competencies, as well as exploring the potential of technology to enhance the delivery and customisation of SST, are essential areas for future research. Moreover, it is essential to develop culturally attuned SST therapies appropriate for patients from diverse backgrounds and to adapt these interventions to address linguistic and cultural barriers in subsequent research. By addressing these research queries, future studies can improve and optimise SST therapies to better the social outcomes of children with ASD.
Study limitations
This comprehensive review and meta-analysis offer limited evidence that SST therapies may positively influence the social skills of children with ASD. The results demonstrate small to moderate impact sizes, indicating that SST interventions may enhance aspects of social functioning, including social communication, reciprocity, and collaborative attention. Nonetheless, the overall impact sizes were not statistically significant across all metrics, including the social responsiveness scale, underscoring diversity in results.
Additional study is required to investigate the reasons influencing this variability, such as the type of intervention, participant characteristics (namely, age and severity of ASD), and implementation fidelity.
In conclusion, longitudinal studies are crucial for assessing the enduring benefits of SST and the transfer of acquired abilities to practical environments. Determining the most efficacious strategies for various subgroups of children with ASD will enhance and optimise these interventions within comprehensive treatment regimens.
Acknowledgment
The authors gratefully acknowledge Falcon Scientific Editing (https://falconediting.com) for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 29, 2024.
- Accepted February 12, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.