


ABSTRACT
Objectives: To investigate the effects of prolonged air travel on sinonasal symptoms among aircrew members.
Methods: This study was carried out among airline aircrew members over 4 months, between May 2023 and August 2023. The collected data encompassed demographic and clinical characteristics, including age, gender, and a history of sinus, nasal, or ear surgery. A validated sino-nasal outcome test-22 data collection sheet to measure the presence of sinonasal symptoms was carried out.
Results: Of the 184 aircrew members, 81% were male and 34.8% were aged 20-30 years. Sinonasal symptoms after the flights were reported by 68.5% of participants. Symptom prevalence varied significantly based on factors such as being a flight attendant, experiencing symptoms during flights, symptoms affecting job performance, altering trips due to recurring symptoms, long flight durations, use of medications, and a history of sinus, nasal, or ear surgery. Multivariate regression analysis identified post-flight or in-flight nasal, sinus, or ear problems, symptoms affecting job performance, and previous sinus, nasal, or ear surgery as significant independent predictors of sinonasal symptoms.
Conclusion: Over two-thirds of airline crew members may experience sinonasal symptoms after prolonged air travel. Flight attendants with a history of nasal, or ear surgery and those with longer flight durations were more likely to experience sinonasal symptoms. Larger observational studies are required to further clarify the prevalence and contributing factors of sinonasal symptoms among aircrew members.
Modern commercial airplanes can travel long distances without frequent refueling or short stopovers. According to the World Health Organization (WHO), air travelers may encounter specific health problems owing to several aviation factors, particularly on long-haul flights.1 Traveling by air can cause various health issues, especially in those with pre-existing medical conditions. Disorders that air passengers may experience range from mild to severe respiratory, cardiovascular, and neurological symptoms.2
Sinonasal symptoms are among the most common health issues experienced by air transport travelers. These occur due to changes in air pressure, low cabin humidity, and potential exposure to allergens or respiratory infections.3 Sinonasal disorders, including allergic rhinitis and rhinosinusitis, are frequent respiratory illnesses affecting all age groups. Symptoms range from simple mild stuffy nose or nasal congestion, facial pain, and feelings of pressure, to more severe issues such as fever, headache, loss of smell, ear pain, and cough.4,5 Air travelers, particularly aircrew members, are at a higher risk of such medical conditions, which can progress to sinus barotrauma. This condition involves tissue injury in the lining of the sinuses caused by rapid changes in the barometric pressure between the surrounding atmosphere and intranasal sinuses during ascent and descent, often due to temporary or persistent occlusion of the sinus ostium.6,7 There is growing evidence that mid-to long-duration flights may increase the risk of sinonasal disorders.
Traveling by air creates a unique environment for travelers. Changes in atmospheric conditions during flights can trigger physiological responses that pose certain health risks to both aircrew members and passengers.8 One of the most common health issues experienced during air flights is sinonasal disorders. Aircrews and passengers traveling on mid to long-range flights are often at higher risk of developing sinonasal symptoms.9 A study by Alzahrani et al,10 found that longer flight durations, especially exceeding 12 hours of flying time per week, significantly increase the risk of developing sinonasal disease. Similarly, Shargorodsky et al11 reported a possible association between the frequency of air travel and the development of sinonasal symptoms such as nasal discharge, sneezing, cough, and feeling of facial pain and pressure. Sinonasal disorders have significant implications on the overall health and well-being of air travelers, negatively impacting their comfort and overall flight experience.12 One of the potential complications of sinonasal symptoms for frequent air travelers is sinus barotrauma. In a cross-sectional survey by Lindfors et al,13 more than 60% of the aircrew members reported experiencing sinus barotrauma during flights. Several studies have associated severe headaches during air travel with sinus barotrauma, particularly during descent or landing. The intensity of this pain has led some travelers to develop anxiety or fear of flying.14-16 Weber et al17 observed that persistent sinonasal disease among aircrews may render them “unfit” for work due to the risk of sinus barotrauma. Managing sinonasal symptoms before flights is vital to prevent sinus barotrauma risk. Some effective managements include medications for symptom relief, such as nasal decongestants, antihistamines, and oral or topical steroids.18,19 Non-pharmacological interventions including relaxation techniques, hydration, chewing gum, the Valsalva maneuver, and applying pressure, or massaging painful areas, can also provide relief.16 For air travelers suffering from advanced stages of sinonasal disease, Weitzel et al20 recommended functional endoscopic sinus surgery. Despite the prevalence of sinonasal symptoms, the effects of prolonged air travel on the sinonasal conditions of aircrew members remain underexplored. Accordingly, this study aimed to assess the effects of prolonged air travel on sinonasal symptoms among aircrew members.
Methods
This cross-sectional study was carried out over 4 months, from May 2023 to August 2023, involving aircrew members from Saudi-based airlines. using a convenience sampling method. The data collection included demographic characteristics, smoking status, flying hours, history of sinonasal surgery, medical condition, experience of sinonasal symptoms, and scores from the sino-nasal outcome test 22 (SNOT-22) scale.21 The sample size was estimated through the Raosoft sample size calculator (Raosoft.com, 2015; Sample Size Calculator by Raosoft, Inc.), applying a 5% margin of error and a 95% confidence interval (CI), based on an estimated population of 1,000 aircrew members. The resulting sample size was 278. Eligible participants were aircrew members aged 20-60 years, while those younger than 20, older than 60, and non-aircrew members were excluded.
Inclusion criteria included: I) active aircrew members employed by Saudi-based airlines; II) individuals aged between 20-60 years; and III) individuals who provided verbal consent for participation. The exclusion criteria included: I) individuals younger than 20 or older than 60 years; and II) participants who declined to provide verbal consent.
The center’s ethics committee approved the study protocol, and participants provided verbal consent prior to the interviews. The study is according to principles of Helsinki Declaration. Participation was entirely voluntary, and individuals had the right to withdraw at any time. To ensure confidentiality, personal information was anonymized in compliance with ethical guidelines.
Data were collected based on medical history. The collected data were tabulated and cleaned before being sent to a biostatistician for subsequent analysis. The collected data were stored on a protected PC to maintain confidentiality.
The sinonasal symptoms experienced by the aircrew members were assessed using the SNOT-22 scale.21 The SNOT-22 is a well-validated, disease-specific tool that encompasses rhinologic symptoms with overall health aspects, including psychological factors. It is widely recognized as the most appropriate patient-reported outcome measure for assessing individuals with chronic rhinosinusitis.23 The SNOT-22 was stratified into 3 levels according to score: a score ranging from 8-20 is classified as mild, 2-50 as moderate, and above 50 as severe.24 A score above 7 points indicates the presence of sinonasal symptoms.25 The reliability of SNOT-22 in this study was 0.977 or 97.7%, indicating excellent internal consistency.
Statistical analysis
Descriptive analysis of metric variables was carried out using standard deviation (SD) and mean, while categorical variables were presented as frequencies and proportions (%). To identify independent predictors of sinonasal symptoms, both univariate and multivariate analyses were carried out. A p-value of less than 0.05 was used to define statistical significance. Data analysis was carried out using the Statistical Package for the Social Sciences, version 21.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 184 aircrew members completed the survey (response rate: 66.2%). Table 1 presents an overview of the participants’ demographic and clinical characteristics. Over one-third (34.8%) were in the 20-30 age group, with males being dominant (81%). Approximately 34.8% of participants were pilots. The prevalence of nasal, sinus, or ear problems after air travel was 58.7%. Among these, 21.3% experienced nose and ear problems after the flight, lasting for less than a day (39.8%). Sinonasal symptoms affected job performance in 44% of aircrew members, and 25.5% had to cancel or change their trip because of recurring symptoms. Of the respondents, 33.2% had more than 12 hours of air travel per week. Allergies were reported by 26.1% of participants, smoking by 39.1%, previous sinonasal surgery by 17.9%, ear surgery by 20.1%, and a history of head, face, or nose injuries by 12%. Additionally, 27.2% of participants were currently taking medication.
- Demographic and clinical characteristics of aircrew members (N=184).
Table 2 provides descriptive statistics of sinonasal symptoms, with the overall mean SNOT-22 score recorded at 30.1±28.9. Respondents classified as having mild symptoms made up 19%, those with moderate symptoms accounted for 25.5%, and those with severe symptoms comprised 23.9%. The prevalence of sinonasal symptoms based on the SNOT-22 criteria was 68.5%.
- Descriptive statistics of sinonasal symptoms using the sino-nasal outcome test-22 (N=184).
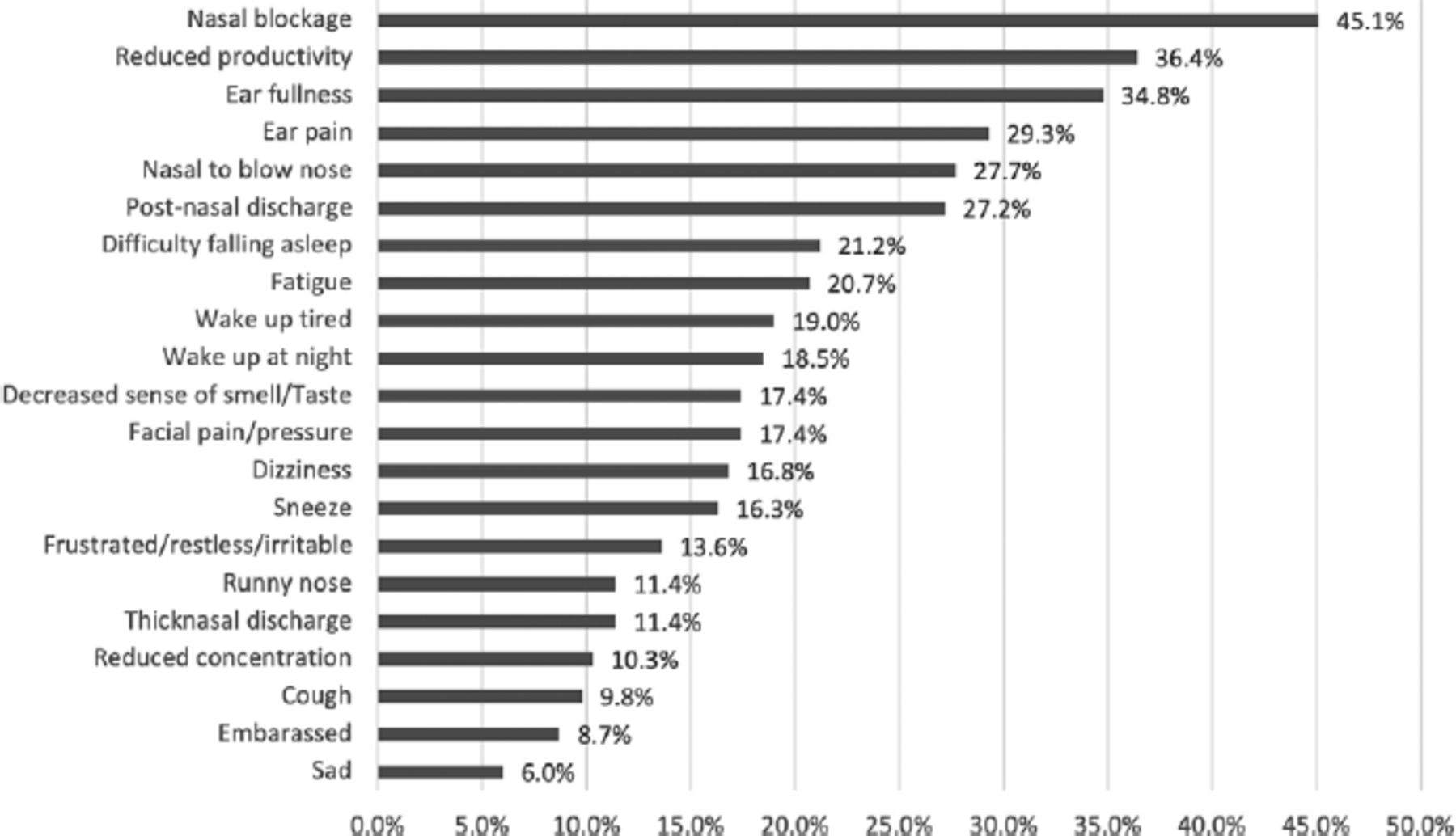
Figure 1 shows that the 5 most important symptoms affecting health were nasal blockage (45.1%), reduced productivity (36.4%), ear fullness (34.8%), ear pain (29.3%), and a nasal to blow the nose (27.7%).

- The most important symptoms affecting health.
Univariate analysis identified several factors significantly associated with the presence of sinonasal symptoms. Flight attendants (X2=6.736; p=0.034), those reporting nasal, sinus, or ear problems after or during the flight (X2=26.731; p<0.001), symptoms affecting job performance (X2=31.407; p<0.001), trip cancellations or changes due to recurring symptoms (X2=15.485; p<0.002), long air travel duration per week (X2=7.833; p=0.005), history of sinus, nasal, or ear surgery (X2=7.012; p=0.008) and use of medication (X2=4.222; p=0.004) were significantly associated with presence of sinonasal symptoms after air travel. However, no significant relationships were observed between the presence of sinonasal symptoms and age, gender, allergy, smoking, medical conditions, or previous accidents involving the head, face, or nose (p>0.05, Table 3).
- Univariate analysis of the factors influencing the presence of sinonasal symptoms (N=184).
Significant results from the univariate analyses were used to carry out a multivariate regression analysis to identify independent predictors of sinonasal symptoms. The results revealed that aircrew members who experienced nasal, sinus, or ear problems during flight were at least 2.98 times more likely to report sinonasal symptoms than those without sinonasal problems (AOR=2.973; 95% CI: [1.323-6.679]; p=0.008). Similarly, aircrew members whose symptoms impacted their job performance were 4.3 times more likely to experience sinonasal symptoms compared to those whose performance was unaffected (AOR=4.285; 95% CI: [1.586-11.578]; p=0.004). Additionally, a history of sinus, nasal, or ear surgery was predicted to have a 3.8 times increased risk of developing sinonasal symptoms (AOR=3.777; 95% CI: [1.126-12.674]; p=0.031). After adjustments to a regression model, no significant effects were observed between sinonasal symptoms and job categories, the need to cancel or change trips due to recurring symptoms, duration of air travel, or taking medication (p>0.05, Table 4).
- The multivariate regression analysis identifying significant independent predictors of sinonasal symptoms (N=184).
Discussion
This study examined the effects of extended flight exposure on the sinonasal health of aircrew members in Saudi-based airlines. According to the SNOT-22 criteria, 68.5% of aircrew members reported sinonasal symptoms ranging from mild to severe. These findings align with the study carried out by Alzahrani et al,10 who reported that sinonasal symptoms among aircrews were mild among 18.6% and severe among 24.4% (overall prevalence: 68.6%). Similarly, among 1789 Finnish aircrew members, 61% reported experiencing sinus barotraumas during flights.13 However, in China, the prevalence of self-reported allergic rhinitis among aircrew members was 23.4%, lower than our report.26 These variations in incidence may reflect differences in the sample size, cabin type, and the methodology applied in the study. Other factors, including the diversity of the study population and regional settings, may have contributed to a similar extent. There is clear evidence that sinonasal symptoms are prevalent among aircrews. Incidentally, not all cases of airline travel are associated with sinonasal symptoms; other symptoms could also contribute, such as fatigue, sleep deprivation, and headache.27-29 It may also elevate the risk of depression, anxiety, alcohol abuse, peripheral artery disease, and various adverse outcomes.30 Hence, airlines and other authorities can devise measures to mitigate the effect of long airline travel, including improved scheduling, regular health screening, training programs, and mental health support.
Data from this study suggest that longer durations of air travel were associated with the development of sinonasal symptoms; however, this did not remain significant after multivariate regression analysis, indicating the need for further investigation. Similarly, Shargorodsky et al11 found that trips lasting 9-10 hours were linked to a -0.02 reduction in the quality of life-respiratory questionnaire survey score, whereas trips exceeding 11 hours were associated with a more significant decline of -1.6 in the score.11 Following these reports, Bai et al26 documented that 10.3% of the aircrew experienced symptoms associated with flight duration, while a few (4.4%) experienced symptoms related to flight altitude. These accounts prove the association between flight duration and the sinonasal condition of airline staff; however, individual health status and environmental factors may have a significant influence on the development of sinonasal symptoms among airline travelers.
Furthermore, the findings of this study suggest that flight attendants who experienced nasal, sinus, or ear problems during or after flights, whose symptoms affected their job performance, who had to cancel or change trips due to recurring symptoms, who had a history of sinus, nasal, or ear surgery and who were on medication were linked to a higher likelihood of sinonasal symptoms. However, in the multivariate regression model, only the experience of sinonasal or ear problems, symptoms affecting job performance, and history of sinonasal or ear surgery remained significant as independent predictors of sinonasal symptoms. This contrasts with the findings of Lindfors et al,13 which suggested that female gender and a higher number of upper respiratory symptoms were associated with sinus barotrauma. These results warrant further investigation to determine the predisposing factors for sinonasal symptoms among aircrew members.
Recognizing specific sinonasal symptoms can help to identify and distinguish between various conditions affecting the nose and sinuses. This study identified the 5 most critical sinonasal symptoms experienced by air travelers, including nasal blockage, reduced productivity, ear fullness, ear pain, and a need to blow the nose. This is almost in agreement with the study of Alzahrani et al,10 where nasal discharge was the primary sinonasal symptom, followed by ear fullness and nasal blockage. Corroborating these observations, Shargorodsky et al11 identified the need to blow the nose, sneezing, and thick nasal discharge as the most prominent sinonasal symptoms linked to airline flight time. Effective management of this disease is necessary. Analgesics, decongestants (topical and oral), topical sprays, and a tapering course of oral steroids are some of the most recognized medications for aerosinusitis, while antibiotics are commonly prescribed in patients with bacterial sinusitis.20 If symptoms persist, consulting a doctor is crucial to improving health conditions.
Study limitations
First, the sample size (N=184) was inadequate, limiting the generalizability of the findings. Additionally, most participants were male, making it difficult to draw conclusive comparisons between genders regarding sinonasal symptoms. Second, the data collection relied on history-based reporting from aircrew members, which could lead to data entry errors, low response rates, and challenges in follow-up. Third, this study employed a convenience sampling method to collect data from aircrews, which could have resulted in sampling bias and lack of generalizability. Finally, the cross-sectional survey design is inherently prone to bias and does not measure cause and effect.
In conclusion, sinonasal symptoms are common among aircrew members. Flight attendants with longer durations of air travel were associated with the development of sinonasal symptoms after flights. Significant independent risk factors for the presence of sinonasal symptoms include experiencing nasal, sinus, or ear problems during or after a flight, symptoms affecting job performance, and a history of sinus, nasal, or ear surgery. Overall, extended flight exposure poses unique challenges to the sinonasal health of aircrew members. Increasing awareness and implementing preventive strategies can help mitigate these effects and improve the well-being of those frequently exposed to the demanding environment of the skies.
Acknowledgment
The author gratefully acknowledges Rommel R. Acunin for the statistical analysis and its interpretation. The author also would like to thank Editage (www.editage.com) for the English language editing.
Footnotes
Disclosure. Author has no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 1, 2024.
- Accepted April 14, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.