


Abstract
Objectives: To improve our local data and demographics of thyroid neoplasm in Makkah region, Kingdom of Saudi Arabia and provide some basic statistics for future studies in our local community.
Methods: A record based retrospective epidemiological study was conducted and included 314 thyroid disease patients who were presented to our centers at Makkah region, Kingdom of Saudi Arabia between December 2009 and December 2019.
Results: A descriptive statistical analysis was carried out. The average age was 42.77 years, with a female-to-male ratio of 3:1, and most of the patients were Saudi (77%). Fifty-seven percent of cases were benign, while in malignant cases, 33.4% were papillary thyroid carcinoma. The mean follow-up time was 15.44 months, with excellent compliance in 39.4% of the patients.
Conclusion: Thyroid tumors have a leading incidence in head and neck tumors in Makkah, Kingdom of Saudi Arabia, mandating further studies to determine the causes and distribution in other regions of the country.
Thyroid diseases are common disorders. Goitrous thyroid lesions are precursor lesions to thyroid carcinoma (TC). Because endemic goiter is a significant concern in many parts of the world, thyroid diseases are common disorders.1 It is known that the occurrence of thyroid lesions increases with iodine deficiency.2 In most countries, occurrence have been appreciably rising over the last few decades.3 This increase could be due to awareness and improved diagnostic methods; in particular, the widespread use of neck ultrasonography (US) and an increased ability to detect and diagnose small indolent tumors.4,5 If these recent trends are maintained, thyroid cancer may become the fourth most common cancer by 2030 in the United States.6
In the Kingdom of Saudi Arabia (KSA), TC is the second most common malignancy in women after breast cancer, and that thyroid is the ninth most common site of all cancers in women in the world.7 Thyroid carcinoma was ranked second in Saudi females and ninth in Saudi males.8
The objective of the study is to improve our local data and demographics of thyroid neoplasm in Makkah region, KSA and provide some basic statistics for future studies in our local community.
Methods
A record based retrospective review of a prospectively maintained demographic and clinical database of 314 thyroid disease-related patients including all the patients with thyroid nodule who were presented to our centers in Makkah region, KSA, from December 2009 to December 2019 and treated surgically. Exclusion criteria included patients less than 14 years old and patients with thyroid nodules who were treated medically. The study was approved by the Institutional Review Board of King Abdullah Medical City (KAMC), Makkah, KSA, and the National Biomedical Ethics Committee, King Abdulaziz City for Science and Technology (Protocol number 14-07-1433, registration number H-02-K-001). Preoperative data such as patient symptoms, type of surgery before referral, family history, drug history, vocal cord assessment, thyroid function test, the main radiological study in the patient, and pathological results of biopsy or reviewed pathology were recorded. Operative data related to the types of thyroid and neck surgeries, the result of the pathology type, and the TNM cancer stage were also obtained. Post-operative data included a clinical examination of the vocal cord and radiology, followed by neck US and computerized tomography (CT), if the patient received radioactive iodine (RAI). The dose for well-differentiated thyroid cancer cases, thyroglobulin level post-RAI ablation, post-operative hypocalcemia, recurrent laryngeal nerve (RLN) paralysis, and records of any revision surgery and outcome were incorporated into the database.
Statistical analysis
The Statistical Package for Social Sciences version 22 (IBM Corp., Armonk, NY, USA) package was used to analyze the data. The participants variables were estimated using descriptive statistics, including frequency counts and percentages for categorical variables.
Results
A total of 314 cases in our study with 179 benign cases and 135 malignant cases. The median age was 42.77 years, with a female-to-male ratio of 3:1. Most patients were Saudi (77%), half were from the Western KSA (157 Jeddah, Makkah, Taif), and 3% of cases had a history of family cancer. Concerning preoperative examination of the vocal cord, we found 17 cases with one immobile vocal cord, and 43 of the total cases underwent surgery at a different institution and were sent to us for completion of thyroidectomy. The mean duration of illness was 27.7 months. For all cases, we requested preoperative images, thyroid function tests, and thyroid fine needle aspiration (FNA), which were either carried out at our institute or reviewed on slides from cytopathology surgery at a different institution (Table 1).
Preoperative data of 314 thyroid patients.
Postoperative data
The waiting time from the first visit to the date of surgery was 11 weeks. Approximately 73.6% of the total cases underwent total or complete thyroidectomy with a mean length of surgery of 169 min, 5.7% underwent unilateral neck dissection and 4.8% underwent bilateral neck dissection. With respect to complications, we had 4 cases (1.3%) with unilateral vocal cord paralysis and 30 cases (13%) with hypocalcemia 6 months after surgery. A total of 179 cases were benign and the remaining 135 cases were malignant: 127 cases were follicular cell-derived thyroid cancer, the most common being papillary thyroid cancer (PTC), 71.4% were classic types; followed by follicular thyroid cancer (FTC). Papillary thyroid cancer was more common in women (73 cases). Most cases of differentiated thyroid cancer (DTC, 94/127) were treated with RAI ablation, and 68.08% of them received only one dose (30 mci), the majority of which were performed in KAMC at 63%. The mean waiting time from the date of operation to the start of RAI dose was 11.69 weeks. Thyroglobulin (TG) was the tumor marker used to evaluate and monitor thyroid cancer management. In 41% of the participants, TG level was <1 ng/ml (Table 2).
Preoperative data of 314 thyroid patients.
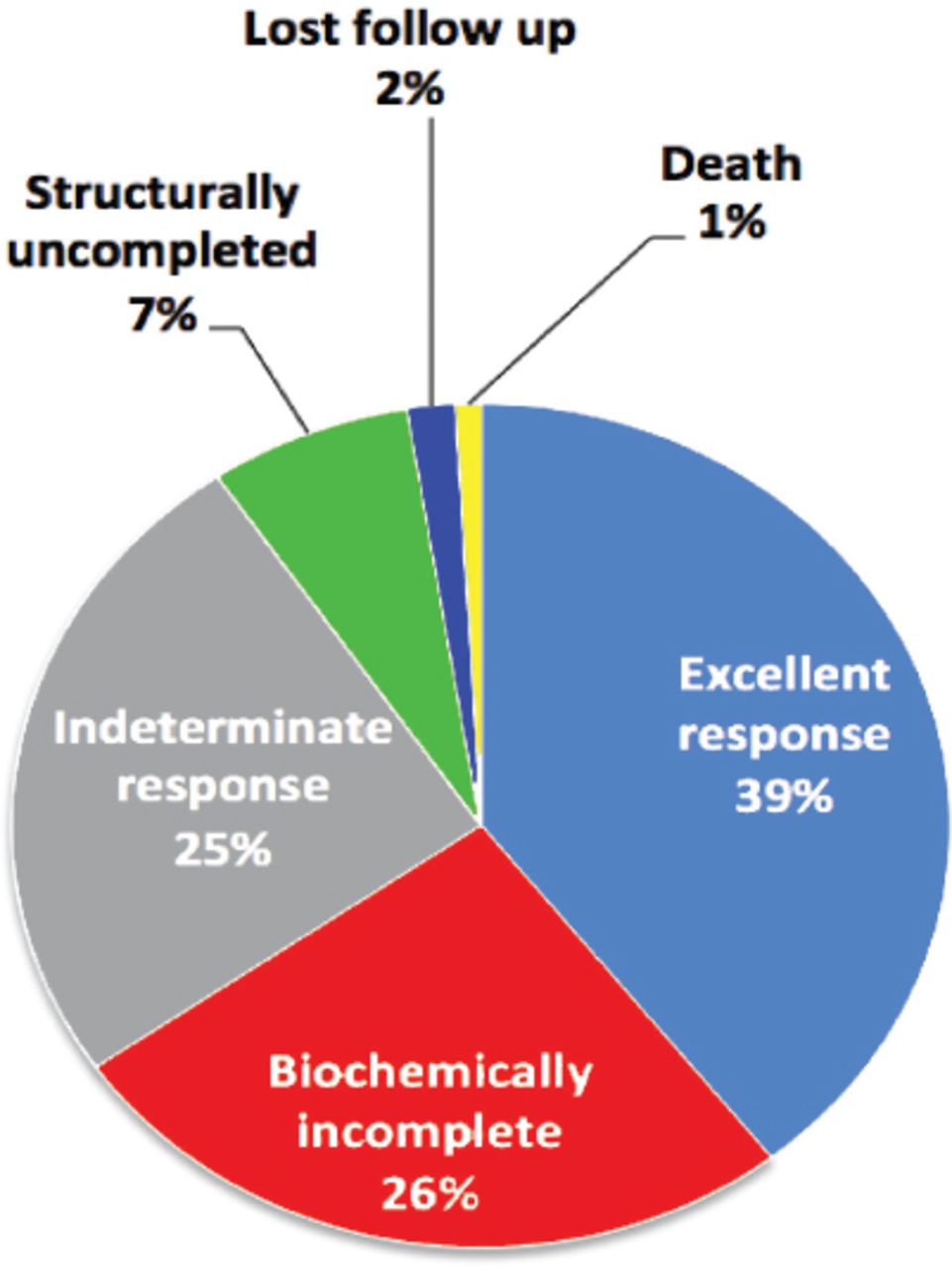
From the last follow-up visit of cancer cases after thyroid surgery and RAI ablation, and according to the the American Thyroid Associations (ATA) of differentiated thyroid carcinoma (DTC), 39.4% of the participants had an excellent response status, and mean follow-up was 15.4 months (Figure 1). The outcome of the 7 cases of non-DTC as follows: one case anaplastic thyroid cancer died from the disease within 5 months of the diagnosis, and the remaining 6 medullary thyroid cancer cases; had excellent response without any evidence of recurrence.
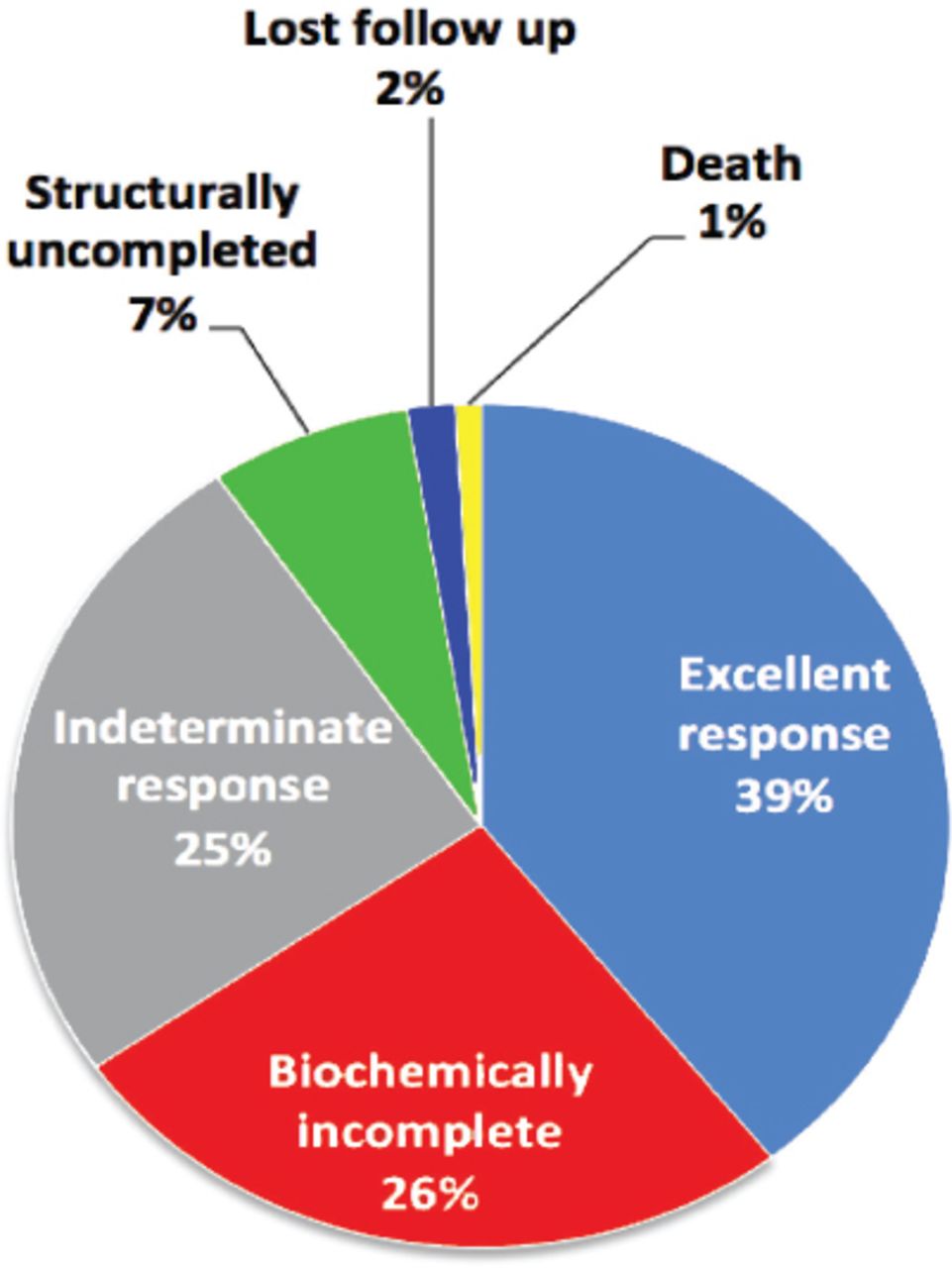
Outcome of differentiated thyroid carcinoma.
Discussion
Thyroid cancer is the second most common cancer of the head and neck region after nasopharyngeal cancer.1-4 Saeed et al,1 found that the highest occurrence of thyroid swelling in the Western region of KSA was noted in the fourth decade of life, followed by another peak observed in the third decade. Another study supports that the highest occurrence of neoplastic disease is seen in the third decade, which is in agreement with our present study.9 Moreover, out of the 314 cases in our current study, there was a female preponderance with an overall male-to-female ratio of 1:3, which is in agreement with the fact that thyroid diseases are more common in women.1,2,7,10,11
In KSA, a significant increase in thyroid cancer occurrence over the last few years due to several risk factors.3,4,12 Our study included patients from different regions as KAMC is a tertiary referral center in the western part, so the majority of our samples were from the western region (157 patients).
Preoperative patient evaluation and preparation, including laryngeal assessment with fiber-optic laryngoscopy, detected unilateral VC paralysis in 5.4 % of the patients, and most of the patients had a history of previous thyroidectomy on the same side of vocal cord paralysis.
In our institute, we followed the ATA guidelines. Preoperative diagnostic thyroid/neck US should be performed in all patients with a suspected thyroid nodule. Some patients having a bulky thyroid with retrosternal extension or clinical palpable neck lymph nodes require a combination of US and CT scans for better evaluation of the central and lateral compartments.8 A CT scan was requested in combination with the US in 23.6% of cases.
Moreover, the diagnostic accuracy of CT in thyroid swelling detection was 92.6% in a previous CT study using surgical findings as the reference standard.10 In 58 cases, we requested only CT scan because those cases were referred from good centers with good quality neck US and fine needle aspiration cytology (FNAC) pathology report.
Fine needle aspiration cytology is considered a first-line invasive investigation in the evaluation of thyroid lesions; with high sensitivity and specificity.13 Mundasad et al,14 performed a comparison study between FNAC and histopathology and found that the FNAC sensitivity was 52.6% and specificity was 86.6%. Handa et al,15 performed a similar study, in which FNAC revealed a sensitivity of 97% and specificity of 100%.16,17
As a referral center, our sample included approximately 43/314 patients who had already undergone primary surgery for benign or malignant disease, carried out in another center. All 43 patients required re-operative completion procedures, with additional challenges to the operative surgeon, especially in cases with preoperative vocal cord paralysis.
Therapeutic lymph neck dissection (ND) was performed only on patients with confirmed lateral lymph node metastases, either primary or revision cases, undergo cervical ND; as per ATA guidelines.8
In our study, most of the cases were benign nodules and PTC was the most common variant in TC cases. This is consistent with the literature, which showed that PTC is the most frequently differentiated TC, followed by follicular carcinoma.12,18,19 Hussain et al,19 reviewed the demographic aspects of TC patients for 10 years at the King Faisal Specialist Hospital and Research Center in Riyadh, KSA, and showed that the majority of cases had PTC and its classical subtype (72%). This is very close to our findings (70%).19
As most of our cases were diagnosed as DTC and underwent RAI ablation to eliminate the residual healthy thyroid tissue after total thyroidectomy (TT), a recent study conducted in Europe in 2018 showed that a low dose of RAI is as effective as a high dose for the ablation of thyroid remnants in low- and intermediate-risk patients.20,21 Additionally, the low dose RAI has clinical advantages such as the reduction of side effects and risk of a second primary cancer.21 Indeed, 74% of our DTC cases received RAI ablation, and around 68% of these patients needed only one dose of RAI.
Thyroidectomy is considered to be a safe surgery with a low occurrence of complications. It has been demonstrated that when performed by high volume surgeons, the procedure is associated with favorable outcomes and fewer complications.21
Hypocalcemia is the most common post thyroidectomy complication and is related to an injured parathyroid gland vascularity causing permanent or transient ischemia post-operatively. Global hypocalcemia occurrence ranges from 1.2-40%. This wide range of occurrence is affected by various factors such as the definition of hypocalcemia, the size and type of thyroid disease, and the surgical technique used for thyroidectomy.22,23 In the current study, patients were followed for 6 months to monitor any biochemical changes including hypocalcemia. Our cut-off range for hypocalcemia was 8 mg/dL, and the result showed that 12.5% had persistent hypocalcemia, which requires long-life calcium and vitamin-D supplementation.
The occurrence of permanent RLN palsy following thyroidectomy varies considerably in the literature, ranging between 1-5%, which was similar to our occurrence (1.3%). Although an increase in this occurrence is influenced by many factors like the surgeon’s experience, extent of thyroid cancer resection, and revision cases, the occurrence reaches 5.5% in some studies.4,5,7,10
In our study, all patients with recurrence were initially classified as high-risk patients, as assessed by the ATA classification.8 Mazzaferri et al,24 demonstrated that the recurrence rate, residual tissue, and cancer-specific mortality rate are significantly higher in patients who underwent subtotal thyroidectomy than in those who underwent total thyroidectomy.
Patient follow-up has an important role in detection of the outcome. Alzahrani et al,18 classified the results of patients who were diagnosed with DTC and receiving RAI treatment postoperatively by following the ATA classification protocol and showed that 44.8% of patients had a complete response and 26.5% had a structural response. However, our cases’ outcome in DTC show almost the same ranges with complete response but with a much lower percentage structurally in total, 7%. Moreover, the result of the non-DTC shows 6 cases of medullary thyroid cancer with an excellent response without any evidence of recurrence.
The mortality rate in our study was 0.9% (3 patients). Two cases had a prolonged significant comorbid disease; and one patient was diagnosed with anaplastic thyroid carcinoma (ATC). The average survival time of ATC is only 6-8 months, and the 5-year survival rate of ATC is only 0-10%.21,25 However, TC mortality remains flat, implying that these small cancers are unlikely to have progressed to being life threatening.21,25,26
Study limitations
The current study has several strengths and limitations, which include a large sample from the main tertiary care center in KSA, where most of the cases undergo standardized practice and management. On the other hand, the retrospective nature of the study with an extended period adds the limitations.
In conclusion, thyroid tumors have a leading occurrence in head and neck tumors in Makkah, KSA. The continuous building of surgical experience and data collection are very important in achieving research and clinical excellency. Furthermore, conducting more studies to determine their causes and distribution in other regions of the country is needed.
Acknowledgment
The authors gratefully acknowledge Editage for English language.
Footnotes
Disclosure. This study was funded by the Institute of Consulting Research & Studies, Umm Al-Qura University, Makkah, Kingdom of Saudi Arabia.
- Received July 30, 2020.
- Accepted November 17, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}