


Abstract
The incidence of communicable diseases has witnessed a reduction in Saudi Arabia during the last 4 decades. Nonetheless, the Jazan region has been indicated as one of the main regions affected by various communicable conditions. The geographical, socioeconomic, and climate characteristics of Jazan have made it vulnerable to communicable and vector-borne diseases. This review aims to provide a comprehensive overview of the epidemiology of communicable diseases in Jazan, Saudi Arabia. This review also gives a historical description of infectious diseases in the region and the relevant prevention and control measures. Prevention and control efforts in the Jazan region successfully eliminated Rift Valley fever and reduced the number of locally acquired malaria and chickenpox cases. Hepatitis B, dengue fever, and pulmonary tuberculosis have exhibited an increased incidence in recent years, suggesting a need for further epidemiological investigations and the application of relevant prevention and control measures.
The risk of ailment varies between individuals according to their internal characteristics (such as genetic risk) and environmental factors (such as the risk of exposure to vector-borne diseases). The concept of risk variation also applies at the population level, where populations may exhibit variation in the incidence of particular health conditions due to variations in exposure to genetic, cultural, behavioral, socioeconomic, geographical, political, and environmental risk factors. Holistic assessment of the health status of a community is rather important to diagnose a community, identify causes and risk factors, and apply the subsequent interventional methods at the community level.
Saudi Arabia (SA) is one of the countries that have been successful in the application of public health practices to ensure health promotion in its communities and the prevention of communicable and non-communicable diseases. Examples of the applied public health practices in SA include the establishment of communicable disease notification systems and public health surveillance systems, assessment of the health status and risk levels of communities, and the application of public health interventions such as the expanded program of immunization, immunization against emerging diseases such as coronavirus disease-19 (COVID-19), screening programs such as the healthy marriage program, and disease-specific control programs such as the national malaria control program and the national tuberculosis (TB) program.
The incidence of communicable diseases has witnessed a remarkable reduction in SA during the last 4 decades, including the successful elimination of some communicable diseases, such as the elimination of Rift Valley fever in the 2000s. Nonetheless, SA can be considered a geographically large country, as it represents the majority of the Arabian Peninsula, with a land area of more than 2 million km2.1 The large geography of the country is associated with variations in the climate of the 13 regions of the country. Additionally, SA is bordered by 7 countries, and health risk factors in those countries can influence the health status of communities in SA. Finally, the cultural value of SA and its economic growth have made it an area of economic and cultural interest; millions of expatriates live in the country, and millions more visit the country every year, including for religious purposes such as Hajj and Ummrah.
The Saudi Ministry of Health (MoH) and other health establishments (such as the Saudi Health Council), academic institutions, the General Authority of Statistics in SA, and international health organizations (such as the World Health Organization [WHO]) publish annual and periodic reports that illustrate several public health aspects of the country. The provision of historical data regarding public health in SA enables assessment of the effectiveness of various public health programs throughout the recent decades. Furthermore, these nationwide reports compare the incidence of particular health conditions in regions of the country and identify challenges and areas for further investigations and improvement in specific regions of the country.
Aims and methodology
This review aims to provide a comprehensive overview of the epidemiology of communicable diseases in Jazan region. This review also gives a historical description of infectious diseases in the region and the efforts of the Saudi MoH in the successful prevention and control of these illnesses. Furthermore, the review presents a description of the current status of infectious diseases in the region, including frequencies, patterns, and determinants. Challenges pertaining to the application of public health interventions and areas of further research are indicated. Finally, the epidemiology of major infectious diseases identified in Jazan region was compared to similar international settings with similar prevalent diseases.
The contents of this review were generated after consulting the statistical yearbooks of the Saudi MoH and the relevant health literature investigating health conditions in Jazan region. Data regarding the incidence of communicable diseases were retrieved from the notifiable diseases section of the published statistical yearbooks, which are currently limited to the years 2006-2021.2 Statistical data regarding communicable diseases in the region were retrieved to calculate the annual frequency of infectious diseases, cumulative frequency through the years 2006-2021, and the proportion of the number of these communicable diseases in comparison with the overall number of communicable diseases in SA. Any notifiable disease with an incidence of one case or more during the studied years in Jazan region was included in the analysis. Notifiable diseases with an incidence of zero in Jazan region throughout the studied period were not involved in the analysis except for Rift Valley fever.
Determinants of infectious diseases in the region were extrapolated either from the statistical yearbooks of the Saudi MoH, such as information regarding gender, age, and incidence according to the month, or studies that assessed the epidemiology of communicable diseases in Jazan region. To ensure the detection of all studies that investigated health conditions in Jazan regardless of the nature of the disease, broad search keywords were used in the relevant scientific search engines, such as using Jazan and Gizan as keywords in PubMed and Google Scholar and screening all the results in addition to searching reference lists of articles of interest. More than 400 titles were detected concerning investigations that were either carried out in Jazan or carried out on a national level and included a sample from Jazan. Among the identified titles, the abstracts were further screened to identify investigations regarding various communicable diseases in Jazan.
Characteristics of the region of Jazan and its implication on public health
Jazan region has been indicated as one of the main regions in SA that have been affected by various communicable diseases during the last 5 decades. Jazan is one of the 13 administrative regions of SA and represents the second-smallest region of SA, with a total size of 13.457 km2 and a total population of 1,365,110. The region is located in the southwestern part of SA and the northern part of Yemen.3
Jazan region has unique geographic characteristics that distinguish it from the rest of SA. It has a coastline of 330 km of the Red Sea on the west and has more than 80 islands, including the famous Farasan islands.4 In the southern parts of the Jazan region are the Sarawat mountains, a chain of mountains starting from Makkah region in the north and ending in Yemen, where the highest peaks can reach 9,000 feet in some parts of Asir and Jazan Province. From the Sarawat mountains, several large valleys slope toward the coastal line of Jazan region.1
Jazan has subtropical weather and seasonal rainfall. The weather conditions and geographical nature of the region have made it one of the main agricultural locations of SA. Furthermore, in addition to the region’s contribution to the production of fish, livestock, and several agricultural products, in recent years, the Saudi Arabian government has invested in the development of the biochemical and petroleum industries in the region to target the neighboring East African markets.5
The geographical, socioeconomic, and climate characteristics of Jazan have made it vulnerable to several communicable and vector-borne diseases. These illnesses include Rift Valley fever, malaria, dengue fever, leishmaniasis, and bilharziasis. The incidence of these conditions in the region is also affected by the geopolitical situation in the neighboring country of Yemen; wars can have an impact on communicable disease control in that country and lead to a higher probability of movement of infected migrants to Jazan. Furthermore, the dependence of farmers in the remote mountains of Jazan on livestock and agricultural activities and the socioeconomic status of its residents have been indicated as factors contributing to the incidence of communicable diseases in the region throughout the last few decades.6
Epidemiology of commonly reported communicable diseases
Assessment of the incidence of nationally notifiable diseases in Jazan region between 2006 and 2021 indicates the presence of several communicable conditions that can be described as endemic in the region. Figure 1 displays the proportions of cumulative frequencies of notifiable diseases in Jazan between 2006 and 2021. Additionally, Table 1 displays data concerning the frequencies of malaria, hepatitis B, dengue fever, chickenpox, and pulmonary TB in the region. It can be noted that malaria, hepatitis B, dengue fever, chickenpox, and pulmonary TB represent 84% of all notifiable communicable diseases in the region between 2006 and 2021, with variability in the incidence according to the years. Nonetheless, it can be noted from Table 1 and Figure 2 that among the most frequently reported conditions throughout the studied period, only the incidence of chickenpox during the last 5 years has witnessed a reduction in comparison with earlier incidence levels.

- The proportions of cumulative frequencies of notifiable diseases in Jazan region between 2006-2021. TB: tuberculosis
- Most frequently reported communicable disease in the Jazan region, Saudi Arabia, between 2006-2021.
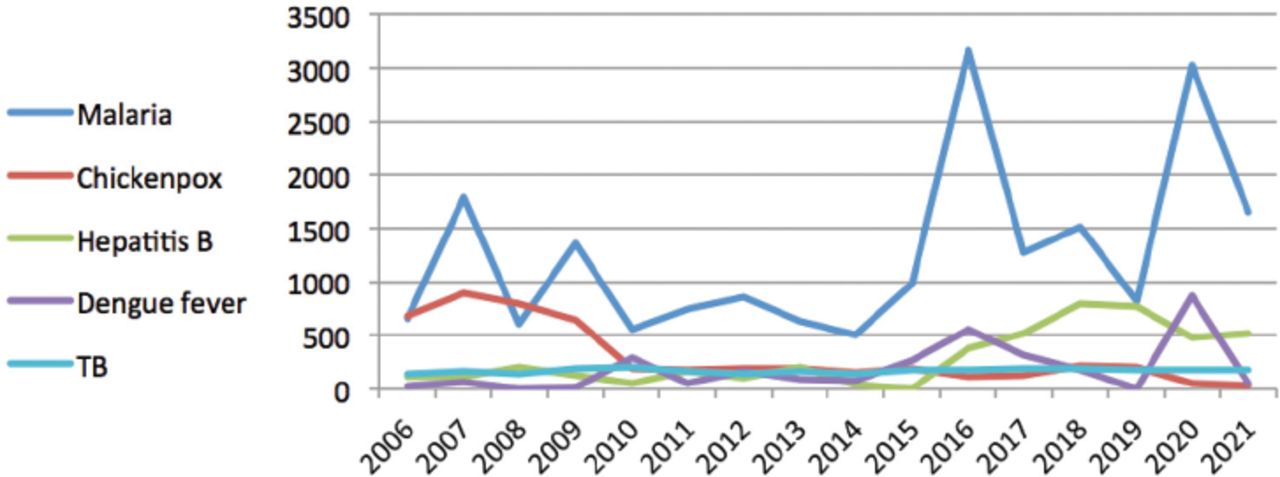
- Yearly number of cases of most frequently reported infectious diseases in Jazan, Saudi Arabia between 2006 and 2021. TB: tuberculosis
Malaria
Assessment of the causative organism of malaria in Jazan region indicates that the majority of malaria cases were caused by Plasmodium falciparum (>80%). Additionally, only 321 cases of malaria were indicated as locally acquired conditions between 2006 and 2011, and the majority of cases of malaria notified in Jazan were imported. In the year 2021, among the reported 1,657 cases of malaria, none of the cases was acquired locally, 112 were indicated as introduced cases, and 1,545 were indicated as imported cases.
Assessment of the incidence of malaria in Jazan between 2006 and 2021 according to age groups indicates that the majority of cases were diagnosed among subjects older than 10 years (92%). Assessment of reported cases of malaria in Jazan according to the month between the years 2009 and 2021 indicates the presence of seasonal variation of incidence of malaria cases in the region (except for the years 2012 and 2013, which were not reported in the statistical yearbooks of the Saudi MoH). The highest cumulative frequency of malaria cases according to the month was indicated in February, followed by January, March, and December, with very low numbers of reported malaria cases in the summer seasons.
Studies that assessed factors associated with the incidence of malaria in Jazan indicated the presence of associated demographic and environmental factors and measured the effect of interventions applied for malaria control in the region. In a cross-sectional study by Al-Mekhlafi et al,7 which recruited 1,124 positive cases of malaria detected between 2010 and 2017, it was concluded that higher proportions of malaria patients were detected among males, patients who belong to the 18-30 age group, non-Saudis, and residents of rural areas. Furthermore, seasonal variation in the incidence of malaria cases indicated the effect of temperature and humidity, where an increased incidence of malaria was recorded after rainfall seasons.
A comprehensive review was carried out by El Hassan et al8 to investigate malaria elimination efforts in Jazan between 2000 and 2014 and summarized major preventive and curative efforts provided by the Saudi MoH. El Hassan et al8 indicated that a total of 5,522 locally acquired cases of malaria were detected between 2000 and 2014 in Jazan, indicating a variation in the incidence of malaria between Jazan region governorates, where governorates on the border with Yemen witnessed higher incidence in comparison with northern governorates.
The large reduction in the incidence of locally acquired malaria cases in Jazan region documents the success of the malaria control program applied in the region. Malaria control efforts in the region were dependent on early detection of cases, continuous assessment and update of malaria treatment practices, and vector control. According to El Hassan et al,8 chloroquine was an effective treatment for malaria cases in the region. However, the occurrence of falciparum infection resistance led to the introduction of artesunate as a first-line treatment in 2007, in addition to other medication options. Additionally, several vector control measures were applied, including indoor residual spraying of more than 51,000 households between 2004 and 2014, larviciding via biological and chemical control applied in more than 100 valleys with more than 500 tributaries and 13,800 breeding sites in villages, and distributing around 500,000 insecticide-treated bed nets in communities with active foci of transmission along the border with Yemen.8
In summary, the majority of the malaria cases identified in Jazan were caused by Plasmodium falciparum. Determinants associated with the incidence of malaria in the region were mainly related to environmental determinants, including the higher incidence in the winter season and after the rainfall. Furthermore, other demographic determinants were identified to be associated with malaria incidence in Jazan region, such as the higher risk among males, non-Saudis, residents of rural areas, and those aged between 18-30. By 2021, none of the malaria cases were acquired locally, and the majority were imported cases, indicating the success of the applied malaria prevention and control programs in the region.
According to the global malaria program of the WHO, SA is not among the certified malaria-free countries.9 However, the incidence of malaria in SA is relatively lower in comparison to other international settings. According to the WHO, African countries were indicated as one of the main regions affected by malaria, where they are home to 95% of malaria cases in the globe.10 According to the World malaria report, the number of malaria cases increased from 245 million cases in 2020 to 247 million cases in 2021, indicating the presence of malaria prevention and control challenges on a global level where significant challenges were pertaining to diagnoses of malaria cases by rapid diagnostic tools, parasite resistance to antimalarial drugs, and limited effectiveness of insecticide-treated nets.11
Hepatitis B
Literature that investigated factors associated with hepatitis B infections in the region of Jazan indicated a decline in cases during the last 4 decades. Earlier investigations carried out in Jazan reported a relatively higher prevalence of hepatitis B in comparison with recent reports. For example, in a study that assessed the prevalence of hepatitis B in 1985, the prevalence of subjects with evidence of existing or earlier hepatitis B infection was 46.5% in a sample of 724 subjects from Jazan (of whom 12.7% were hepatitis B surface antigen [HBsAg] carriers).12 A similar study, which assessed the prevalence of hepatitis B among children in 1986, revealed evidence of existing or earlier hepatitis B infection in 28% of 325 schoolchildren (of whom 11.1% were HBsAg carriers).13
Subsequent investigations carried out to assess the prevalence of hepatitis B in the region among larger samples indicated reductions in the prevalence of the disease. A study by Ayoola et al,14 which reviewed data from 14,882 voluntary blood donors in Jazan between 1995 and 1998, indicated that only 5.4% were carriers of HBsAg. Additionally, Ayoola et al14 recruited a sample of 229 children aged less than 10 years, where only 2 (0.9%) children were identified as carriers of HBsAg. A similar study assessed the presence of HBsAg among 29,949 blood units donated between 2004 and 2009 in the region of Jazan, indicating a reduction of the prevalence from 5.6% in 2004 to 2.3% in 2009.15
Despite the presence of several studies carried out to assess the prevalence of hepatitis B cases in Jazan, studies that assessed determinants of the disease and modes of transmission are limited. A study that analyzed demographic data of 1,888 subjects diagnosed with hepatitis B infection in Jazan between 2015 and 2018 indicated a higher prevalence of the disease among males, Saudis, and those who belong to older age groups (the mean age of the patients was 44.5 years).16 Furthermore, Al-Mazrou et al17 carried out a study in the early 2000s in which they recruited a sample of 2,664 pregnant women from 5 regions of SA, including Jazan. They detected 65 pregnant women with HBsAg, 23 of whom were from Jazan (35% of all positive cases). Upon investigating possible exposures increasing the risk of infection among the identified cases, no statistically significant associations were identified with the risk of infection according to the history of surgery, blood transfusion, or dental procedures.17
The decline in the incidence of hepatitis B indicated in Jazan region can be justified by the overall reduction of incidence in the country. In the late 1980s, the Saudi Arabian government introduced mass vaccination against hepatitis B, including among children in their first year of school, and introduced the hepatitis B vaccine in the expanded program of immunization; the introduction of the vaccine was indicated to be associated with the reduction of hepatitis B incidence, especially among children.18 Furthermore, the establishment of screening of blood donations and premarital screening in the country assisted in the identification of cases, enabling the application of subsequent preventive and curative measures.19 Nonetheless, despite the reduction of hepatitis B cases in the country, the presence of the disease among older individuals generates a risk of exposure in the community and may explain the persistence of infection with hepatitis B in the country and in Jazan region. This indicates the need for further investigations in the region to identify possible routes of transmission among high-risk individuals and in healthcare settings. Finally, reports on efforts carried out in the region for the prevention and control of hepatitis B are currently lacking.
In summary, although hepatitis B represents one of the most frequently diagnosed infectious diseases in Jazan region, the incidence of the disease has witnessed a reduction in the region. The reduction of the incidence of hepatitis B in the region is associated with the overall reduction of the cases in the country, suggesting the success of various programs dedicated to primary and secondary prevention of the infection, such as vaccination and screening programs. However, the persistence of the infection indicates the need for further investigations.
The prevalence of hepatitis B in SA was reported to be relatively lower than the global prevalence of the disease (3.2% versus 3.6%).20 In a systematic analysis carried out by the Global Burden of Disease 2019 Hepatitis B collaborators, it was revealed that although the prevalence of the disease has decreased since 1990, approximately 316 million individuals are affected with chronic hepatitis B.21 Nonetheless, variations in the incidence of hepatitis B between countries can be noted. For example, according to the Centers for Disease Control and Prevention, a total of 2.157 acute cases of hepatitis B and a total of 11.635 newly detected chronic cases of the disease were reported in 2020, indicating an increase of cases in comparison to the year 2019 where the main reason of increase of cases was partially explained by under-reporting associated with the COVID-19 pandemic.22 Furthermore, the burden of the disease has been reported to be higher in sub-Saharan Africa and East Asia, where major factors associated with the infection rates were underdiagnosis and the associated low treatment rates.23
Dengue fever
Studies that assessed the epidemiology of dengue fever in the region of Jazan are limited. A study by Alshabi et al,24 which reported the incidence of dengue fever in Jazan region between 2012 and 2020, indicated that the cumulative incidence of the disease in the study period was 3,757 cases, which is relatively higher than the reported cases of dengue fever in the corresponding Saudi MoH statistical yearbooks. The variation in recorded incidence can be partially explained by variation in the identification of cases and the reporting systems, as Alshabi et al24 recruited patients from non-governmental hospitals. According to Alshabi et al,24 a marked increase in the incidence of dengue fever in recent years has been detected. Furthermore, nearly half of the sample diagnosed with the disease were 30 years old or younger (9% under the age of 10), 61.8% of the patients were males, and the majority of the patients were either Saudis or Yemenis.24 Unlike malaria cases identified in the region in recent years, dengue fever incidence in Jazan suggests endemicity, with Saudis and those of younger ages at risk of developing the disease.
Earlier reports indicate that SA was a dengue-free country, and earlier cases of the disease were identified in the western regions of SA in the early 1990s.25 Subsequently, the disease spread to other regions of the country, including Jazan; the current evidence suggests that Jazan has a high incidence of dengue fever in comparison with other regions of the country. Al-Raddadi et al26 carried out a seroprevalence study of anti-dengue IgG antibodies in 4 regions in the west and south of SA, and the highest prevalence was detected in Jazan. Furthermore, Al-Raddadi et al26 concluded that rates of mosquito bites, the presence of mosquitoes in homes, and the presence of breeding sites were the highest in Jazan region in comparison with the other studied regions, which may partially explain the higher seroprevalence of dengue in the region. In a study that recruited 553 patients diagnosed with dengue fever in Jazan between 2010 and 2011, nearly one-third of the cases were reported in April in comparison with the number of cases recorded in August, indicating the presence of seasonal variation in the incidence of cases in Jazan.27 Finally, another smaller-scale study that assessed seroprevalence of dengue infection in the Baish and Al Darb governorates in Jazan in addition to samples from the Aseer region indicated that anti-dengue IgG was detected among 71 subjects of 268 screened participants in Jazan. Furthermore, it was concluded that living on farms and proximity to animal water basins was a major risk factor for dengue infection among their sample.28
The dengue surveillance program was established in SA in 1994.26 Later on, dengue fever was designated as an electronically notifiable condition in SA in 2008.29 The surveillance system is now operational under the umbrella of the Saudi Center for Disease Prevention and Control.30 A review of the literature suggests the presence of limited evidence regarding the prevalence of dengue fever and its demographic and environmental determinants in Jazan. Additionally, reports on the application of a vector control program targeting the dengue virus in the region are currently lacking. Nonetheless, a study published in 2016 indicated that adult Aedes aegypti mosquitoes (vectors of the dengue virus) are only susceptible to cyfluthrin and showed variable resistance to other insecticides, while the larvae were more susceptible to methoprene in comparison with other larvicides.31 Finally, the relevant literature suggests adequate knowledge on dengue fever among primary healthcare attendants but limited mosquito bite prevention practices.32
In summary, dengue fever witnessed the highest incidence in Jazan in 2020. However, a higher prevalence of the disease is expected due to underdiagnosis. Although SA was indicated as a dengue-free country before the 1990s, the current infection rates suggest endemicity in the region. Dengue fever infections in the region are mainly attributed to environmental determinants and possible resistance of the Aedes aegtpti to insecticides.
According to the WHO, nearly half of the globe’s population is at risk of dengue fever, where between 100-400 million infections occur on an annual basis. The prevalence is higher in tropical and sub-tropical regions and was indicated to be higher in urban areas.33 Variation of the incidence of dengue fever has been indicated due to variation in the climate and urbanization. Unlike malaria, which is predominantly prevalent in Africa, It has been reported that the majority of dengue fever cases occurred in Southeast Asia and South Asia.34
Pulmonary tuberculosis
According to the Saudi national tuberculosis program, the incidence of TB has been reducing over the past 5 decades in SA since the application of the program. Its main control interventions are related to surveillance, early detection of cases, and application of appropriate treatment regimens.35 Nonetheless, despite the relatively smaller population size of Jazan in comparison with other major regions in the Kingdom, Jazan represents one of the main regions affected by pulmonary TB. A study that assessed TB trends in SA between 1990 and 2010 concluded that Makkah and Jazan witnessed the highest incidence rates of TB in comparison with the other regions and indicated the presence of control challenges in some regions in the country.36 However, studies that assessed epidemiological factors contributing to the risk of acquiring TB infection in Jazan are limited to a single study, which assessed the risk of developing TB among 316 patients diagnosed with HIV and suggested the need to screen patients affected with HIV for TB and to integrate healthcare delivered for HIV and TB patients.37
In summary, Jazan represents one of the main regions affected by pulmonary TB in SA. The current evidence suggests that the development of TB among cases in Jazan is associated with HIV diagnosis. However, evidence concerning other risk factors associated with TB in the region is limited.
According to the WHO, approximately 10.6 million people were affected by TB in 2021. Nearly 7% of these cases were among people diagnosed with HIV, and the majority of the cases were from Southeast Asian countries, followed by African countries.38 It has been reported that the COVID-19 pandemic posed a challenge to TB control programs in recent years, where sub-optimal treatment and limited preventive services were the main factors associated with the increased burden of the disease. Undernutrition, poverty, diabetes, tobacco smoking, and household air pollution were indicated as determinants associated with the global burden of the disease.39
Chickenpox
Searching the relevant literature indicated a lack of studies that investigated the epidemiology, prevention, and control of chickenpox in Jazan. Nonetheless, a significant reduction of reported cases of chickenpox in Jazan since 2009 is noted (95% reduction). Investigations carried out to assess the epidemiology of chickenpox vaccination in SA indicated that the chickenpox vaccine was introduced in SA in 1998 and was mandatory in the expanded program of immunization in 2008. The introduction of the vaccination against chickenpox was associated with reduced incidence of the disease all over the country.40 Although the success in the prevention and control of the disease is evident, chickenpox outbreaks in SA have been reported in healthcare settings, suggesting a need for assessment of the susceptibility of chickenpox outbreaks among vulnerable populations.41
Although chickenpox is a vaccine-preventable condition, recent reports indicate that the incidence of the condition is still continuing to increase. For example, chickenpox has been indicated as the third most frequently reported vaccine-preventable disease in China after TB and influenza, where factors associated with the vaccination and under-reporting of cases have been indicated as the main challenges of the chickenpox prevention and control efforts.42 In 2019, nearly 84 million people were diagnosed with chickenpox globally, where the highest incidence was indicated to occur in Asia Pacific countries.43 In a review that assessed factors associated with the incidence of the disease in Sri Lanka, the lower temperature climate, exposure to the disease in household, school, or work settings, and high population density have been indicated as the main driving factors for the incidence of chickenpox in Sri Lanka.44
Epidemiology of other communicable diseases with higher incidences in comparison with other regions in SA
This section reviews infectious diseases with low frequencies in Jazan but higher incidence levels in comparison with other regions in SA. According to the statistical yearbooks of the Saudi MoH, a total of 158 cases of visceral leishmaniasis were reported in Jazan between 2006 and 2021, representing 73% of all reported cases of visceral leishmaniasis in the country during that period. Despite the application of the national leishmaniasis control program in SA during the 1980s and the success in reducing the incidence, visceral leishmaniasis can be described as endemic in the southwest of SA, namely, Jazan and Aseer regions.45
The 2021 statistical yearbook of the Saudi MoH indicates that 8 cases of visceral leishmaniasis were reported in Jazan, representing all the cases of the disease reported in SA. Studies that assessed the epidemiology of visceral leishmaniasis in the region indicated that Leishmania donovani and Leishmania infantum have been identified as causative organisms of the disease in the region.46 Historical studies published in 1992 and 1994 on the epidemiology of visceral leishmaniasis in the region indicated that the black rat (Rattus rattus) was reported as a probable reservoir for visceral leishmaniasis in Jazan and indicated that the incidence of the disease, which is transmitted by sand fly bites, was variable according to the seasons, with more cases reported during the summer than the winter.47,48 Nonetheless, more recent epidemiological investigations assessing the endemicity of the disease in the region are currently lacking.
According to the WHO, nearly between 700000 and 1 million cases of leishmaniases, including visceral leishmaniasis, occur in the world on an annual basis.49 The majority of visceral leishmaniasis has been reported to be detected in Eastern African and Southeast Asian countries. Visceral leishmaniasis prevention and control measures have been successful in some countries leading to the elimination of the disease, such as in China. However, some countries faced challenges pertaining to the control of the disease due to factors related to limited surveillance, limited cases detection and management, and limited vector control activities.50
According to the statistical yearbooks of the Saudi MoH, a total of 1,227 cases of measles were reported in Jazan between 2006 and 2021, representing 11.8% of all reported cases of the disease in the country during that period. The number of reported cases of measles in Jazan between 2006 and 2021 is fluctuant. For example, in the past 5 years, the highest number of measles cases in the region was reported in 2019, with a total of 109 cases, while the number of cases reported in both 2020 and 2021 was only 4.
Reports that investigated the epidemiology of measles in Jazan are currently lacking. In a nationwide study that assessed measles trends in SA between 2009 and 2012, it was concluded that Jazan represents one of the regions where measles cases are concentrated.51 An earlier report indicated that measles vaccination was introduced in SA in 1982 and aided in the control of measles infection in the country.52 Nonetheless, the persistence of the infection, including in Jazan, indicates issues related to vaccination coverage, vaccination effectiveness (such as vaccine failure), or reduction of measles seropositivity, especially among older susceptible individuals.
On a global basis, one of the most important issues associated with the incidence of measles is related to the use of vaccination to avert serious consequences of the disease. According to the WHO, an estimated 128 thousand deaths occurred worldwide during 2021, where the majority of these fatalities occurred among unvaccinated or under-vaccinated children.53 Despite the efforts dedicated to achieving the global elimination of measles, the proportion of infants who received the first dose of a measles-containing vaccine dropped from 86% in 2019 to 84% in 2020, where this reduction was mostly related to disruption of vaccine delivery due to the COVID-19 pandemic. Furthermore, vaccine hesitancy has been indicated as a factor contributing to the overall reduced immunization against measles and the reappearance of measles cases in countries which achieved verified elimination of the disease.54
According to the statistical yearbooks of the Saudi MoH, a total of 439 cases of bilharziasis were reported in Jazan between 2006 and 2021, representing 10% of all reported cases of the disease in the country during that period. The number of reported cases of bilharziasis in Jazan between 2006 and 2021 is fluctuant. For example, only 2 cases were reported in 2019 and 2020 (one case for each year), and 15 cases were reported in 2021 in Jazan. An earlier investigation published in 1997 records bilharziasis control activities carried out in Jazan, such as integrating bilharziasis control into primary healthcare services, active case detection via detection of the ova among children in schools and at-risk communities, treatment of identified cases, and chemical snail control.55 Nonetheless, it has been indicated that despite the success of the Saudi government in reducing the incidence of bilharziasis in the country due to the improvement of the irrigation systems, the southwestern regions of the country, namely Jazan and Aseer, remain at risk of the disease due to their proximity to Yemen, where bilharziasis control efforts are less effective.56 Nonetheless, further studies assessing specific risk factors of infection with bilharziasis in Jazan are currently lacking.
Bilharziasis is prevalent in tropical and subtropical areas, mostly in poor areas with limited access to safe water and inadequate sanitation. According to the WHO, 251.4 million individuals needed preventive treatment for bilharziasis in 2021, where the majority of them are living in African countries.57 Despite the global effort aiming for the eradication of the disease, economic and environmental factors, limited awareness regarding the risk of infection, and vector control challenges have been indicated as factors associated with the reduced effectiveness of the disease elimination efforts.58
Communicable diseases with a relatively low incidence in comparison with other regions in the country
There are several other notifiable communicable diseases that have low incidences in the region in comparison with other regions in the country. These diseases can be classified according to the total number of cases reported between 2006 and 2021 in the region into 2 classes: Firstly, diseases with a cumulative number of cases varying between 1,000 and 100, including cutaneous leishmaniasis, salmonellosis, hepatitis A, hepatitis C, and amoebic dysentery; secondly, diseases with a cumulative number of cases of less than 100, including mumps, rubella, whooping cough, tetanus, typhoid and paratyphoid, shigellosis, meningitis, and leprosy.
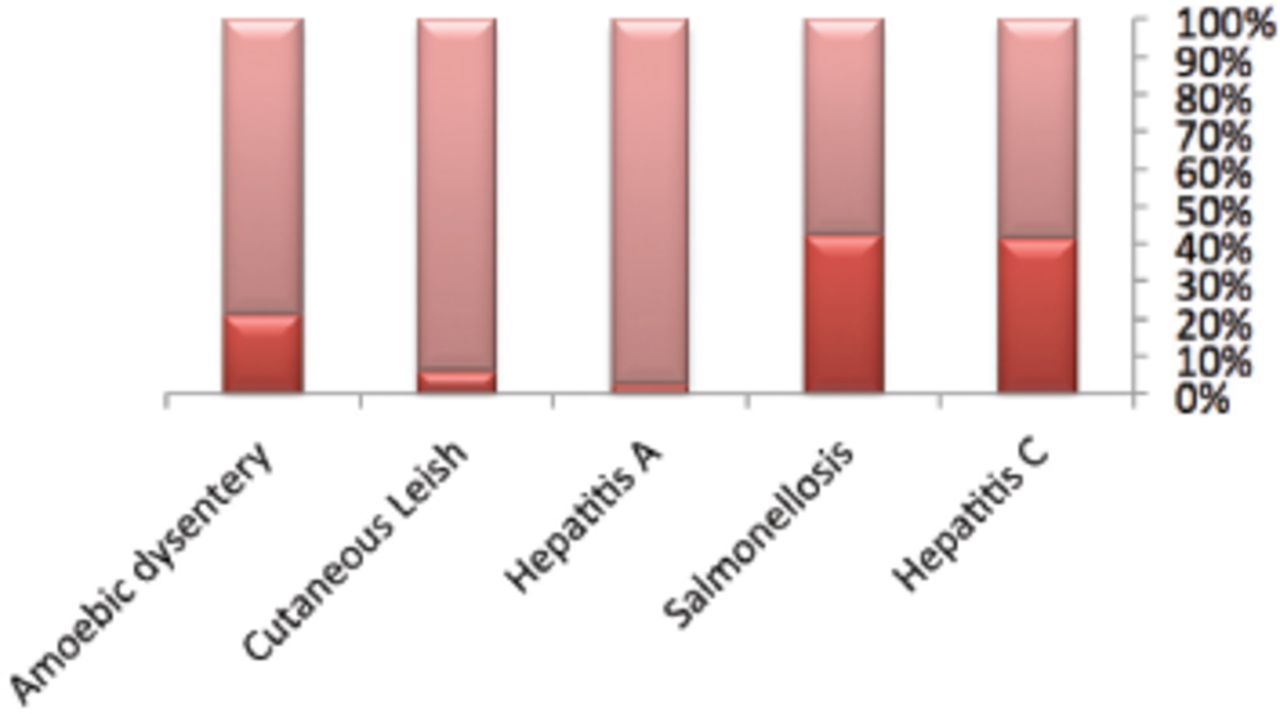
Figure 3 describes the proportions of cutaneous leishmaniasis, salmonellosis, hepatitis A, hepatitis C, and amoebic dysentery in the last 5 years in comparison with the total number of cases of these conditions reported in the period between 2006-2021. The figure indicates that 40% of all salmonellosis and hepatitis C cases that were reported in Jazan were reported in the years between 2017-2021, indicating a surge in the incidence in the last few years.
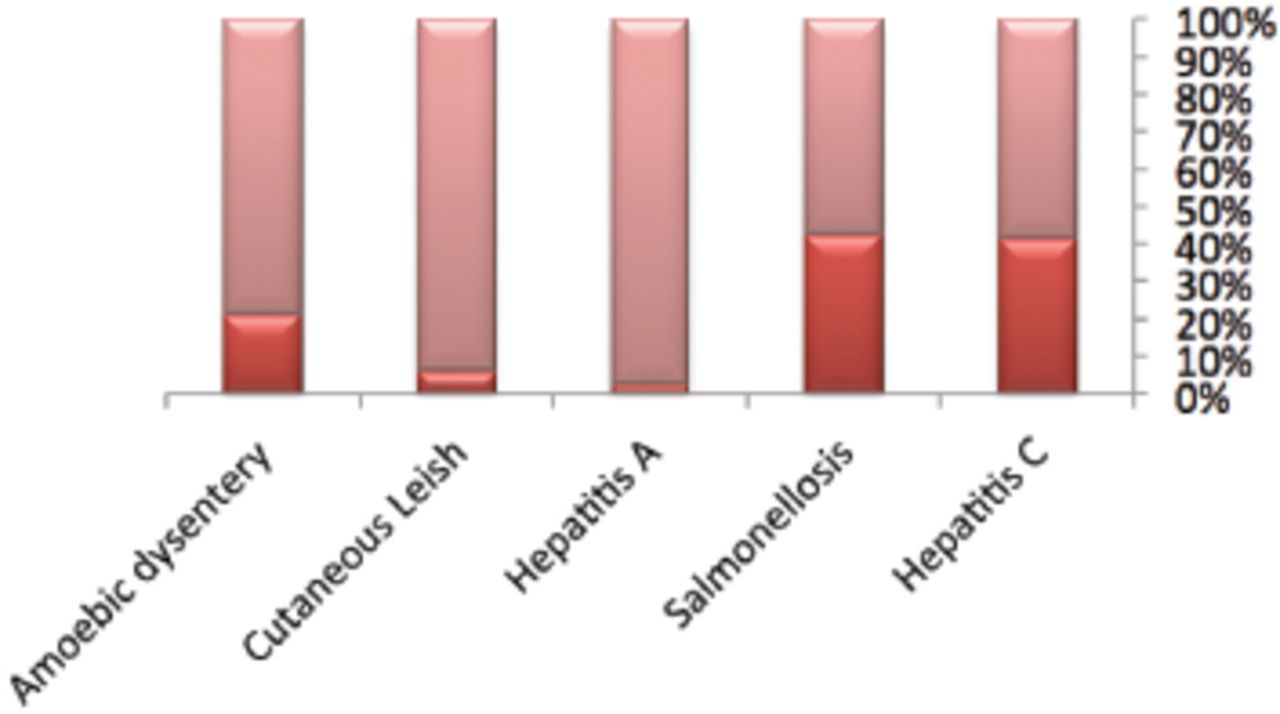
- Proportion of cases reported between 2017 and 2021 according to the total reported cases between 2006 and 2021 in Jazan region.
It can be noted that the surge of salmonellosis in the region during the COVID-19 pandemic period in Jazan is contradictory to the incidence of the disease in other regions, such as the European Union countries where the incidence of salmonellosis was stable before the pandemic and was significantly lower during the pandemic.59 This reduction can be partially attributed to the application of curfews in several countries and the limited movement and traveling of individuals.
The WHO reported that hepatitis C is a prevalent condition worldwide where the highest burden of hepatitis C is present in the Eastern Mediterranean region and Europe.60 The recent increase in hepatitis C cases in Jazan is consistent with the global increase of the disease in recent years. A systematic review and meta-analysis that involved 230 articles reporting hepatitis C records from 51 countries indicated an increase of the incidence from 0.8/1000 person-years in 1989 to 14.1/1000 person-years in 2021, where this increase was variable between countries and has been reported to be associated with the prevalence of HIV infection indicating an urgent need for early case detection, behavioral counseling, and provision of prompt treatment of affected cases.61
Amoebic dysentery witnessed a similar increase in incidence in the last few years but with a smaller magnitude, while the incidence of cutaneous leishmaniasis and hepatitis A decreased in the last few years. Factors associated with the increased incidence of hepatitis C, salmonellosis, and dysentery in Jazan during the years between 2017-2021 are not known, representing an area for further investigation. Nonetheless, the statistical yearbooks of the Saudi MoH indicate that the reported salmonella cases are sporadic cases and not the results of outbreaks.
Prevention and control efforts that led to the elimination of Rift Valley fever
The first Rift Valley fever outbreak was announced in Jazan in the year 2000; exposure to infected animals (such as goats and sheep) was the main risk factor for infection.62 The occurrence of the outbreak in Jazan was preceded by the incidence of the disease in Yemen, indicating the spread of the disease from the northern regions of Yemen to Jazan.63 The establishment of the Rift Valley fever control program in SA facilitated the reduction of the incidence of cases and led to the final elimination of the disease. The preventive efforts were related to vector control through insecticides, swamp drainage, and host control targeting susceptible herds such as seasonal surveillance, vaccination, and serological assessment of imported animals at the borders with Yemen.64 The Saudi MoH statistical yearbooks of the years between 2009-2021 indicate no detection of Rift Valley cases either in Jazan or any other region of the country, indicating the success of disease control in the country.
In conclusion, prevention and control efforts in Jazan were successful in the elimination of Rift Valley fever and in reducing the number of locally acquired malaria and chickenpox cases. Hepatitis B, dengue fever, and pulmonary TB have exhibited an increased incidence in recent years, suggesting a need for further epidemiological investigations to identify risk factors and modes of transmission in the region and further assessment of the need to apply relevant preventive measures. Finally, among the diseases that have relatively lower frequencies in the region, hepatitis C, salmonellosis, and dysentery have exhibited a surge in the last 5 years, indicating an area for further research and assessment.
Acknowledgment
The author gratefully acknowledges Proofed Inc. for their English language editing.
Footnotes
Disclosure. Author has no conflict of interests, and the work was not supported or funded by any drug company.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.