


Abstract
Objectives: To investigate the analgesic effect of a subcostal-posterior transversus abdominis plane (TAP) block combination following laparoscopic sleeve gastrectomy.
Methods: This study was conducted at Fatih Sultan Mehmet Educational and Research Hospital, Istanbul, Turkey, between March 2014 and June 2015. A total of 40 patients with a body mass index of 40-60 kg/m2 scheduled for laparoscopic sleeve gastrectomy were randomly allocated into 2 groups. Patients in Group I (n=20) received a bilateral subcostal TAP block, and patients in Group II (n=20) received a bilateral subcostal and posterior TAP block. Pain intensity was assessed at rest and during coughing using the visual analog scale (VAS) prior to and at various time points after TAP block (0 min, 30 min, 2 hours, 4 hours, 6 hours, 12 hours, and 24 hours). Morphine consumption over 24 hours and time to first morphine requirement were recorded.
Results: There was no difference in VAS scores between groups. Morphine consumption was 6.78±5.95 mg in Group I, and 7.28±5.95 mg in Group II (p=0.795). Time to first morphine requirement was 267.22±303.84 min for Group I, and 207.80±209.81 min for Group II (p=0.154).
Conclusions Subcostal-posterior TAP block provided equivalent analgesia to subcostal TAP block alone following laparoscopic sleeve gastrectomy.
An increasing number of people are undergoing surgery to lose weight and manage the complications of morbid obesity. Although bariatric surgery is generally performed laparoscopically, pain management has focused on reducing complications and improving patient comfort.1 Pain can be moderate to severe in the early postoperative period following bariatric surgery.2 Pain experienced during and after surgery can result in sensitivity or over-sensitivity to pain, and post-operative acute pain can become chronic.3 Morbidly obese patients are predisposed to opioid-induced airway obstruction and respiratory depression, which can make pain control following bariatric surgery challenging.3-5 Morbidly obese patients require a multimodal analgesic technique that can offer pain management without detrimental respiratory effects. A transversus abdominis plane (TAP) block is an efferent block of the anterior abdominal wall that can reduce pain and morphine use following lower abdominal surgery.6,7 The anterolateral abdominal wall is innervated by the thoracolumbar nerves (T6-L1) that give rise to both lateral and anterior cutaneous branches. The T6-T12 nerves run anteriorly through the TAP into the rectus sheath, and emerge as anterior cutaneous nerves.8 Traditional posterior TAP block provides effective pain relief below the level of the T10 dermatome, but often fails to block areas above the umbilicus.9 The use of a subcostal TAP block to alleviate supraumbilical abdomen pain is an adequate postoperative analgesic technique for upper abdominal procedures.9-12 The TAP is a wide space and is larger in obese patients. Carney et al13 found that the anterior subcostal approach provides anterior spread of contrast within the TAP (as detected with MRI), while the posterior approach results in predominantly posterior spread of contrast. The combination of subcostal and posterior blocks may cover a larger area in the TAP. This study investigated the use of a subcostal-posterior TAP block combination, relative to a subcostal TAP block alone, for analgesia following laparoscopic sleeve gastrectomy.
Methods
The study was approved by the Fatih Sultan Mehmet Educational and Research Hospital Ethical Committee (2014/03). All participants provided written informed consent. The randomized clinical trial was conducted between March 2014 and June 2015, and included 40 patients with a body mass index (BMI) of 40 to 60 kg/m2, 18 years of age or older, and scheduled for laparoscopic sleeve gastrectomy. Criteria for exclusion included a history of alcohol or drug dependence/abuse, history of opioid intake or chronic pain disorder, and contraindications to peripheral nerve block such as allergy to local anesthetics, coagulopathy, or infection in the area.
A closed envelope technique was used to randomly allocate patients into 2 groups. Patients in Group I (n=20) received a bilateral subcostal TAP block, and patients in Group II (n=20) received a bilateral subcostal and posterior TAP block. All surgeries were performed by the same surgeon. Patients were not premedicated. After monitoring heart rate, non-invasive blood pressure, peripheral oxygen saturation, and bispectral index (BIS), anesthesia was induced using propofol (2-3 mg/kg; Fresenius Kabi, Uppsala, Sweden), fentanyl (2 µg/kg; Vem İlaç; Tekirdağ, Turkey) and rocuronium (0.5 mg/kg; Koçak Farma, Tekirdağ, Turkey). All doses used for general anesthesia were calculated using adjusted body weight (ideal body weight + excess weight × 0.4). After tracheal intubation, anesthesia was maintained by total intravenous anesthesia with continuous propofol (3-6 mg/kg/h) and remifentanil (0.25-1 µg/kg/min; Vem İlaç; Tekirdağ, Turkey) administered with standard infusion pumps to maintain a BIS reading of 40 to 60 during surgery. Mechanical ventilation with a ratio of 40 to 60 oxygen-air mixture was used to maintain normocapnia. The surgeon applied 4 mL of 0.25% bupivacaine to each trocar insertion site prior to incision. The intra-abdominal pressure was set at a maximum level of 15 mm Hg during surgery. Prior to the end of the surgery, patients received paracetamol (1 g; Aroma İlaç; Tekirdağ, Turkey), tramadol (100 mg; Mefar İlaç; İstanbul, Turkey) and intravenous morphine (0.1 mg/kg; İdol İlaç; İstanbul, Turkey).
Intervention
An ultrasound-guided TAP block was performed using 30 mL of 0.2% bupivacaine (Vem İlaç; Tekirdağ, İstanbul) at each injection site. A linear ultrasound probe (Famio 8; Toshiba; Shimoishigami, Otawara-Shi, Japan) was used for the TAP block. For the posterior approach, the probe was placed transversely in the midaxillary line between the iliac crest and costal margin. The external oblique, internal oblique, and transversus abdominis muscles were visualized. For the subcostal block, the probe was placed obliquely on the upper abdominal wall along the subcostal margin near the midline. After identifying the rectus abdominis muscle, the probe was gradually moved laterally along the subcostal margin to identify the transversus abdominis muscle lying posterior to the rectus muscle. The external and internal oblique muscles were also visualized. A Pajunk needle (22-gauge, 10 mm; Medizintecknik; Geisingen, Germany) was introduced anteriorly in the plane for both techniques. The needle entered the fascia between the internal oblique and transversus abdominis muscles; 2 mL of 0.9% saline (İmaretçioğlu İlaç; Samsun, Turkey) was injected to verify proper positioning of the needle. Following negative aspiration, 30 mL of 0.2% bupivacaine was injected into the fascia. The spread of the injected solution was observed as a dark oval shape between the 2 muscles. For the posterior TAP block, an assistant was required to pull away the abdomen. Patients received patient-controlled analgesia (PCA) with morphine, following TAP block. The PCA pump was programmed to deliver a bolus dose of 1 mg morphine with a 15-min lockout and no background continuous infusion.
Outcome
Prior to surgery, patients were instructed on the use of the 10 cm visual analog scale (VAS) to grade their pain from 0 (no pain) to 10 (most severe pain). Pain intensity was assessed at rest and during coughing prior to and at various time points after TAP block (0 min, 30 min, 2 hours, 4 hours, 6 hours, 12 hours, and 24 hours). Patients were observed in the recovery room for 30 min following TAP block. Patients received 100 mg tramadol intravenously as a rescue analgesic if VAS exceeded 3. Morphine consumption (24 hours), time to first morphine requirement, rescue analgesic required (yes/no), incidence of postoperative nausea and vomiting (PONV), and patient satisfaction with analgesia score were recorded. Time to first morphine requirement was defined as the time the patient received the first PCA dose of morphine following discharge from the recovery room. No prophylactic antiemetic was administered. The incidence of PONV during the study period was recorded as none, mild, moderate, severe, and very severe. Patient satisfaction with analgesia was evaluated 24 hours after TAP block using a 5-point Likert scale (5: excellent; 4: good; 3: fair; 2: poor; 1: bad). Patients were monitored for any signs of adverse effects such as local site infection, hematoma formation, local anesthetic toxicity due to intravascular injection (dizziness, tinnitus, perioral numbness, lethargy, seizures, and signs of cardiac toxicity), extension of the block to the femoral nerve, peritoneal perforation, and bowel perforation. Patients had their abdomens covered with dressing after the application of the block. Data collection was performed by an anesthesiologist who was not aware of the group allocations.
Sample size
A pilot study was conducted with 5 patients in each group. Postoperative morphine consumption was 7.00 ± 1.22 mg for Group I and 5.00±1.58 mg for Group II. The power analysis determined that 19 patients were required in each group to reject the null hypothesis of equal morphine consumption in the 2 groups with a probability (power) of 0.90. The probability of type I error associated with this test was 0.05. To account for the possibility of lack of data collection and exclusion from the study, 20 patients were included in each group.
Statistical analysis
Data analysis was performed using the Statistical Package for Social Sciences Version 16.0 (SPSS, Chicago, IL, USA). According to the Kolmogorow-Smirnow normality test, a t-test was used for homogenous variables such as age, height, weight, BMI, duration of surgery, morphine consumption, and time to first morphine requirement. Heterogeneous variables (VAS scores) were analyzed using the Mann-Whitney U-test. The Chi-square test was used for PONV and patient satisfaction, and Fisher’s exact test was used for gender, ASA score, and requirement for rescue analgesic. A p-value <0.05 was considered statistically significant.
Results
All patients in each group completed the study. Both groups had similar demographic characteristics (Table 1). Both groups had similar VAS scores (Figures 1 & 2), which were lower (at rest and during coughing) after than before TAP block (p=0.000). Morphine consumption did not differ significantly between the 2 groups (Group I: 6.78±5.95 mg; Group II: 7.28 ± 5.95 mg; p=0.795). Time to first morphine requirement was 267.22±303.84 min for Group I and 207.80±209.81 min for Group II (p=0.154). Requirement of rescue analgesic, incidence of PONV, and patient satisfaction scores were also similar for both groups (Table 2). No patients experienced local anesthetic toxicity.
Demographic variables and duration of surger

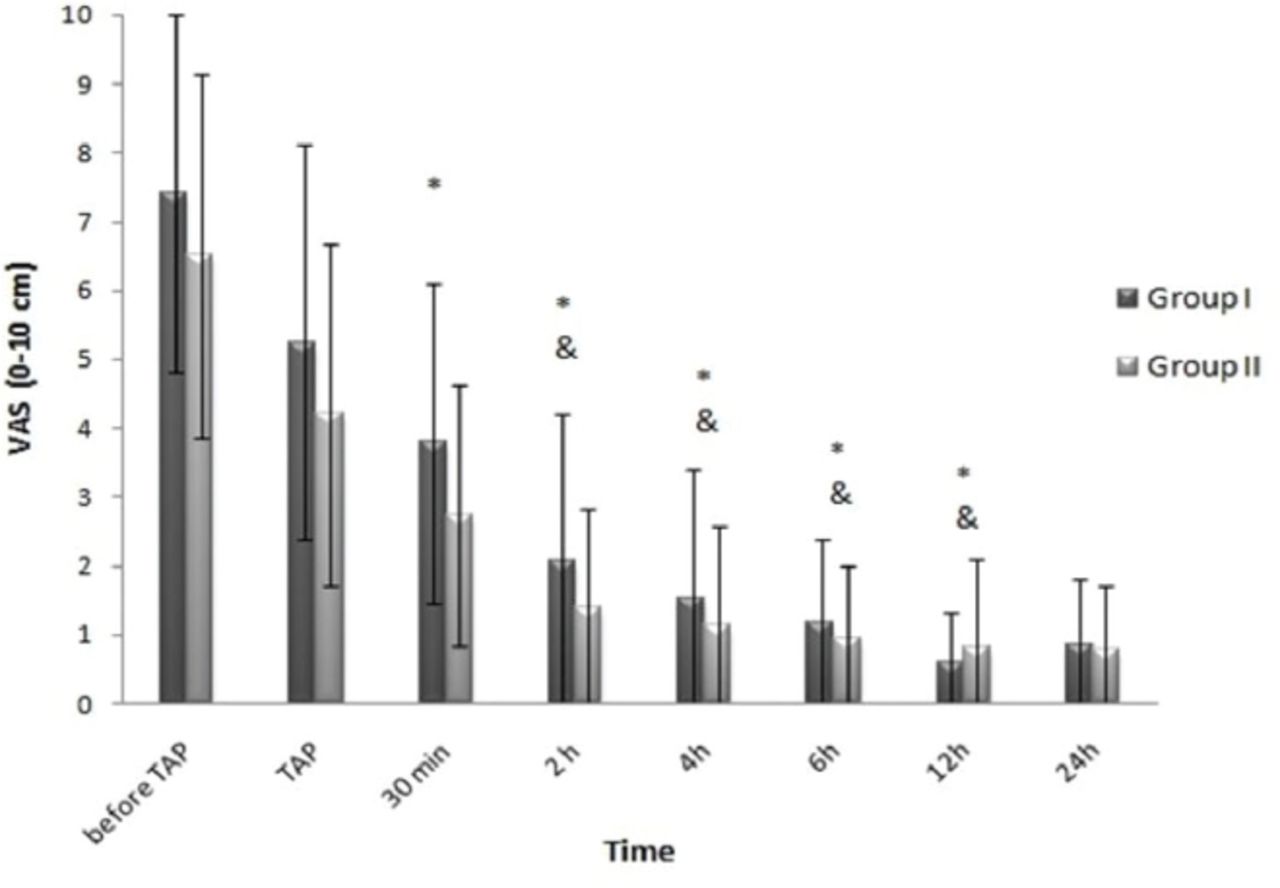
Comparison of VAS scores at rest between and within groups. *p<0.01 when compared with VAS score before TAP block (Wilcoxon test), &p<0.01 when compared to VAS scores at TAP block and 30 min after TAP block (Wilcoxon test)

Comparison of VAS scores during coughing between and within groups. *P <0.01 when compared with VAS score before TAP block (Wilcoxon test), &p<0.01 when compared to VAS scores at TAP block and 30 min after TAP block (Wilcoxon test).
Requirement for rescue analgesics, postoperative nausea and vomiting and patient satisfaction in Groups I and II.
Discussion
This study investigated the use of subcostal-posterior TAP block, relative to subcostal block alone, for analgesia. The 2 techniques provided equivalent analgesia following laparoscopic sleeve gastrectomy. Postoperative morphine requirement was minimal in both groups. Sinha et al5 performed ultrasound-guided posterior TAP block as part of a multimodal analgesic technique in morbidly obese patients undergoing laparoscopic bariatric surgery. They achieved superior postoperative analgesia with a posterior TAP block using 20 mL of 0.375% ropivacaine for each side. The block was performed at the end of the surgery, with the patient tilted 15° away from the block side and the abdomen pulled away by an assistant. There was no discussion of application of local anesthetic at the trocar site. In contrast, Albrecht et al2 found that bilateral TAP block did not provide additional analgesic benefit when combined with local anesthetic infiltration of the trocar insertion site for laparoscopic gastric bypass surgery. This conclusion is consistent with previous studies suggesting that TAP block is no more advantageous than trocar insertion site infiltration alone in patients undergoing laparoscopic cholecystectomy or appendectomy.14-16 Albrecht et al2 performed the block with a subcostal approach just after the induction of anesthesia, using 30 mL of 0.25% bupivacaine for each side. It is possible that the rise of intra-abdominal pressure in these obese patients, which was further increased by peritoneal insufflation in addition to the reverse Trendelenburg position, may have limited cephalad spread of the local anesthetic. As the increased intra-abdominal pressure and the use of the reverse Trendelenburg position remain constant, we combined the 2 approaches and injected 60 mL of local anesthetic solution into each side of the abdomen to improve the distribution of the anesthetic in the TAP. No beneficial effect of the combination was detected.
The effect of TAP block depends on the pattern of local anesthetic spread.16,17 The results of the study conducted by Lee et al16 showed that maximum dermatomal block distribution was observed at 30 min and usually regressed by 24 hours. In the present study, TAP block was performed after emergence from anesthesia, which allowed observation of the difference in VAS scores before and after the block. In agreement with Lee et al,16 we found that the analgesic effect was obtained within 30 min and lasted 24 hours. A previous study18 reported satisfactory analgesia with posterior TAP block following single-port sleeve gastrectomy; patients received the block upon arrival to the PACU and reached adequate analgesia levels within 30 min. The sensory block ranged from T5-L1 and the analgesia lasted for 12 hours.
Bhatia et al9 compared the subcostal and posterior approaches for TAP block after laparoscopic cholecystectomy. Although the subcostal and posterior TAP groups initially had comparable postoperative pain scores, the subcostal TAP block patients had markedly lower scores after 4 hours. Shin et al19 found that an oblique subcostal TAP block provides better analgesia than a posterior TAP block during the first 24 hours after laparoscopic cholecystectomy. Takimoto et al17 assessed the addition of upper and lower subcostal TAP block to lateral TAP block after laparoscopic cholecystectomy. Patients who received upper and subcostal TAP blocks, in addition to lateral block, had only marginal short-term analgesic benefit compared with patients who received the lateral block alone. The largest incision is usually at the umbilicus and subcostal TAP blocks are effective in the T7-11 region, which may explain the short-term benefit of the combination.17 In this study, the greatest analgesic effect of the subcostal block was in the region covering the surgical area, which could explain the lack of additional analgesic effect of a posterior TAP block. A 4-block approach to anesthetize both the upper and lower abdominal walls provided effective analgesia after major abdominal surgery.8 The analgesic efficacy of the block lasted 6 hours and allowed low opioid consumption on the first postoperative day and early mobilization.8 The shorter duration of the analgesic effect may be related to excessive tissue swelling and increased blood flow, resulting in a faster washout of the local anesthetics. Carney et al13 suggested that the mechanism of analgesia may be related to an effect in the paravertebral space or systemic analgesia due to intravascular absorption of the injectate. The opioid-sparing effect of TAP block decreases airway complications in obese patients. Nausea and vomiting is a major complication of opioid use. Reduced opioid use decreases the occurrence of this complication.
No complications related to the TAP block were observed. The lack of observed complications does not imply that TAP block is free of potential complications. The use of ultrasound provides direct needle visualization and reduces the incidence of complications such as visceral or vascular injury; it also allows for reduced local anesthetic doses, although the risk for local anesthetic systemic toxicity (LAST) remains constant.20 The systemic absorption and peak plasma levels of local anesthetic after TAP block in bariatric surgery has not been investigated. It is possible that morbid obesity may confer an additional margin of safety against LAST given the large potential volume of distribution.2 Gravante et al21 found that obese patients require higher local anesthetic doses compared with non-obese patients, and Araco et al22 stated that patients with a higher BMI were likely to fail block; technical failure is unlikely in this case as it was the surgeon who injected the local anesthetic in the TAP under direct vision. The TAP is a wide space and is larger in obese patients. An adequate volume of local anesthetic solution is crucial to obtain adequate analgesic effect. In this study, the addition of a posterior TAP block was expected to prolong the analgesia duration; however, we observed no difference in the time to first morphine requirement between the groups.
Study limitations
This study was limited by its small sample size. As plasma levels of local anesthetics were not measured, we could not compare differences in local anesthetic toxicity between the 2 groups. The distribution of sensory block was also not assessed.
Further studies with larger sample size should focus on determining optimum effective dose and volume of local anesthetic. Studies on plasma levels and systemic absorption of local anesthetics will also be beneficial to clarify possible mechanisms of action of TAP block.
Compared with subcostal TAP block alone, subcostal-posterior TAP block did not provide improved analgesia following laparoscopic sleeve gastrectomy.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 8, 2017.
- Accepted September 12, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}