


Abstract
Objectives: To translate and linguistically validate the urticaria control test (UCT) to/for Arabic speakers. No Arabic version of the UCT is available to assess disease control in patients with chronic urticaria (CU). Secondary objectives were to assess disease control in Lebanese CU patients and determine influence factors.
Methods: This is a prospective observational study of 178 CU patients diagnosed during their first visit to a private Allergy/Immunology Clinic, Hotel Dieu de France Hospital, Beirut, Lebanon between January and December 2014.
Results: Factor analysis showed that all 4 UCT items on the Arabic version converged over a solution of one factor. A high internal consistency was found with a Cronbach’s alpha of 0.824. Most patients in this study had chronic spontaneous urticaria (96%), of which 19% also had inducible urticaria. The majority was <40 years (67.4%), with disease duration of <2 years (70.8%). Most patients used H1-antihistamines, but unfortunately, 34.3% used systemic glucocorticosteroids, of which 24.7% also used H1-antihistamines. The disease was poorly controlled in most patients (79.2%, UCT <12). Age, gender, duration, diagnosis, triggers, and/or history of atopy had no influence.
Conclusion: We developed the first linguistically validated Arabic UCT to improve CU management in Arabic speaking patients. We also found that disease control was poor in most CU patients, and is unaffected by age, disease duration, gender, subtype, triggers, history of atopy, and/or previous treatments.
Chronic urticaria (CU) is a common skin disorder characterized by recurrent pruritic wheals, angioedema, or both that occur for more than 6 weeks affecting up to 1% of the total population.1,2 It can be distinguished into chronic spontaneous urticaria (CSU) and chronic inducible urticarias (CIndUs). All sub forms of CU can be challenging conditions for affected patients and their treating physicians. The signs and symptoms of CU, particularly of CSU, usually vary strongly from day to day and considerably affect the patient’s quality of life.3,4 Therefore, the clinical presentation of a patient during a doctor’s visit is almost never representative of the actual current situation of the disease. This makes it difficult for physicians to estimate patients’ disease activity and disease burden, and to adjust treatment to the current needs. To overcome this obstacle, several patient-reported outcomes (PRO) measures have been developed for CU patients in the past few years,5,6 including the Urticaria Activity Score (UAS),1,5 the Angioedema Activity Score (AAS),7 Chronic Urticaria Quality of Life questionnaire (CU-QoL),6,8 the Angioedema Quality of Life Questionnaire (AE-QoL),9,10 the Urticaria Severity Score,4,11-13 and the Urticaria Control Test (UCT). Of these PROs, the UCT is the easiest and quickest tool. It was the first questionnaire for assessing disease control in patients with CU and it has been found to exhibit high levels of validity and reliability.3,14,15 The disease control assessment in CU helps decide if the patient’s current treatment is sufficient or needs to be intensified, but also helps to get an overview of the patient’s disease status and disease burden.3 The treatment of patients with CU should be targeted toward controlling the signs and symptoms of CU, reducing its impact on patients’ quality of life, and minimizing the medications’ adverse effects.1,3 The UCT can be used in all adult patients with chronic urticaria (CSU and CIndUs) and is recommended for each patient visit.3 In addition to serving as a useful tool to detect patients with poorly controlled disease symptoms, it may also be used to monitor disease status over time, and to guide treatment decisions.3
The primary objective of this study was to translate the UCT to Arabic, linguistically validate it for use in CU patients in Lebanon, and to check the reliability of the Arabic version. The secondary objectives of this study were to assess disease control in Lebanese CU patients using the UCT, and to analyze the impact of patients’ age, disease duration, diagnosis, trigger factors, history of atopy, and treatments on disease control.
Methods
Translation and linguistic validation of the Arabic UCT version
In order to obtain a linguistically validated Arabic version of the UCT,16 a structured forward-backward translation with subsequent patient testing was performed. The American-English and the German versions of the UCT were translated to Arabic by a professional translator, and the Arabic version was subsequently back-translated to English and German by another professional translator. The translators compared the original versions and the back-translations of the UCT to determine whether the instructions, items, and answer keys kept their meaning during the translation process; discrepancies were resolved by consensus measures. Finally, a pilot test was conducted with 15 patients to check if the Arabic UCT version was well understood.
Assessment of disease control in Lebanese CU patients
In order to assess the construct validity and internal consistency reliability of the UCT, as well as disease control in Lebanese CU patients (both CSU and CIndUs), a prospective observational study was conducted between January and December 2014. It included 178 patients diagnosed with CU during their first visit to a private Allergy/Immunology clinic located in Beirut. The diagnosis of CU was based on clinical history of itchy urticarial lesions or angioedema, occurring for more than 6 weeks, and by physical examination of those lesions if present at the time of the patient visit. Patients under the age of 14 years as well as illiterate or non-Arabic speaking patients who could not complete questionnaires were excluded from the study. The UCT was distributed in the private clinic to patients after verbal informed and written consent was obtained.
Participants were asked to complete all 4 questions (items) of the Arabic UCT to evaluate the physical symptoms of the disease (item 1), the associated quality of life impairment (item 2), the effectiveness of treatment (item 3), and the overall level of disease control management (item 4) during the past 4 weeks. Every item of the UCT has 5 answer options (5-point Likert scale) that are scored from 0 to 4 points, with higher scores indicating better levels of disease control. The UCT total score ranges from 0 to 16 points, with a score of 12 or more indicating a well-controlled disease, whereas a score of less than 12 reflects poor disease control and the need for better treatment.3 In this study, patients’ data was dichotomized accordingly.
Ethical considerations
The Institutional Review Board of the University, Faculty of Pharmacy, Beirut, Lebanon waived the need for an approval based on the facts that it was an observational study that respected participants’ autonomy and confidentiality, induced minimal harm, and followed the principles set out in the Declaration of Helsinki for such studies.
Subjects were asked to fill a questionnaire regarding their general health and were not aware of the exact objective of the study; written consent to provide the information was required. Patients were reassured that if they refused to participate in the study, there would be no consequence whatsoever on their medical care. The information on previous treatment and atopy was collected as part of the patient’s history. The questionnaire was structured in line with those usually undertaken when evaluating chronic urticaria in patients. Furthermore, data analysis respected patients’ anonymity.
Statistical analysis
Data entry was performed by a medicine intern using Excel; patients’ names were removed upon entry. Data analysis was performed by one of the investigators on the Statistical Package for the Social Science software, version 23 (IBM Corp., Armonk, NY, USA). To confirm the construct validity of the Arabic UCT, a factor analysis was performed using the principal component analysis technique, with a promax rotation as the extracted factors were found to be significantly correlated. The Kaiser-Meyer-Olkin measure of sampling adequacy and Bartlett’s test of sphericity were used to ensure adequacy. The retained number of factors corresponded to Eigen values higher than one. Out of all the items asked in the questionnaire, we assessed whether items were over-correlated to each other (the items that are dependent from each other) (r >0.9), whether they had a low loading on factors (how each variable weighed for the factor in question) (r <0.3), or whether they had a low communality (proportion of each variable’s variance that can be explained by the factors) (r <0.3). Moreover, Cronbach’s alpha was recorded for internal consistency reliability analysis for the total score and for subscale factors. The Chi-square test was used for bivariate analysis of categorical variables. A p-value of 0.05 was considered statistically significant.
Results
Patient sample characteristics
As expected from other epidemiologic studies of CU, the majority of participants were female (61%) and below 40 years of age (67.4%). Most patients were affected by CSU (75.8%), 19.7% had both CSU and an inducible form of CU, while 4.4% were solely affected by chronic inducible urticaria. The majority had a disease duration of less than 2 years (70.8%); 44.4% of the total sample had angioedema.
Construct validity and internal consistency of the Arabic UCT
The UCT was completed by all patients, and the factor analysis was ran over the whole patient sample (n=178). Out of all UCT items, no items were over-correlated to each other (r: >0.9), had a low loading on factors (r: <0.3), or had a low communality (r: <0.3). Thus, all of the original UCT items were kept in the Arabic version. The UCT items converged over a solution of only one factor that had an Eigen value over one, explaining a total of 66% of the variance. A Kaiser-Meyer-Olkin measure of sampling adequacy of 0.730 was found, with a significant Bartlett’s test of sphericity (p<0.001). A high internal consistency of the Arabic UCT version was found with a Cronbach’s alpha of 0.824 (Table 1).
Factor analysis of the urticaria control test questionnaire in the Lebanese population.
Chronic urticaria is poorly controlled in most patients
Analyzing the individual UCT items, CU caused very much (18.5%) and much physical discomfort (45.5%) of the patients. In only 23% of patients, quality of life was not affected (Table 2). Chronic urticaria treatment was reported to be a little (34.8%) or not at all effective (19.1%), and 25.8% of patients reported that their treatment was effective in controlling their disease (Table 2).
Urticaria control test (UCT) results among Lebanese participants.
The mean UCT score of the whole sample was 8.73 ± 3.08, with 141 patients (79.2%) reporting poor disease control according to the UCT (UCT score value of 11 or less; Figure 1). Stratified by CU subtype, the mean UCT score for patients with CSU was 8.70 ± 3.06, that of patients with CIndU was 8.74 ± 2.95, and that of patients with both CSU and CIndU was 8.71 ± 3.03.
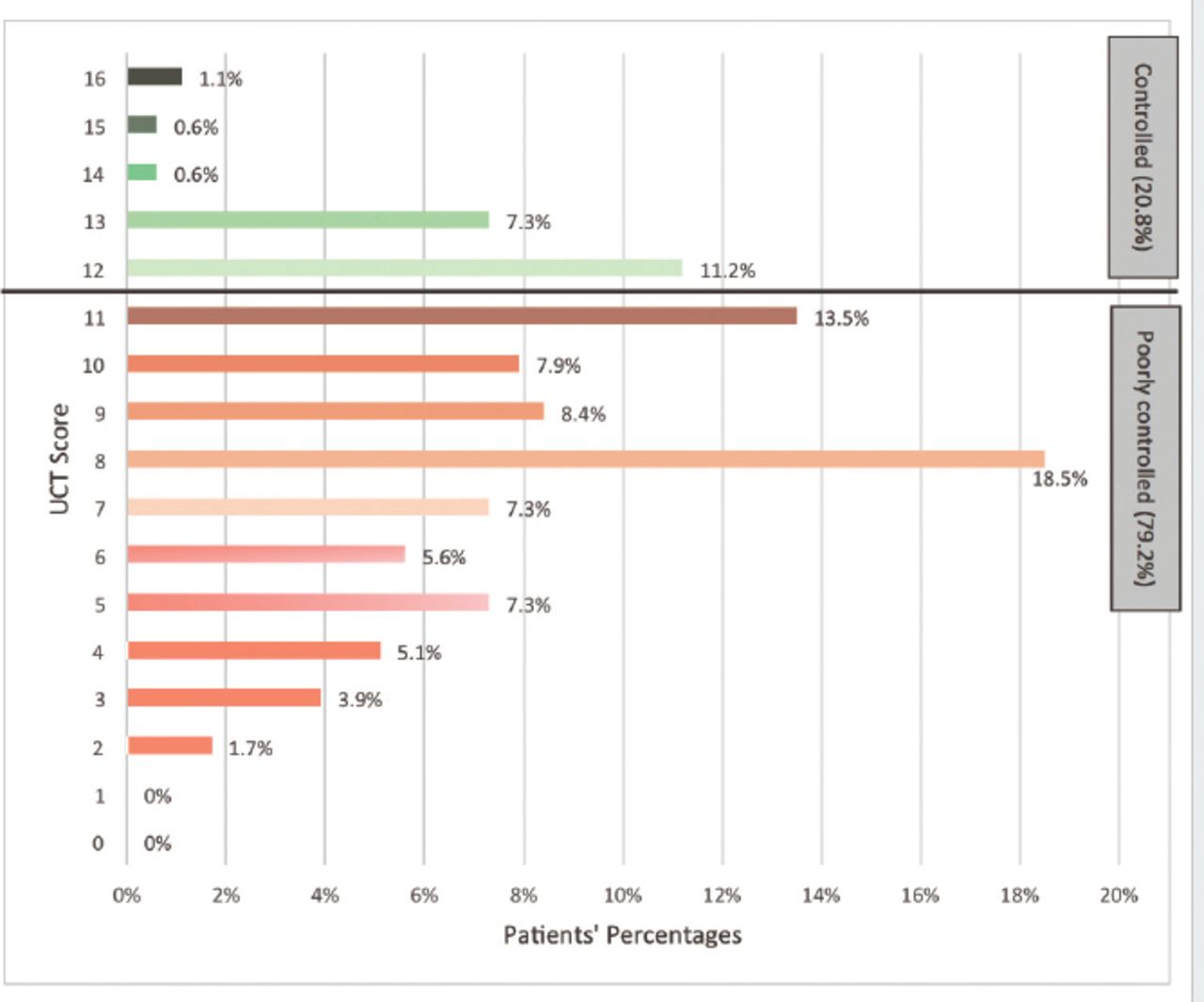
Percentages of patients according to their urticaria control test (UCT) score. Patients under 12 have an uncontrolled urticaria, while patients with a UCT score of 12 or more have a controlled disease.
Triggers of chronic urticarial
Most of the patients studied did not report relevant triggers of CU exacerbation. In some patients, physical triggers (6.2%) and certain foods (5.6%) were reported to increase disease activity. Moreover, 12.4% of patients were found to exhibit exacerbation of CU after nonsteroidal anti-inflammatory drugs intake. Thirteen patients (7.3%) had comorbidities identified by the doctor (atopic dermatitis, allergic rhinitis, asthma), while 41 (23%) patients had other reported comorbidities (allergy to antibiotics, anti-inflammatory drugs, aspirin, food).
Treatment of chronic urticarial
At the time of presentation, 93.3% of patients were on H1-antihistamine treatment. The H1-antihistamines used were mainly second generation drugs, but some patients took second generation antihistamines during the day and first generation antihistamines at bedtime (4.5% of cases). The doses used were either normal or up to twice the licensed dose. Sometimes combinations of 2 different H1-antihistamines were applied. Approximately 40% were on a single dose of non-sedating H1-antihistamines, 50% on higher than the licensed dose (using the same drug or 2 different drugs), and 4.5% used a combination of first generation (mainly hydroxyzine) and second generation H1-antihistamines. Every third patient (34.3%) received long-term oral glucocorticoid treatment (more than 10 days), out of which 44 (24.7%) were using both H1 antihistamines and glucocorticosteroids. None of the patients were on omalizumab (anti-IgE), leukotriene antagonists, or cyclosporine treatment (Table 3).
Current treatments in all patients with chronic urticaria at the time of visit.
Bivariate analysis for factors correlating with well controlled versus poorly controlled urticarial
Cross tabulation conducted among patients with poorly controlled CU (mean UCT: 7.67 ± 2.49) versus patients with well controlled CU (mean UCT: 12.76 ± 1.23) showed no significant difference between the 2 groups for any of the included variables (p>0.05): There was no influence from age, gender, disease duration, diagnosis, triggers, and/or history of atopy (Table 4). In addition, there were no major differences in the rates of control when we compared patients on different treatments. For example, among patients on H1 antihistamine monotherapy (n=109), only 15.6% had well controlled disease.
Bivariate analysis for controlled versus poorly controlled patients using the urticaria control test (UCT).
Discussion
In the current study, we linguistically validated the first Arabic version of the UCT questionnaire, with the intention of using it among patients with CU in Lebanon. The translation process was conducted by independent translators, the point that decreases the subjectivity of the UCT adaptation. In addition, our results provide initial evidence supporting the validity and reliability of the Arabic UCT. The construct validity was adequate because items converged over only one factor, with adequate factor loadings for all items. The internal consistency reliability for the Arabic UCT scale was high (Cronbach’s a=0.824), similar to the internal consistency estimated for the original version of the UCT (Cronbach’s a=0.84).3 These findings show that the reliability estimate (Cronbach’s alpha) of the Arabic UCT version is adequate and similar to the internal consistency reliability determined for the original version of the UCT.3
In our study, a female predominance (60.7% of patients with chronic urticaria were women) was found, with a high percentage aged between 21-40 years. This supports earlier studies that show that CU is more prevalent in female patients, occurring at a 2:1 female-to-male ratio, and that the peak incidence is between 20 and 40 years of age.2 In addition, in this study, 71% of patients had a disease duration of fewer than 2 years, and 22% between 2 and 10 years, which is compatible to what is found in the literature. Chronic spontaneous urticaria is estimated to last between one and 5 years with a mean duration of 3 to 5 years, but this is likely to be longer in more severe cases (concurrent angioedema and concurrent inducible urticaria).17,18 A small proportion of patients can have CSU for >20 years.19 The similarity of our sample’s sociodemographic and disease characteristics with those of the literature suggest that our population with CU is comparable to that of other countries and previous studies.
In our study, more than 90% of patients had CSU overall, with 19% of the CSU patients showing comorbidity of one more chronic inducible urticarias. Again, this is very similar to other CU patients populations studied.20 Furthermore, 44% of our patients reported recurrent angioedema, similar to the study of Axelrod et al21 showing that 50% of patients with CSU also experience concurrent angioedema.
In our study, 76% of patients did not have any history of allergies. Twenty-three percent of the patients reported having experienced allergic reactions to antibiotics, anti-inflammatory drugs, aspirin or food. In fact, NSAIDs and aspirin mainly cause “pseudo-allergic” reactions with IgE-independent mast cell activation. Chronic urticaria is not caused by food allergy. In contrast, it is assumed that intolerance to naturally occurring food ingredients, mainly aromatic compounds such as those found in fresh tomatoes, spices, or wine can contribute to the development of signs and symptoms of CSU.22
The EAACI/GA2LEN/EDF/WAO guideline for the management of urticaria recommends therapy for chronic urticaria to aim for complete symptom control.1 In terms of therapy, second-generation H1-antihistamines are the first-line treatment for chronic urticaria (namely, CSU and CIndU), and up-dosing H1-antihistamines to 4 fold is recommended for the management of patients who do not experience disease control on the standard dose.1 Second line treatment options, for antihistamine-resistant patients, include omalizumab and cyclosporine.16,23 In our study, almost all patients (93.3%) were on H1 treatment, mostly with non-sedating antihistamines used at standard or double dose, none were on omalizumab or cyclosporine, despite low rates of controlled disease. This shows that CU patients, in real life, are largely not treated according to guideline recommendations, which is in line with the results of other recent studies.23,24
Steroids should be reserved for coping with exacerbations of CU and only be used as short-term treatment.1 In Lebanon, patients frequently receive multiple courses of intramuscular steroids and long-term steroid treatment with an anti-histamine in the same tablet. Notably, one third of our patients were on long-term treatment, for example longer than 10 days, with glucocorticosteroids at a high dose (1 mg/Kg). Though effective, steroids do not result in cure or alter the disease course, which is precisely why they should not be used for the routine treatment of CU patients and only be reserved for a short period of time in cases of exacerbation.21
Although the preliminary results of this study show the utility of the translated UCT in Arabic-speaking patients suffering from CU, further research should explore the psychometrics of the Arabic UCT in larger studies; in fact, the small sample size and the geographic limitation are weak points of our study. Future studies should also involve other districts in Lebanon and the region, to be able to extend the results to the general population of Arabic speaking countries. No anchor instruments (that are validated yet) were applied so the convergent validity of the Arabic UCT could not be explored.
Since language barriers are an important obstacle to proper medical communication and management, translation of the UCT to Arabic and validation of the Arabic form was essential. The linguistically validated Arabic UCT can be used to screen Arabic-speaking patients for poorly versus well controlled disease. This may help physicians to better and reliably determine the patients’ disease status and therefore guide and document treatment decisions. This is particularly important since the results show that the majority of patients with chronic urticaria are suffering from poorly controlled disease. Larger prospective studies are needed to evaluate the effects of different treatment options on the control of chronic urticaria as well.
In conclusion, our study results demonstrate that the mean UCT score of all patients in this study was 8.7, which is clearly below the cutoff of 12 points for well controlled disease. Moreover, the UCT scores were not found to be different in the 3 observed patient groups (CSU, CIndU, and CSU plus CIndU), suggesting that the low level of CU control is independent of its subtype. Rates of uncontrolled disease were high across the entire study population and unaffected by age, gender, disease duration, triggers, and/or history of atopy. This indicates that insufficient therapy is a common problem that affects all subgroups of patients with CU.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 29, 2017.
- Accepted October 30, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.