


Abstract
Objectives: To investigate the relationship between metabolic control, acute and long-term complications, the coexistence of autoimmune diseases, and to assess the different factors that can affect the glycemic control level among children with type 1 diabetes mellitus (T1DM).
Methods: This is a cross-sectional study that included 228 T1DM children and adolescents visiting the pediatric diabetes clinic at the King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia from January 2013 to January 2014. The clinical and laboratory characteristics of the patients were recorded. Metabolic control, complications, and associated autoimmune diseases were evaluated.
Results: The mean age of patients was 10.99 years, and the glycated hemoglobin (HbA1c) level was 8.8%. Acute complications included ketoacidosis in 65.4% of patients, and hypoglycemic attacks in 68.9%. Long-term complications were detected in patients including retinopathy (4.4%), microalbuminuria (16.2%), and dyslipidemia (8.3%). Autoimmune thyroiditis was noted in 14%, and celiac disease was found in 19.7% of patients. A significant difference was found in pubertal and pre-pubertal age groups in terms of glycemic control (p=0.01).
Conclusion: The level of HbA1c was found to be higher among the pubertal age group. A relationship between autoimmune diseases and gender was determined.
Type 1 diabetes mellitus (T1DM) is one of the most common chronic diseases in pediatric patients. The incidence of T1DM among children is rising worldwide, and varies depending on different factors. The overall annual increase is estimated at 3% with approximately 70,000 children worldwide expected to develop T1DM every year.1 In Saudi Arabia, the reported prevalence in children and adolescents was 109.5/100000 in 2008.2 Type 1 diabetes mellitus is an autoimmune disease characterized by insulin deficiency due to destruction of pancreatic beta cells. Patients with T1DM are at high risk of developing other autoimmune diseases, such as autoimmune thyroiditis (AIT) and celiac disease (CD).3,4 Moreover, T1DM can lead to numerous complications in pediatric patients, with the most common acute complications including hypoglycemia, and diabetes ketoacidosis (DKA). Long-term complications in childhood include retinopathy, nephropathy, and dyslipidemia, among others. In this study, we aimed to assess the relationships between glycemic control, acute and long-term complications, associated autoimmune diseases,and to assess other different factors that can affect or predict the glycemic control level among children with T1DM visiting the pediatric diabetes clinic at King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia.
Methods
This is a retrospective cross-sectional study conducted in children and adolescents with T1DM, followed up at the pediatric diabetes clinic at KAUH from January 2013 to January 2014. The study population consisted of 228 children and adolescents with T1DM aged one to 18 years. The data were obtained from a questionnaire, and all laboratory findings were obtained from the KAUH Phoenix system. An informed verbal consent was acquired from the patients/parents. These data comprised clinicodemographic information, anthropometric measurements, and information regarding the status of the patients’ metabolic control, and the presence of other autoimmune diseases, or any acute and chronic complications. Patients with major data insufficiency due to incomplete questionnaires and those with secondary or monogenic diabetes, and/or polyendocrinopathies were excluded from the study. Glycated hemoglobin (HbA1c) is the most frequently used test to measure the glycemic control, and the goal is 7.5 or lower, independent of the patient’s age.5 The mean HbA1c reading obtained during the last year was used for each patient. All patients were divided into 3 groups according to the glycemic control as follows: good glycemic control (HbA1c <7%), moderate glycemic control (HbA1c 7-9%), and poor glycemic control (HbA1c >9%). Detection of AIT was based on physical examination and laboratory findings including the serum levels of free thyroxin (FT4), thyroid stimulating hormone (TSH), anti-thyroid peroxidase, and anti-thyroglobulin. The presence of at least one positive antibody in addition to low serum FT4 (normal range, 12-22 pmol/L) and high TSH levels (normal range, 0.27-5 mIU/L) was essential to establish the diagnosis.6 The diagnosis of CD was based on the presence of a high titer (≥20 IU/L) of IgA anti-tissue transglutaminase, confirmed by jejunal biopsy. Information regarding the acute complications of T1DM, such as DKA, and hypoglycemia were obtained from the information recorded in the questionnaires as the frequency of attacks per year. The presence of microalbuminuria was detected first by spot urine samples and confirmed by using 24-h urine samples. Microalbuminuria was defined as a urinary albumin excretion of 20-200 µg/min (30-300 mg/day) or an albumin/creatinine ratio of 2.5-25 mg/mmol in boys and 3.5-25 mg/mmol in girls in the morning urine sample.7 Retinopathy was diagnosed by the presence of microaneurysms, hemorrhage, exudates, microvascular abnormalities, or macular edema in the examination with ophthalmoscope by an opthalmologist.7 Cataract and error of refraction were also considered. Dyslipidemia was diagnosed by the following lipid profile measures: a low-density lipoprotein (LDL) of >100 mg/dl, high-density lipoprotein (HDL) of <35 mg/dL, and triglycerides (TG) of >150 mg/dL.8 Vitamin D deficiency was diagnosed by 25-hydroxyvitamin D levels of <20 ng/mL.9 Patients were divided into 4 groups according to age (<5 years, 5-10 years, 10-15 years, >15 years). Puberty was defined either by age with a cut-off level of 10 years in females, and 12 years in males, and/or by the appearance of stage 2 development of the breast in females, or testicular enlargement of more than 4 mL in males. Ethical approval for this study was obtained from the Research Ethics Committee of KAU Hospital.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics version 22.0 software (IBM Corp., Armonk, NY, USA). Continuous variables are represented as mean ± SD, and categorical variables as percentages. Student t-test was used for comparative evaluation of the continuous variables in each of the glycemic control groups; as our population was not normally distributed, we transformed the data to normalize the distribution. When appropriate, the Chi-square test and cross tabulations were applied for the analysis of categorical data. Logistic regression analyses were used to define other possible relations. P<0.05 was considered statistically significant for individual variables.
Results
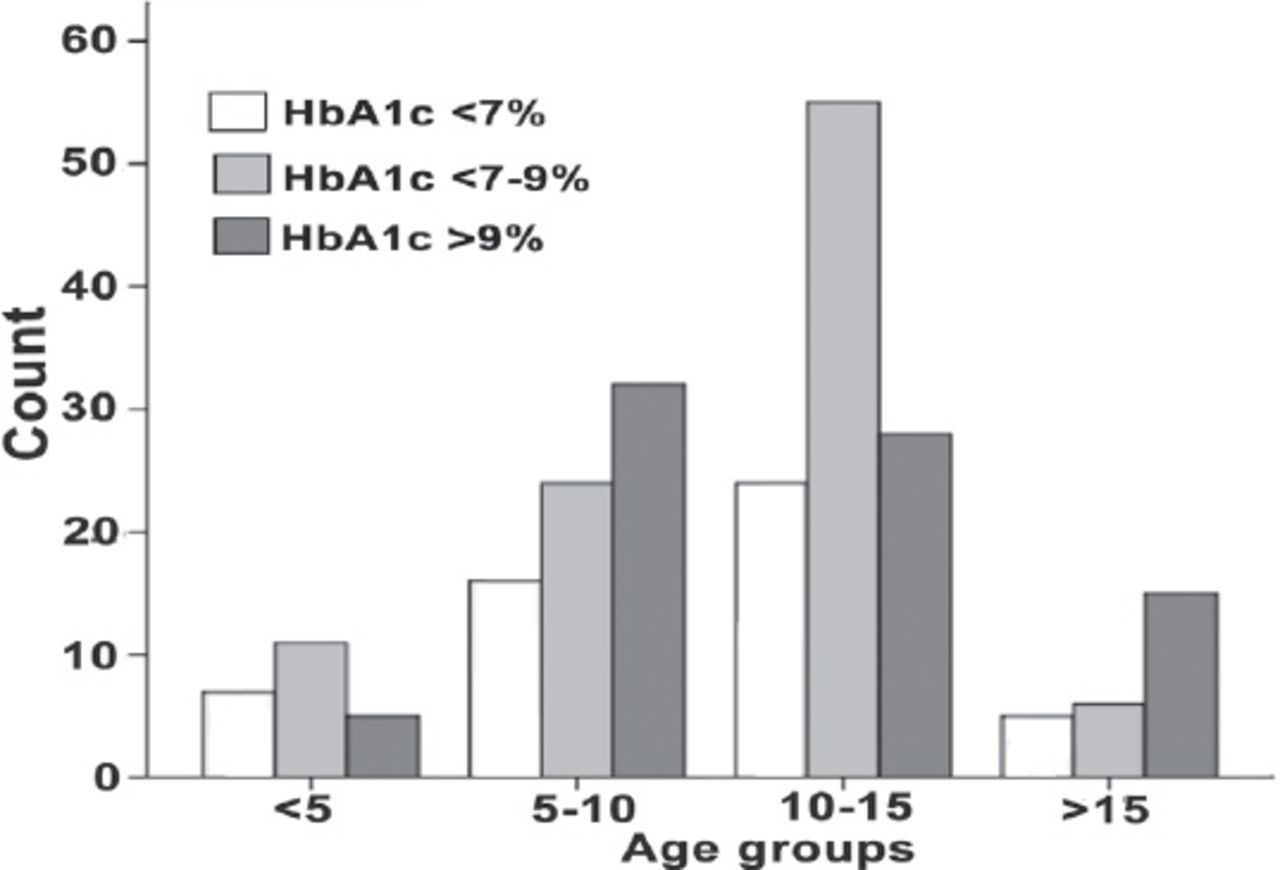
The study included 228 children and adolescents (mean age: 10.99±3.9 years; 38.2% males, 61.8% females), with most patients (47.3%) aged between 10-15 years. In the school age group (5-10 years) 70% were located in the poor control group (HbA1c >9), moreover in the age group of post puberty (>15 years) 57.7% was again presented in the poor control group (Figure 1, Table 1).
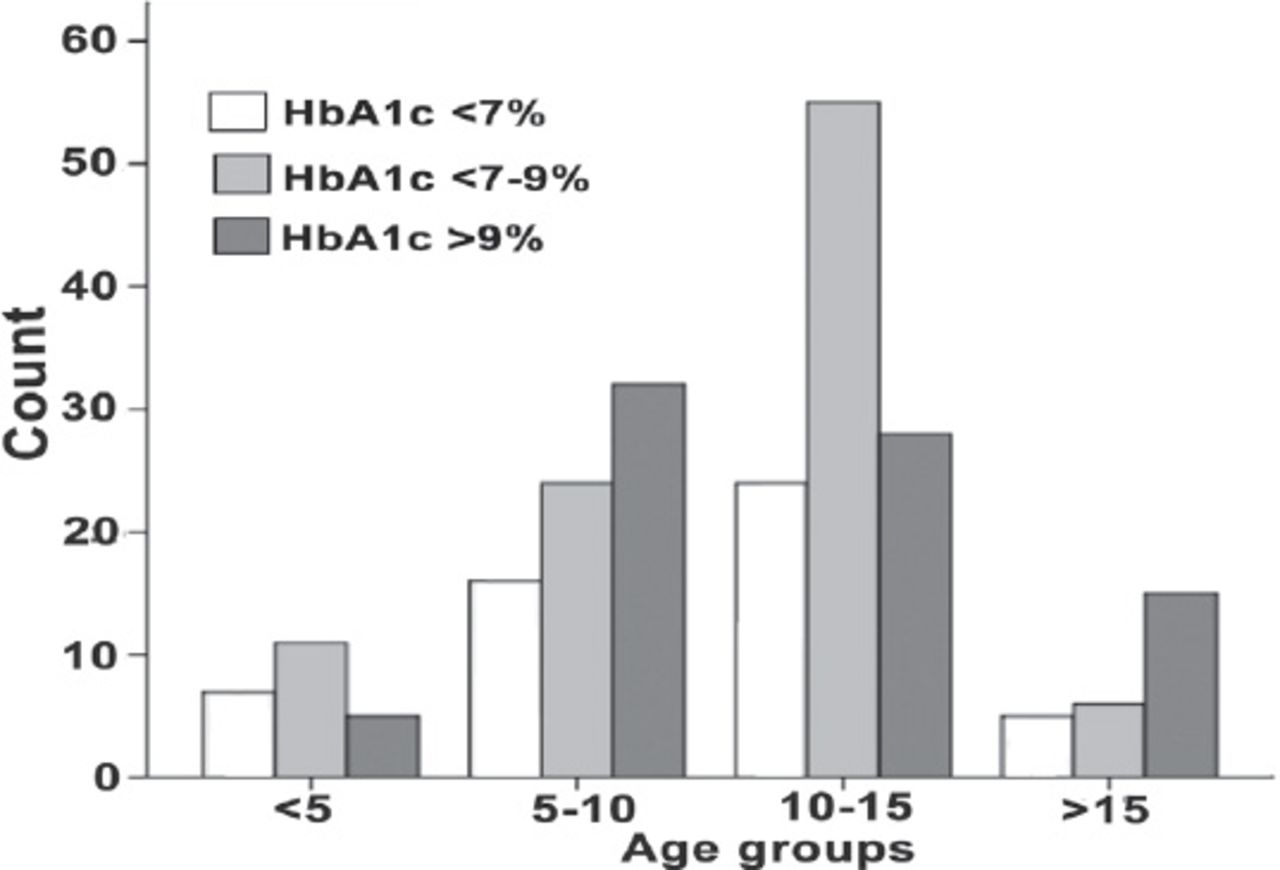
Bar chart representing each age group in relation to the glycemic control level in the studied diabetic pediatric patients.
Demographics of T1DM and acute complications classified by glycemic control in the studied diabetic pediatric patients.
Acute complications
A total of 149 patients (65.3%) had at least one episode of DKA during their disease course. Of these patients, 20.1% were classified as the good metabolic control group, 38.3% belonged to the moderate metabolic control group, and 41.6% were in the poor metabolic control group, with significant differences observed between the glycemic control groups (p=0.01). The mean number of DKA attacks was 1.64 per year. On the other hand, hypoglycemic attacks were reported among 157 patients (68.9%), and no significant differences were observed among the groups (Table 1) Logistic regression analyses were performed to ascertain the effects of DKA and hypoglycemic attacks on the prediction of glycemic control. We found that DKA attacks increases with HbA1c level (odds ratio [OR]=1.208, 95% CI=0.648-2.252), while the hypoglycemic attacks was found to be decreased with an increase in HbA1c level (OR=0.567, 95% CI=0.243-1.323) (Table 2).
Factors assessed to affect or predict good glycemic control in the studied diabetic pediatric patients.
Long-term complications
A cross tabulation was performed using the Chi-square test for comparison, and the t-test was used to compare the means. Retinopathy was identified in 9 patients (3.9%), who were all classified as having moderate-to-poor control (7.8% of the poor control group had retinopathy), with no significant differences observed between the glycemic control groups (p=0.08). Cataract was found in 2 patients only (0.9%), aged 9 and 15 years with moderately good control; error of refraction was detected in 36 patients (14.4%) with no significant correlation to the HbA1c level observed. In this study, 37 patients had microalbuminuria, and 81% of these patients belonged to the moderate-to-poor control group (HbA1c >7%). The mean level of urine albumin was 41.9±2 µg/min. The presence of microalbuminuria was found to be increased with increasing HbA1c levels (OR=1.207; 95% CI: 0.975-1.494), and with longer duration of T1DM (OR=1.071; 95% CI: 0.860-1.332). Dyslipidemia was detected in 206 patients, with a mean LDL level of 173.7±1.3 mg/dL, and TG level of 123.8±4 mg/dL. A total of 93% of the poor control group presented with dyslipidemia, although there was no significant correlation to the HbA1c level (p=0.69). However, there was a relative relation regarding HbA1c level and dyslipidemia that showed (OR=1.154; 95% CI: 0.911-1.463). Vitamin D deficiency was detected in 160 patients, and the mean level of vitamin D was 35.8±19.3 mmol/L; no significant correlation between the vitamin D level and HbA1c level was found (p=0.26).
Associated autoimmune diseases
Autoimmune thyroiditis was identified in 14% of the patients with thyroid dysfunction in 11 patients (4.8%) and subclinical hypothyroidism was detected in 21 patients (9.2%). The mean FT4 was 14.4±3.4 pmol/L, and the mean TSH level was 2.6±3.2 mIU/L; a significant difference between the glycemic control groups was detected in relation to the level of serum TSH, as determined using the t-test (p=0.02). Additionally, 45 patients (19.7%) were diagnosed with CD. The presence of AIT was found to be higher among females, based on the logistic regression results with female gender (OR=1.033; 95% CI: 0.432-2.469), and age (OR=1.041; 95% CI: 0.899-1.204). While CD was found to be increased with age (OR=1.017; 95% CI: 0.935-1.107), and high HbA1C level (OR=1.016; 95% CI: 0.884-1.166).
Discussion
The HbA1c level was found to be higher among the pubertal age group compared to the pre-pubertal age group.10 In this study, we found that most of the school aged group and post-pubertal aged group were in the poor control glycemic control groups. This can be, at least partially, explained by the decreased compliance due to behavioral changes, such as; missed insulin injections; less frequent finger stick home testing for glucose levels; modified dietary habits with more junk and fast foods, especially that delivered at schools; and decreased physical activity due to increased time spent in front of the television, computer, and mobile, in addition to the reduction in care and follow-up provided by the parents.
Severe hypoglycemia and DKA are considered as major life threatening, but preventable complications in children with T1DM. Poor glycemic control has been associated with an increased risk of DKA,11 and in the present study, we confirmed the correlation between glycemic control and frequency of DKA. Hypoglycemia has been reported to increase along with intensive insulin treatment (26.7/100 patient-years).12 In the present study, no significant difference was determined among the different groups of metabolic control. However, we found that hypoglycemic attacks decreased with increased glycemic control level as a predictor of the HbA1c level.
In a previous study, the number of hypoglycemia and DKA cases was reported to be higher in cases of longer disease duration, and in females.13 In our study, we observed a trend in the percentages of DKA and hypoglycemic attacks in the female gender, although these differences were not significant. Regarding the long-term complications of T1DM, diabetic retinopathy and nephropathy are known to play important roles. One study reported that early retinal alterations were associated with an adverse diabetes risk profile, including high HbA1c levels, long duration, and hypertension.14 In the present study, we found no significant association between retinal changes and the HbA1c level. The prevalence of microalbuminuria in children with T1DM is reportedly 10-40%, and approximately 10% of patients have persistent urine albumin elevation.15,16 In the present study, 16.2% of the patients had microalbuminuria. A high risk of microalbuminuria has been reported to be related to insufficient metabolic control, especially in females with long durations of diabetes.17 This study showed a similar result in relation to the HbA1c level and duration of the disease; we found that the presence of microalbuminuria increased with increasing HbA1c levels and with longer duration.
Dyslipidemia is more common in children with diabetes than in healthy children, and is associated with poor glycemic control.18 In the current study, HbA1c level were found similarly associated with dyslipidemia, whereas no significant correlations were observed between HbA1c and LDL and TG levels. Moreover, some studies have suggested an association between T1DM and vitamin D deficiency.19,20 Herein, we found that 70.2% of the patients had vitamin D deficiency, but no relationship between vitamin D status and the HbA1c level was observed. In our society, many other factors apart from T1DM might contribute to vitamin D deficiency.
In a previous study in Saudi Arabia, thyroid dysfunction (TD) was diagnosed in 15.83% of children and adolescents with T1DM.6 In the present study, we found TD due to AIT in 4.8% of the patients, and subclinical hypothyroidism in 9.4% of the patients. It has been reported that subclinical hypothyroidism is associated with more frequent hypoglycemic attacks in children with diabetes.6,21 However, in this study, no significant correlation between the presence of subclinical hypothyroidism and hypoglycemic attacks was observed, whereas we found that the presence of subclinical goiter was significantly associated with hypoglycemic attacks (p=0.009). The prevalence of TD is reportedly higher among females, and with increasing age.22 In this study, similar findings regarding gender were observed.
In Saudi Arabia, the prevalence of CD among children and adolescents with T1DM has been continuously increasing, and it is currently reported to be between 1-16%; this prevalence is considered one of the highest in the world.23,24 In this study, 19.7% of the patients were diagnosed with CD. In a previous study conducted in Saudi Arabia,25 anti-tissue transglutaminase and endomysial antibody were measured in blood samples from children with T1DM, and intestinal biopsy was indicated in some cases. In this previous study,25 all patients with CD with positive anti-tissue transglutaminase had mucosal damage on biopsy. On the other hand we reported 45 patients diagnosed with CD based on positive antibodies and biopsy results. Other previous studies have reported that most patients with diabetes with CD do not have typical gastrointestinal symptoms,24 herein, we similarly found that none of the CD-positive patients had specific gastrointestinal symptoms. Lastly, a previous study reported no significant differences between patients with CD and patients without CD in terms of age, gender, HbA1c level, hypoglycemia, and the presence of any other autoantibodies.26 In the present study, we found that the presence of CD among patients tended to increase with age and high HbA1C level.
In conclusion, the present study revealed a relation between puberty and school age with the glycemic control among patients visiting the diabetes clinic at KAUH in Jeddah. Other autoimmune diseases were found to be coexisting with T1DM in some of the patients, especially in females. Moreover, the presence of vitamin D deficiency in patients with T1DM was found to be high in our population. Based on these results, we recommend intensive diabetes education in terms of behavioral changes during puberty for both patients and parents, and more educational programs to be conducted at schools. Furthermore, we also want to emphasize the importance of routine screening for autoimmune diseases, and annual screenings for long-term complications among children and adolescents with T1DM.
Related Articles
Lasheen AE, Abdelbasit OB, Seidahmed MZ, Hussein KA, Miqdad AM, Al Zahrani MH, et al. Infants of diabetic mothers. A cohort study. Saudi Med J 2014; 35: 572-577.
Al-Hayek AA, Robert AA, Alzaid AA, Nusair HM, Zbaidi NS, Al-Eithan MH, et al. Association between diabetes self-care, medication adherence, anxiety, depression, and glycemic control in type 2 diabetes. Saudi Med J 2012; 33: 681-683.
Bin-Abbas BS, Jabari MA, Issa SD, Al-Fares AH, Al-Muhsen S. Vitamin D levels in Saudi children with type 1 diabetes. Saudi Med J 2011; 32: 589-592.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 14, 2014.
- Accepted December 1, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Autoimmune diseases and their prevalence in Saudi Arabian patients with type 1 diabetes mellitus
- Celiac disease in type 1 diabetes mellitus in the Kingdom of Saudi Arabia: Characterization and meta-analysis
- Celiac disease among at-risk individuals in Saudi Arabia
- Pattern of thyroid, celiac, and anti-cyclic citrullinated peptide autoantibodies coexistence with type 1 diabetes mellitus in patients from Southwestern Saudi Arabia