


ABSTRACT
Objectives: To investigate the psychological stress and its association with bronchial asthma in Saudi Arabia, focusing on the mechanisms by which stress affects asthma.
Methods: This cross-sectional study included 733 adults with asthma aged ≥18 years and was carried out between October 2022 and May 2023 in Saudi Arabia. Data were obtained using an online questionnaire assessing asthma severity and stress levels.
Results: Cronbach’s alpha indicated that the reliability of the stress scale was 0.728 and the reliability of the asthma control tool was 0.819. Of the participants, 52% were women and 48% were men, with 48.7% aged 18-26 years. Asthma severity was classified as low (20.3%) or high (54.6%) and 85.4% of the respondents reported elevated stress levels. A statistically significant correlation was noted between asthma control and sterss (r= -0.22, p<0.05), indicating that higher stress levels hinder the management of asthma.
Conclusion: There is a strong association between psychological stress and exacerbation of bronchial asthma. Stress impacts immune responses, thereby contributing to the pathogenesis of asthma. Therefore, effective stress management is essential in improving the control of asthma and the alleviation of its symptoms.
Stress, the sensation of feeling overwhelmed or unable to cope with mental or emotional pressure, significantly affects one’s mood, well-being, behavior, and health. As stress arises from both intrinsic and extrinsic stimuli that trigger biological responses, understanding and recognizing the types of stress can be beneficial for their effective management.1
Stress can be categorized into acute, episodic, and chronic stress. Acute stress is a common reaction to challenging situations and occurs in all individuals. Episodic stress is characterized by frequent episodes of acute stress that arise after prolonged periods of tension and anxiety due to anticipation.1 Chronic stress involves high stress levels sustained over an extended period of time, which can negatively affect physical and psychological health, and may manifest as respiratory or cardiovascular conditions with symptoms such as rapid breathing, shortness of breath (SOB), and an unstable heart rate.2,3 It can also contribute to anxiety, depression, stomach aches, headaches, and sleep problems. Therefore, understanding and recognizing the causes of stress are essential for the effective prevention and intervention of the condition.1
Typical causes of stress include natural or human-made disasters, long-term illness, potentially fatal accidents, robbery, familial stressors, caring for a loved one with a chronic illness, poverty or homelessness, hazardous work environments, lack of work-life balance, or dissatisfaction with one’s job. Owing to the diversity among individuals, there are unlimited factors that contribute to stress. The impacts of stress on the body can be severe if the cause is not properly controlled. As each individual is exposed to different stressors, symptoms may vary from person to person. Symptoms of stress include chronic pain, sleep apnea, other sleep disturbances, low sex drive, digestive issues, difficulty concentrating, and impaired decision-making.1 Stress is a known trigger and exacerbating factor for various pathological conditions, including asthma, depression, anxiety, cardiovascular disease, acquired immunodeficiency syndrome, and certain types of cancer.3,4 Additionally, acute stress can enhance resistance to infection. Recent evidence has suggested a causal association between persistent psychosocial stress, asthma, and asthma morbidity.5
Asthma, a primary inflammatory condition of the airways, is characterized by increased hyper-reactivity and obstruction of airflow in the conducting airways and is caused by partially or completely reversible inflammation that resolves either spontaneously or with treatment. Classic symptoms of asthma include SOB, coughing, wheezing and chest tightness.6 Airway inflammation has highlighted the possibility that stress-induced modifications in the immune response may contribute to the progression and exacerbation of asthma.7 The mechanism of psychological stress-induced exacerbation of bronchial asthma is mediated through neuroendocrine activity, which likely involves a series of pathological events from the brain to the lungs.8 Consequently, emotional perceptions, neuroendocrine activities, and immune networks are pathological systems which are responsible for dysregulation and exhaustion are influenced by excessive stress intensity, amount, duration, or individual personality traits.9 Furthermore, psychological, occupational, and familial stressors are risk factors for adverse health outcomes, including poor asthma management.10,11 Behaviors such as smoking, which are often used as coping mechanisms, can worsen the symptoms of asthma and complicate their management. Furthermore, the severity of asthma symptoms is associated with an increase in perceived stress.10
Several studies have suggested a relationship between stress and asthma. According to recent studies involving a variety of modalities, psychological factors may affect asthma symptoms in both adults and children. Psychological stress has been shown to exacerbate asthma symptoms, as highlighted in a literature review that described the significance of psychological interventions for the management of asthma.12 Asthma morbidity and its symptoms may be influenced by stress at personal, familial, or social levels. Furthermore, environmental exposure combined with stress may exacerbate negative outcomes and morbidity of asthma. A recent study showed that patients simultaneously experiencing stress and air pollution exposure have a higher risk of inflammatory reactions and respiratory dysfunction than those exposed to only one or the other. Additionally, chronic stress might intensify airway inflammation triggered by environmental and infectious pollutants, resulting in the worsening of asthma symptoms.13,14 Chronic stress has been associated with decreased responsiveness to short-acting bronchodilators and the subsequent worsening of asthma symptoms.15,16 Contributing factors such as community crimes, violence, psychosocial stressors (acute or chronic), anxiety disorders, arguments, and bullying due to asthma also play a role in asthma morbidity.13,14,17 Although stress and asthma are known to be related, the mechanism underlying this association is not fully understood.14
According to the aforementioned literature review, despite the vast number of studies on asthma, it is evident that studies examining the psychological aspects of asthma are both few in number and limited in scope. Although previously studied, there is a lack of literature explaining the relationship underlying psychological stress and its association with asthma. Furthermore, the psychological aspects of asthma in the Arab region need to be investigated, as research is scarce in this area, with an average of only one study per year over the past 25 years.12,18
Given the limited research available on the association between stress levels and bronchial asthma in Saudi Arabia, we aimed to provide a qualitative addition to the existing studies and enrich our findings in this field by analyzing psychological stress and its association with bronchial asthma in Saudi Arabia. By examining how stress influences asthma, this study sought to investigate the psychological stress effect on the pathophysiological mechanisms underlying asthma. Specifically, we explored how stress-related factors contribute to asthma symptoms and exacerbations, shedding light on the physiological changes that stress may induce in the respiratory system. This information is crucial for addressing the limited understanding of stress-related asthma mechanisms within the Saudi Arabian population, while offering valuable insights for improving the management of asthma as well as patient well-being.
Methods
This study utilized a cross-sectional design carried out in Saudi Arabia between October 2022 and May 2023, with the study divided into 5 geographical regions: central, western, eastern, southern, and northern. This study included individuals aged ≥18 years with asthma residing in Saudi Arabia. We utilized 2 instruments to gather data from the patients: the asthma control test (ACT) and perceived stress scale (PSS) for patients aged ≥18 years. These 2 instruments are both reliable and valid, and have been expertly translated from English to Arabic.
The inclusion criteria were as follows: a diagnosis of asthma and age ≥18 years, while there were no exclusion criteria.
The study sample size for this analytical cross-sectional study was initially calculated to be 385 participants. However, to account for a 30% nonresponse rate, the final study sample size was adjusted to 501 participants. Convenience nonprobability sampling is a suitable sampling technique that is consistent with the study’s aims and objectives.
An institutional review board approval was obtained from King Abdullah International Medical Research Center, Jeddah, Saudi Arabia (approval no. SP22J/101/08). and written informed consent were obtained from all of the participants
The data were collected from an online questionnaire comprised of 3 sections: I) section 1, demographic characteristics of the participants (age, gender, and geographical area); II) section 2, PSS to determine the stress levels of the participants, comprised of 10 questions in English and Arabic, each with 5 responses, ranging 1-5, with higher scores representing higher stress; and III) section 3, severity of asthma determined using the ACT, which consisted of 5 questions written in English and Arabic. This test has been validated and approved worldwide.
To minimize potential bias, this study included participants from 5 geographic regions across Saudi Arabia to enhance representativeness. Furthermore, the previously validated PSS and ACT tools were translated into Arabic for cultural relevance. No exclusion criteria were applied to ensure inclusivity. Despite the use of convenience sampling, efforts were carried out to engage a diverse participant pool to reduce selection bias. This study targeted Saudi Arabian adults with asthma, with a sample size calculated using a simple random sampling equation based on the targeted population with a 95% confidence interval (CI), 5% margin of error, and an anticipated population proportion of 50%.
Statistical analysis
Quantitative variables such as stress levels and asthma severity scores were assigned numerical values based on the participants’ responses to the PSS and ACT. These scales provided continuous data that allowed for the statistical analysis of the associations between stress and asthma control. Stress scores were grouped into categories (low, moderate, and high) to examine the differences in asthma outcomes among varying stress levels. This grouping approach simplified the interpretation and revealed potential thresholds at which stress significantly affected asthma severity. Demographic variables such as age were also categorized into ranges to assess how various age groups experienced stress and asthma differently. Data preparation and revision were carried out using Excel prior to data analysis, which was carried out using the Statistical Package for the Social Sciences, version 25.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics used in this study included frequencies and percentages of categorical variables, while means and standard deviations (SDs) were calculated for scale variables. The differences and correlations between study variables and scales were examined using t-tests, analysis of variance, and correlation analyses. Statistical significance for all analyses was p<0.05.
Results
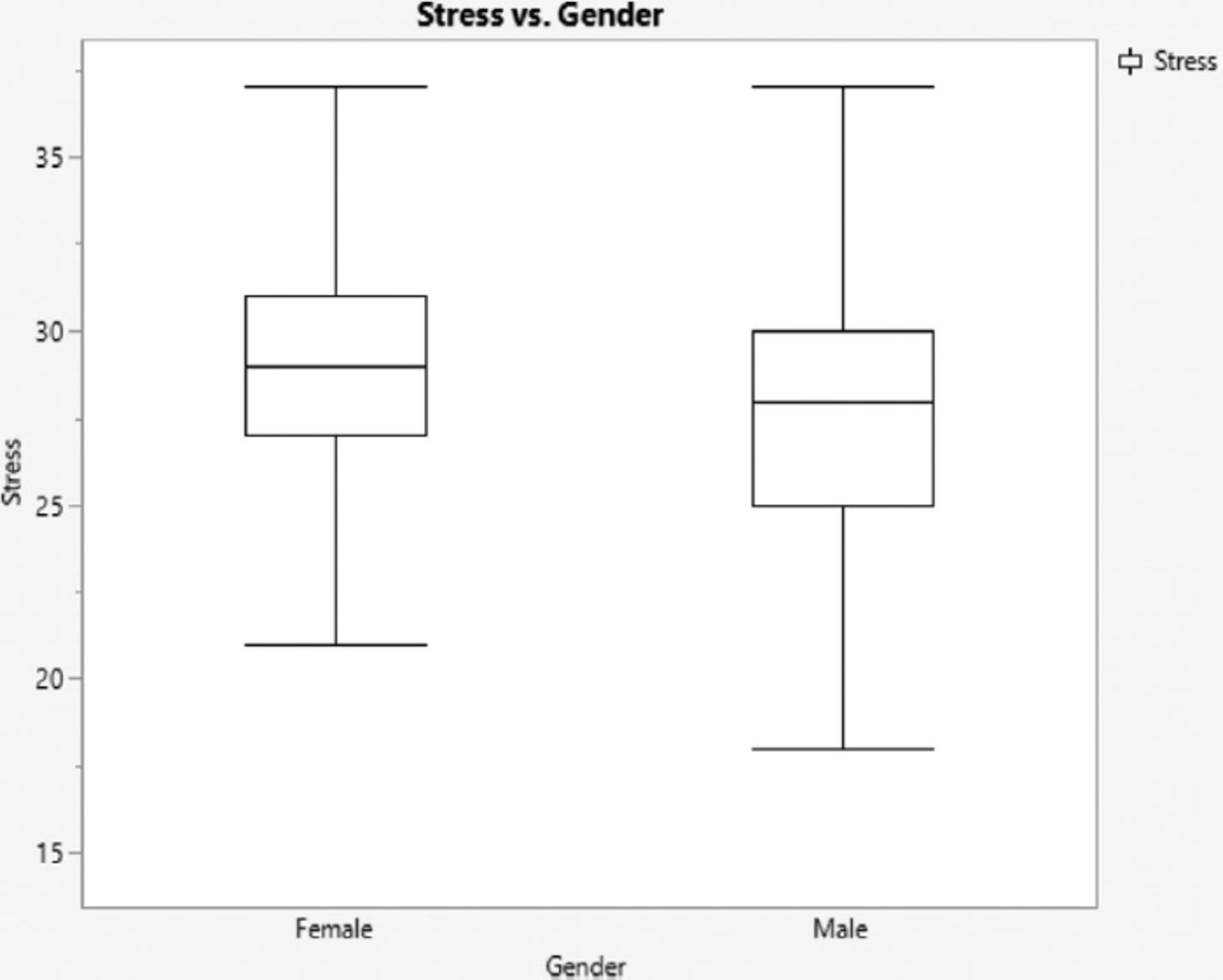
The coefficient of Cronbach’s alpha test was 0.728 for the stress scale and 0.819 for the asthma scale, indicating high internal consistency for both. There were a total of 733 participants, 352 (48%) of whom were men while the remaining 381 (52%) were women. The age distribution showed 357 (48.7%) participants aged 18-25 years, 198 (27.0%) aged 26-39 years, and 178 (24.3%) aged ≥40 years. The participants were geographically distributed as follows: western (n=340; 46.4%), southern (n=181; 24.7%), eastern (n=126; 17.2%), central (n=75; 10.2%), and northern (n=11; 1.5%). Stress levels were classified as follows: low (n=14; 1.9%), moderate (n=93; 12.7%), and high (n=626; 85.4%), as summarized in Table 1. Asthma control levels were categorized as follows: uncontrolled (n=149; 20.3%), partially controlled (n=184; 25.1%), and completely controlled (n=400; 54.6%). The Pearson correlation coefficient was -0.22 (p<0.05), and a significant negative correlation was identified between the 2 variables, indicating that higher stress levels were associated with poorer asthma control, while contrarily, lower stress levels were correlated with better asthma control, as shown in Table 2. The results showed a difference in stress levels between men and women, with women having a higher level of stress than men (Figure 1), while men had less control over asthma than women (Figure 2). The mean of stress levels were 30.1250±5.8379 for men and 32.1969±5.4449 for women (p<0.001), indicating a statistically significant difference in stress levels between men and women. When assessing asthma control levels, the mean were 20.0881±4.42483 for males and 18.853±4.65317 for females, as shown in Table 3.
- Reliability, frequency, and demographic characteristics.
- Frequency of stress and asthma categories and correlations.
- Mean score, standard deviation, frequency, and p-value of stress and asthma association regarding age and gender.

- Plot box illustrates the difference between males and females in responding to stress using the perceived stress scale.

- The plot box illustrates the variation in asthma control levels between males and females, as measured by the asthma control scale.
Among the 733 participants, 264 (84.3%) with high levels of stress had activities of daily living (ADL) that were significantly associated with poor asthma control level (p=0.002), whereas only 11 (3.5%) participants with low levels of stress showed the same association. According to the results, 191 (79.3%) participants with high levels of stress demonstrated a significant relationship between poor asthma control and dyspnea (p<0.001), compared to 12 (5.0%) participants with low levels of stress, who exhibited a similar relationship (p<0.001), based on the second question on the ACT. We also found that the number of awakenings at night and low quality of sleep (insomnia) were significantly associated with poor asthma control among 287 (83.4%) participants with high levels of stress (p<0.015), while 14 (4.1%) participants with low levels of stress and poor asthma control showed a significant association (p<0.015). The majority of the participants (n=355; 85.3%), with high stress levels exhibited an insignificant association between poor asthma control and the use of asthma medications (p=0.097). Similar findings were observed among 13 (3.1%) participants with poor asthma control and low stress levels (Table 4).
- The frequency and percentages for the asthma scale categories.
Discussion
We investigated psychological stress and its association with bronchial asthma in Saudi Arabia. Our analyses revealed that stress and asthma were significantly negatively correlated, suggesting that elevated stress levels were linked to inadequate asthma control. However, most of the participants evaluated their asthma control levels to be within an acceptable range.
This study explored the relationship between gender and asthma, which had no significant correlation. Interestingly, male participants had lower asthma control than female participants, whereas female participants had higher stress levels than their male counterparts. These findings are in contrast to those described in relevant literature that has examined the association between gender and asthma.19 Previous studies have shown that asthma affects adult women more frequently and more severely than other diseases. Gender differences in the incidence, prevalence, and severity of asthma are influenced by factors such as genetic changes, sex hormones, environmental factors, and responses to asthma treatments. The etiology of asthma in women has been correlated with changes in sex hormone levels during adolescence, the menstrual cycle, and pregnancy. Additionally, lower physical activity levels in women compared to men have been linked to a higher likelihood of experiencing asthma symptoms.20,21
We found that dyspnea, a primary symptom of asthma, was significantly associated with asthma control. This finding aligns with a previous study indicating that diminished perception of dyspnea is associated with a higher risk of asthma attacks and exacerbations. Advanced stages of the asthma, as well as eosinophilic airway inflammation, have been identified as potential causes of poor perception of dyspnea.22
We also observed a significant relationship between insomnia and asthma. Approximately 40% of the participants in this study experienced insomnia associated with poor asthma control, a relationship suggested by previous studies. Additionally, insomnia is accompanied by functional limitations, particularly in older adults with asthma.23 Another study suggested that uncontrolled asthma is highly associated with an increased risk of insomnia, whereas controlled asthma does not pose the same risk. Furthermore, asthma-related comorbidities, especially when combined with uncontrolled asthma, have been shown to exacerbate insomnia symptoms.24
This study highlighted a significant association between asthma and ADL, which are essential and routine tasks carried out independently by healthy individuals. Our findings suggested that ADL performance decreased in participants with poorly controlled asthma. Approximately 58% of the study participants reported uncontrolled asthma associated with reduced ADL. Several prior studies have shown that uncontrolled asthma has a greater impact on ADL than controlled asthma. Moreover, participants have reported that their general quality of life, sleep, social interactions, sports, and regular physical activity were adversely affected by asthma.25,26
Study’s limitations
The small number of participants recruited from the northern region is low compared to the rest of the regions (western [n=253], eastern [n=183], southern [n=157], central [n=129], and northern [n=11]). Additionally, there was insufficient representation of participants aged ≥40 years, who are more vulnerable to the adverse effects of poor asthma control.
In conclusion, this study revealed a strong association between psychological stress and exacerbation of bronchial asthma. Factors influencing this association include dyspnea, insomnia, and ADL. As stress levels increase in individuals with asthma, as do dyspnea and insomnia, which negatively impact asthma control, leading to poor outcomes as measured by the ACT. Over time, reduced ADL further exacerbates the psychological, social, and physical challenges faced by patients with asthma. To address these issues, healthcare facilities and institutions should educate the public on effective stress management in conjunction with asthma control. Routine educational sessions in asthma clinics should be integrated to address these aspects and provide patients and their families with practical strategies to manage stress and enhance their understanding of asthma. These sessions can empower individuals to proactively manage their health. Future studies should recruit a larger, geographically diverse sample and focus on including more participants aged ≥40 years to provide a detailed analysis of individuals with asthma as well as high levels of stress.
Acknowledgment
The authors gratefully acknowledge Editage for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 19, 2025.
- Accepted April 14, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.