


Abstract
Objectives: We determined the surgical and oncological outcomes of laparoscopic nephroureterectomy (LNU) in comparison to open nephroureterectomy (ONU) and factors predicting bladder recurrence after nephroureterectomy.
Methods: We retrospectively reviewed and compared the data of patients who underwent ONU or LNU for non-metastatic, upper-tract urothelial carcinoma from 2000 to 2016. The primary endpoint was to determine bladder cancer recurrence-free survival (BCRFS), cancer-specific survival (CSS), and overall survival (OS). The data were analysed using Student’s t-test, Chi-square test, and Kaplan-Meier curve.
Results: Total of 50 patients, of which 24 had LNU and 26 had ONU, met the inclusion criteria. Median durations of follow-up were 4.2 and 6.5 years (p=0.1070) in LNU and ONU, respectively. Operative time, blood loss and hospital stay were significantly lower in the LNU group than in the ONU group (p=0.0001, p=0.0001, p=0.0018). Cancer-specific survival rate in the LNU was 75% and ONU was 73.3% (p=0.1902), whereas BCRFS and CSS were not significantly different in both groups (log-rank test; BCRFS: p=0.809 and CSS: p=0.802). Patients who underwent ureteroscopy with biopsy (p=0.001), had multifocality (p=0.001) and previous history of (H/O) bladder cancer (p=0.020) were at significant risk for developing bladder cancer recurrence after nephroureterectomy.
Conclusion: Laparoscopic nephroureterectomy can benefit patients because of its minimal invasiveness, and oncologic outcomes are comparable to ONU. Preoperative ureteroscopy with biopsy, multifocality and previous H/O bladder cancer might be risk factors for bladder cancer recurrence.
Upper-tract urothelial carcinoma (UTUC) is an uncommon disease. It accounts for approximately 5% of urothelial carcinomas, and it comprises of 5-15% of malignancies arising from the kidneys while ureteral urothelial carcinoma represents only 1%.1,2 Upper-tract urothelial carcinoma has a higher propensity for recurrence and progression than bladder cancer does. Among patients with primary UTUC, 25-75% will develop metachronous urothelial carcinoma (UC) in the bladder, usually within 2 years of diagnosis of initial UTUC. These findings stress the need for close surveillance of the bladder in patients with UTUC.3 Almost 50% of UTUC cases are invasive, and 19% of patients present with metastatic disease.4 The gold standard treatment for localized UTUC is radical nephro ureterectomy (RNU) with excision of the bladder cuff5 because of the high propensity for multifocality, recurrence, and progression. This can be carried out by either open radical nephroureterectomy (ONU) or laparoscopic nephroureterectomy (LNU). Although ONU is the gold standard for UTUC, it is associated with significant morbidity; on the other hand, LNU has been found to be more effective, with fewer intra- and perioperative adverse outcomes as a minimally invasive treatment.6 However, in comparison to ONU, oncological outcomes for LNU, such as cancer-specific survival (CSS), metastasis-free survival (MFS) and bladder cancer recurrence-free survival (BCRFS), remain controversial topics.7,8 Some researchers argue that surgical manipulation during dissection and high-pressure pneumoperitoneal insufflation during LNU are risk factors for bladder, local and port-site metastasis.9 Since UTUC has a high propensity for recurrence, progression and poor prognosis, it is even more crucial to search for predictive factors. Several studies based on perioperative clinicopathological features have been presented, with an aim to identify risk factors for metachronous bladder cancer recurrence.8,10 Previous history of bladder cancer, concomitant carcinoma in situ (CIS), multifocality and preoperative ureteroscopy (URS) with or without biopsy have been validated as risk factors for metachronous bladder cancer with different surgical approaches. Recently, a few studies have proposed that diagnostic URS with biopsy for upper urinary tract lesion is an independent risk factor for metachronous bladder cancer recurrence.11
Our main objective in this study is 2-fold: 1) to compare the perioperative and oncological outcome of LNU versus ONU; 2) to determine predictive factors for metachronous bladder cancer recurrence after nephroureterectomy.
Methods
Our research proposal was approved by the Office of Research Assistant (ORA) of King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia (RAC # 5121091).
We retrospectively collected the data of patients at our institution, who underwent either ONU or LNU for UTUC from 2000 to 2016. We excluded patients on the basis of following criteria: histology other than UC, positive lymph nodes (LN), and metastasis at diagnosis.
Preoperative evaluation included staging computed tomography (CT) of the chest, abdomen and pelvis, with and without contrast, along with blood work and urine cytology. Bone scan was performed in symptomatic cases suggestive of metastasis. Ureteroscopy and biopsy were performed only in equivocal cases or at surgeon’s preference to confirm pathology prior to radical surgery. Cystoscopy was performed in all patients to determine the presence of synchronous tumor in the bladder before NU.
Perioperative clinicopathological data such as age, gender, intraoperative blood loss, operative time, hospital stay, type of bladder cuff excision, location of tumor, history of prior bladder cancer, and histopathological data were also documented from patient files. Oncological outcome in terms of BCRFS, overall survival (OS), and CSS were also reviewed. Time from diagnostic URS to RNU and to bladder recurrence was also noted.
Surgical techniques
Surgical method (laparoscopic versus open) mainly depended on patient and surgeon preference. Radical nephroureterectomy was performed according to department standard protocol. Regardless of surgical approach, the basic principle of RNU was adopted with en bloc removal of kidney, Gerota fascia, entire ureter and bladder cuff. In few cases, bladder cuff was not taken due to uncertainty of UC. Regional LN dissection was generally performed only in cases where LN involvement was suspected or if they were palpable intraoperatively. Four-trocar technique was used to perform transperitoneally LNU. Open nephroureterectomy was performed by standard technique through flank incision and bladder cuff was excised extravesically with a lower-quadrant Gibson incision.
Pathological evaluation
All surgical specimens were processed according to standard pathological protocol and reviewed by our expert genitourinary histopathologist. American Joint Committee on Cancer classification 2010 and World Health Organizations 2004 were used to determine tumor stage and grade respectively. Therefore, the patients who underwent surgery before these guidelines were reassessed for tumor stage and grade. Tumor multifocality was defined as synchronous presence of 2 or more histologically confirmed in any location from renal pelvis to ureter.
Follow-up
Patients were regularly followed up with flexible cystoscopy every 3 months for the first year, every 6 months for the next 2 years and then annually thereafter. Follow up included history, physical examination, urine analysis, urine cytology, cystoscopy, chest radiograph and abdominopelvic CT. Bladder cancer recurrence-free survival was defined as time period from surgery to the occurrence of UC in bladder. Cancer-specific survival was defined as the interval from RNU to the death directly from UTUC. Overall survival was evaluated from date of RNU to last date of follow up or date of death from any cause. Date of death was obtained from either hospital record or by taking first relative on phone if occurred in other hospital.
Statistical analysis
Statistical analyses were performed using SAS software package, version 9.4 (Statistical Analysis System, SAS Institute Inc., Cary, NC, USA). Clinical and pathological characteristic of 2 groups (ONU versus LNU) were compared by using student’s t-test for continuous variable and the Chi-squared test for categorical variables. Comparisons for both continuous and categorical data was carried out using the nonparametric test (Mann-Whitney test) in which normality test (Shapiro-Wilk) was significant <0.05. For each of these tests, the significance level was set at <0.05. Fisher exact test was used in variables in which we received warning sign where number values were less than 5.
Univariate logistic regression analysis was used to determine the association between baseline patient characteristics such as age, body mass index (BMI) and surgical approach. Multivariable regression analysis was used to investigate the association between surgical approach and variables which were significant in univariate regression model.
Recurrence-free probabilities were determined using Kaplan-Meier methods, and patients without disease recurrence were restricted at their date of last follow-up. Survival time was calculated from the date of radical nephroureterectomy (RNU) to last follow. A multivariable Cox proportional hazards regression model was used to determine the association between surgical approach and bladder cancer recurrence, controlling for the effects of age, pathologic stage and grade, nodal status, carcinoma in situ, multifocality, preoperative URS with biopsy and prior history of bladder cancer.
Results
From January 2000 to December 2016, a total of 64 patients underwent radical nephrectomies, in which 50 patients met our inclusion criteria. Of these 50 patients, 26 patients had ONU and 24 underwent LNU for non-metastatic UTUC. Median follow-up was 6.5 years in ONU group and 4.2 years in LNU group (p=0.107).
Table 1 shows the baseline characteristics and comparative analysis of clininicopathological factors according to surgical mode. More than half (60%) of the patients had renal pelvic tumor. Bladder cuff was not taken in 5 (10%) patients due to uncertain pathology. Three (60%) patients developed recurrence in ureteral stump that underwent open distal ureterectomy and bladder cuff removal later on. Similarly, more than half (58%) of the patients had preoperative URS and biopsy for diagnostic purposes. Eighteen (62.1%) of these patients developed bladder recurrences after a median period of 8.2 (IQR, 5.89-14.69) months after preoperative ureteroscopy and biopsy. Significant association was found in patients who had preoperative URS and biopsy and developed bladder cancer recurrence (p=0.003). There were positive lymph nodes in 5 (19.23%) patients in the ONU group and in one (4.16%) patient in the LNU group. Patients who had positive lymph nodes (6 patients) at surgery received adjuvant systemic chemotherapy with gemcitabine and cisplatin.
Baseline clinical and pathological characteristics and comparative analysis results according to mode of surgery.
Perioperative outcome
There was a significant difference in the intra- and perioperative results, which were in favor of LNU. The operative time calculated as the time of making incision to closure of wound in both groups was significantly lower in the LNU group than in the ONU group (p=0.0001 (Table 2).
Intra- and perioperative comparative analysis using nonparametric (Mann-Whitney) test.
Survival analysis
During median follow up of 4.47 years, bladder recurrence occurred in 20 (40%) patients, including 10 (38.5%) in ONU and 10 (41.7%) patients in LNU group (p=0.817). Three patients (2 in ONU and one LNU) in which ureteral stump recurrence occurred due to non-excision of bladder cuff underwent distal ureterectomy and bladder cuff excision. There were no cases of port-site metastasis in LNU group. Local recurrence in retroperitoneal space occurred in 4 (15.4%) patients in ONU group versus 2 (8.3%) patients in LNU group (p=0.668). In all, the estimated CSS was 74% in ONU and 76% in LNU group (p=0.190). At last follow up, 13 (26%) patients died of metastatic disease, including 7 (26.9%) in ONU and 6 (25%) patients in LNU group (p=0.876) as shown in Figures 1A-1C.

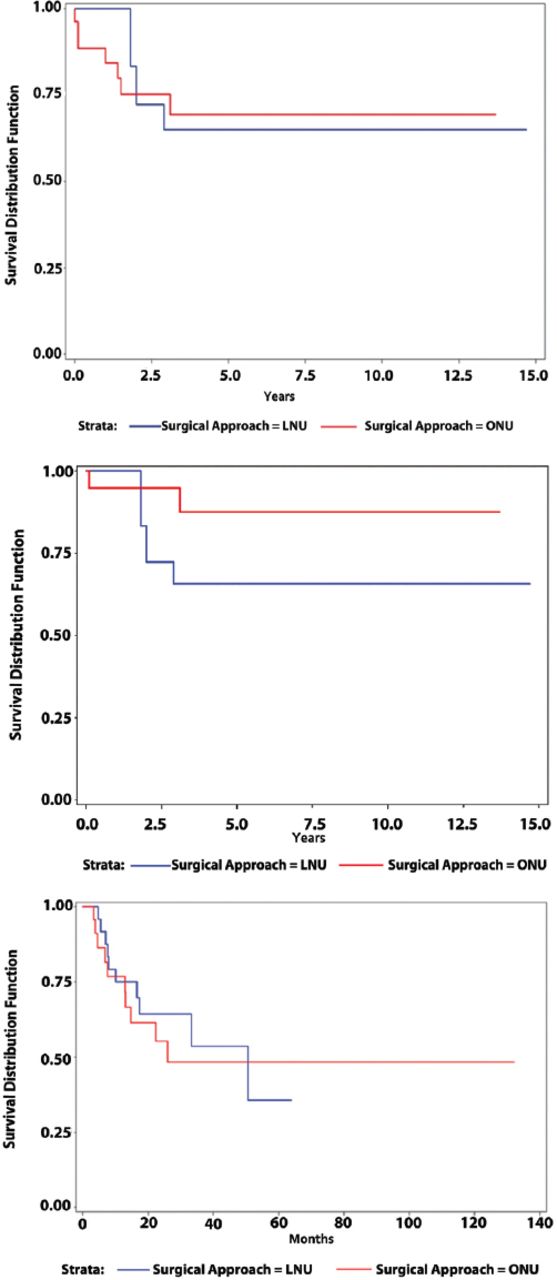
Kaplan-Meier curve of A) overall survival between ONU and LNU (Log rank p=0.802), B) cancer specific survival between ONU and LNU (Log rank p=0.190), and C) bladder cancer recurrence-free survival between the ONU and LNU groups (Log rank p=0.809). ONU: open nephroureterectomy, LNU: laparoscopic nephroureterectomy
Clinical outcome and surgical approach by univariate analysis
Table 3 shows the results of univariable analysis that examined predictors of clinical outcomes in all patients. Surgical approach was not associated with CSS (HR:1.13; 95% CI: 0.55-2.29), p=0.72), OS (HR: 1.14; 95% CI: 0.38-3.42, p=0.80), and BCRFS (HR: 1.11; 95% CI: 0.46-2.68, p=0.80). Pre-operative URS with biopsy (HR: 8.97; 95% CI: 2.07-38.85, p=0.003), multifocality of tumor (HR: 9.45; 95% CI: 3.10-28.77, p=0.001), and prior history of bladder cancer (HR: 0.22; 95% CI: 0.05-0.95, p=0.04) were significantly associated with bladder recurrence. Higher pathological stage was associated with poor CSS (HR: 2.94; 95% CI: 0.98-8.85, p=0.05) and OS (HR: 67.76; 95% CI: 8.26-555.58, p=0.001]. Similarly, the sessile nature of a tumor’s architecture was associated with poor CSS (HR: 1.01; 95% CI: 0.45-2.27, p=0.001) and OS (HR: 2.90; 95% CI: 0.97-8.67, p=0.05)
Univariate cox proportional hazard analysis of predicting CSS, OS and BCRFS outcome.
Clinical outcome and multivariate analysis
Table 4 presents the multivariate analysis of predictors of clinical outcome of factors that were significant in univariate analysis. Higher pathological and nodal stage was significantly associated with poor CSS (HR: 4.933; 95% CI: 1.199-0.302; p=0.027 and OS, (HR: 81.73; 95% CI: 3.26-20.33; p=0.007) whereas multifocality and history of (H/O) of bladder cancer was associated with bladder cancer recurrence. Preoperative URS with biopsy was not significantly associated with bladder recurrence on multivariate analysis.
Multivariate cox proportional hazard models analysis of predicting CSS, OS and BCRFS outcome
Figures 1A-1C show the Kaplan-Meier estimates for OS (log-ranked p=0.802), CSS (log-ranked p=0.190), and BRFS (log-ranked p=0.809) stratified by surgical approach in the overall cohort of patients; the result was not significant.
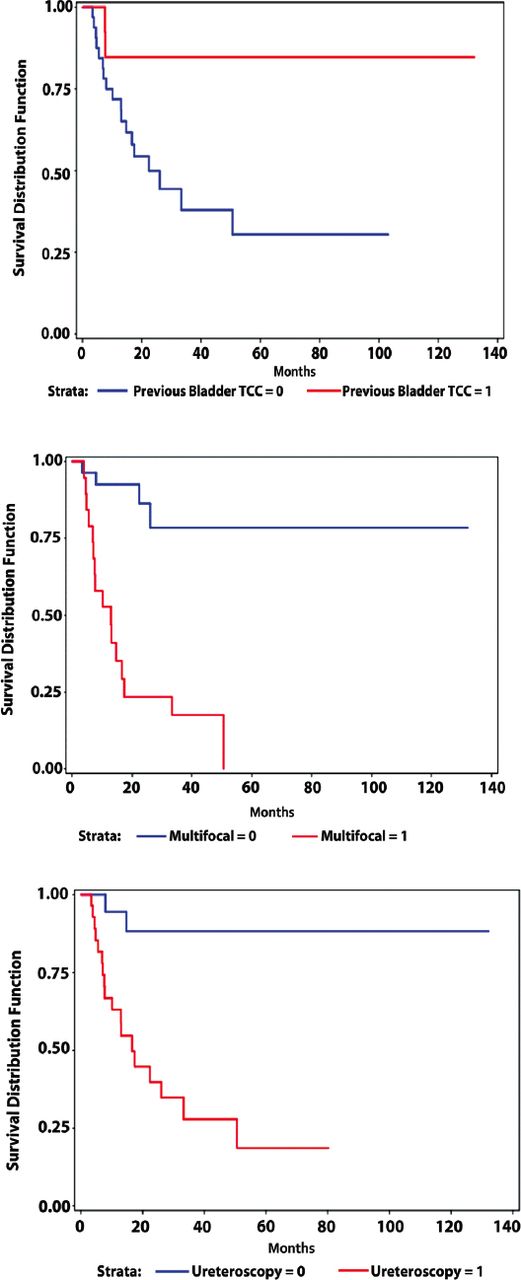
Similarly, Kaplan-Meier estimates for bladder cancer recurrence was significantly associated with H/O bladder cancer (log-rank p=0.027), multifocality of tumor (log-rank p=0.001) and preoperative URS with biopsy (log-rank p=0.004), as shown in Figures 2A-2C.
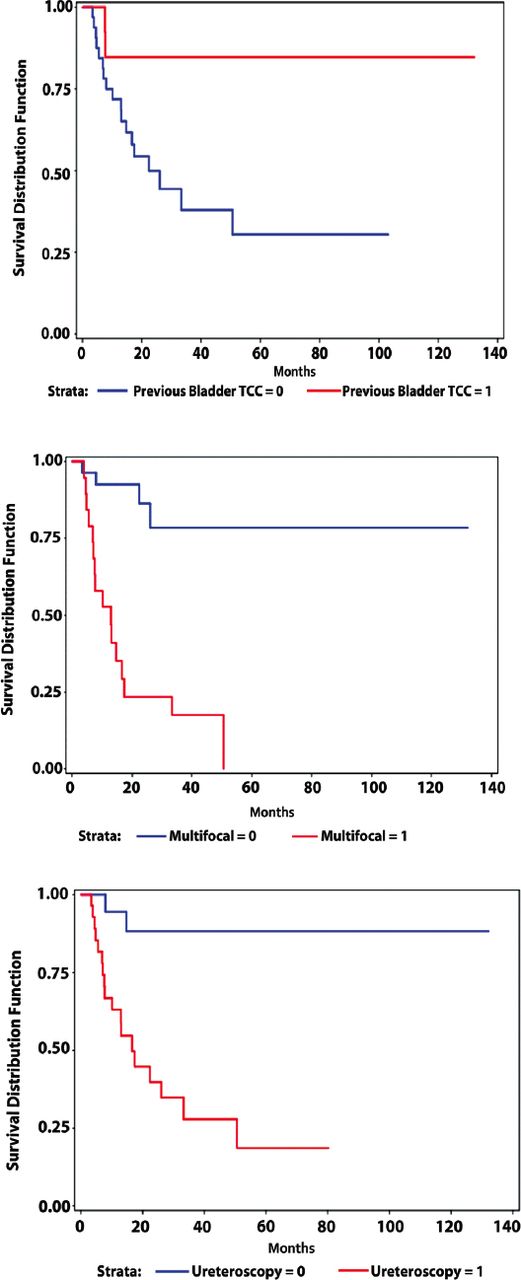
Kaplan-Meier curve of A) bladder cancer recurrence-free survival by history of bladder cancer (Log rank p=0.0.027), B) bladder recurrence-free survival by multifocality (Log rank p=0.0001), C) bladder recurrence-free survival by pre-operative preoperative ureteroscopy with biopsy (Log rank p=0.003)
Discussion
Laparoscopic nephroureterectomy is a feasible alternative procedure to ONU for UTUC treatment in many centers with available facilities and experienced laparoscopists,12 despite concerns about its safety. Several patient series have published the technical feasibility and lower postoperative morbidity of LNU with less blood loss, short hospital stay, and even short operative time compared with ONU, regardless of the technique used in LNU for lower ureter management.13 In our study, we observed a significant decrease in blood loss, shorter hospital stays, and decrease in operative time in patients with LNU as compared to those in the ONU group. Similar perioperative and minimally invasive benefits of LNU were reported by Mullen et al14 in their study.
In terms of oncological outcome, controversy still exists among researchers regarding the feasibility of LNU for the management of UTUC. We found that surgical approach was not independently associated with CSS and recurrence-free survival. Various studies have been published that support our series. Liu et al15 found in 265-patient series that oncological outcome of LNU is comparable to that of ONU, and LNU was more advantageous in terms of lower morbidity and minimal invasiveness. Favaretto et al16 reported analyses of 324 patients with UTTCC who had radical NU at the Memorial Sloan-Kettering Cancer Center and found no association between surgical approach and oncological outcome. Similarly, 2 large multi-institutional studies of patients who underwent LNU and ONU for UTUC failed to show any difference in oncological outcome with surgical approach.17,18 However, in contrast, some patient series found a worse outcome with LNU than with ONU. Peyronnet et al19 found that outcomes of patients treated with LNU had significantly poorer outcomes in high-grade and stage tumors than with ONU, whereas there was no difference in oncological outcome in low-stage and low-grade disease. Recently, Kim et al7 published a patient series that reported a worse oncological outcome with LNU than with ONU, but there was no difference in intravesical recurrence between the 2 groups. They elaborated, stating that the LNU group showed worse 5-year OS (26% versus 62.7%, log-rank p=0.007) and CSS (32.7 versus 68.4%, log-rank p=0.005) rates than the ONU group only in pT3/T4 patients compared to the other stage patients. Moreover, in univariate and multivariate Cox regression analyses in pT3/T4 patients, LRNU was an independent predictor of worse OS (HR: 2.59; 95% CI: 1.44-4.65; p=0.001) and CSS (HR: 2.50; 95% CI: 1.32-4.71; p=0.005) rates than ORNU. This can be attributed to the high-pressure environment during pneumoperitoneum that is created during the laparoscopic procedure. Under pneumoperitoneum, manipulation of a large tumor can create gravitational effects, eventually seeding and implanting cells in the retroperitoneum and bladder.20
Few studies report port-site metastasis after LNU. We have not found a single case of port-site metastasis in the present study. Few laparoscopic port-site metastases were published in the literature in the early years, and researchers proposed that closed-system laparoscopic surgery, avoiding direct contact between instruments and tumor mass and use of laparoscopic bags for specimen extraction might reduce port-site metastasis.21,22 Regarding distal ureter management, we managed most cases with an open extravesical approach and a bladder cuff technique with separate Gibson incision except in 5 cases in which the bladder cuff was not excised. Three of 4 patients developed recurrence in the ureterectomy stump, which was managed with bladder cuff excision later. Adequate bladder cuff excision is paramount in the management of UTUC.23 Another debatable issue is the bladder cancer recurrence-free rate with a surgical approach and factors that increase the likelihood of bladder cancer recurrence after RNU. In our patient series, we found no difference in bladder cancer recurrence rate with the surgical approach. The same results have been published in the literature.24 Few studies,8,25 have reported that LNU was significantly associated with the bladder cancer recurrence rate as compared to ONU (HR: 1.62; 95% CI: 1.18-2.22). In our study, we observed that preoperative URS with biopsy, multifocality of tumor, and previous H/O bladder cancer were significant risk factors for intravesical recurrence after RNU in patients with UTUC. Forty percent of our patients developed bladder recurrence after a median follow-up of 18 months. Various studies have been published regarding the risk factors for bladder cancer recurrence after RNU.26-28
To strengthen our present results, we found that preoperative diagnostic URS was significantly associated with bladder recurrence on univariate analysis but this association was not found on multivariate analysis. Several studies have reported that preoperative URS with manipulation is a risk factor for seeding and eventually bladder cancer recurrence.10,11 Guo et al29 recently indicated in their meta-analysis that preoperative URS did not have a negative impact on OS, CSS, and RFS, but patients were at high risk for intravesical recurrence after RNU.
Study limitations
The main limitation of our series is its retrospective and small study population; potential bias and reporting errors are the main risk factors of any retrospective study. Due to small sample size, results of various variables in univariate and multivariate analysis might be affected. Besides, our cases spanned 16 years with multiple surgeons with varying surgical expertise and learning curves for LNU among surgeons; this might affect the surgical outcome, and we have not clearly identified this point in this study. On the other bright side, we have similarities in the management of distal ureter and distribution of clinicopathological parameters between the 2 groups, which gives a more reliable outcome. We look forward to a prospective study to overcome these limitations, although it is difficult due to rarity of disease.
In conclusion, LNU can benefit patients because of minimal invasiveness, and oncologic outcomes are comparable to those of ONU. Preoperative ureteroscopy with biopsy, multifocality and previous H/O bladder cancer might be risk factors for bladder cancer recurrence after NU.
Acknowledgment
We gratefully acknowledge the contribution of Mrs. Samia Alhashmi, Biostatistician, King Faisal Specialist Hospital & Research Centre, Riyadh, Saudi Arabia for helping in data analysis. We would also like to thank Elsevier (https://www.webshop.elsevier.com) for the English Language editing of the manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 9, 2019.
- Accepted October 22, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}