


Abstract
Objectives: To systematically review the literature to assess the quality of evidence related to corticotomy-assisted orthodontic treatment (CAOT) as adjunctive treatment in orthodontics.
Methods: The study was conducted in the Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia between 2013 and 2014. Various electronic databases were searched and abstracts were retrieved. Defined inclusion criteria were then applied to the obtained original articles for further evaluation by 2 examiners independently. The criteria of selection included human, or animal studies, which assessed some aspects of CAOT and/or the biological principles behind it. Case reports and series were excluded. The quality of the studies was evaluated by the methodological score for clinical trials developed.
Results: Fourteen articles were retrieved initially, but only 12 articles were finally selected for the study. The CAOT was found to accelerate tooth movement by 2-2.5 folds when compared with conventional orthodontic tooth movement. The CAOT was found safe on periodontal health and exhibits no or little risk of root resorption. A localized turnover of alveolar spongiosa and the absence of a hyalinized zone was the acceptable biological explanation of CAOT. There is no evidence to support that CAOT enhances the movement of ankylosed teeth, closing old extraction sites, post-orthodontic stability, or transverse expansion.
Conclusions: Corticotomy-assisted orthodontic treatment should be considered with caution. Long term randomized clinical trials are still needed.
Orthodontists have attempted several methods to decrease treatment time while maintaining good quality of orthodontic treatment.1 Corticotomy-assisted orthodontic treatment (CAOT) is considered one of these modern methods that aims at reducing the treatment time and overcoming some limitations of orthodontic treatment, especially in adult patients.2 The concept of performing surgical cuts to accelerate orthodontic tooth movement is not new. However, it was not introduced properly until the late 20th century when Wilkco et al2-4 proposed selective alveolar corticotomy with augmentation grafting, followed immediately by fixed orthodontic treatment. They patented and trade marked their technique as Periodontally Accelerated Osteogenic Orthodontics (PAOO). They observed a rapid orthodontic movement following PAOO, which was estimated to be 6-8 months faster than the conventional orthodontic treatment.2-4 Several indications and effects of CAOT were reported, which included: reducing treatment time and facilitating the treatment of several orthodontic modalities such as impacted canine traction, closing old extraction sites, slow expansion, post-orthodontic stability, open bite correction, the treatment of bimaxillary dento-alveolar protrusion, molar intrusion, and manipulation of anchorage.4-23 Controversies exist in regard to the different surgical and orthodontic aspects of the technique of CAOT. For example, the use of buccal and palatal decortication with the help of bone grafting was adopted in the initial description of the procedure with a rate of activation of the fixed orthodontic appliance after CAOT of 2 weeks. This showed a 3-4 fold increase in tooth movement.2-4 Others, however, used only buccal decortications, and showed a 2-2.5 fold increase in tooth movement.14,24,25 Recently, modifications of the CAOT technique such as the use of piezocision and corticision, which are performed without reflecting gingival flaps, were introduced in an attempt to minimize the risk associated with the conventional technique. These techniques, while all involve surgical cortical injuries, they seem to be different in their effects and healing process and so far, they were described only in case reports.26,27 The biological principle behind CAOT was investigated in many animal studies. The increasing velocity of tooth movement after corticotomy (cortical injuries) was attributed to accelerating bone turnover, which was called the regional accelerating phenomenon (RAP). The RAP was defined as a re-organization activity and physiologic event that occurred adjacent to the site of injury, resulting in regional decrease in bone density in the healthy tissue.22 Most of the animal studies confirmed RAP as the main biological mechanism behind the acceleration of orthodontic tooth movement. The most recent explanation of the biological mechanism behind CAOT concluded that localized selective decortication surgery in combination with orthodontic tooth movement results in a rapid alveolar bone remodeling in bone marrow cavities, leads to reduced hyalinization of the PDL, and absence of the lag phase during later stages of orthodontic tooth movement.12 That was used to explain the observed decreased root resorption in the corticotomy side, an apparently added advantage to CAOT.23
Rationale
Corticotomy-assisted orthodontic treatment was initially presented in case reports.2-6 Many human and animal studies were later conducted to test the effectiveness of this technique.7-17,24,25 Most published papers indicated that performing cortical and alveolar bone cuts around the roots of teeth would help accelerate tooth movement.1 However, the evidence of the outcome and the effectiveness by experimental studies has not been well-documented especially in the presence of an increasing number of case reports. In addition, the available case reports and experimental studies lack consensus on the biological basis, the described technique of CAOT, and the indications of its use. These aspects need to be verified and supported by scientific evidences.
The objective of this systematic review was to evaluate the quality of evidence behind the following: 1) CAOT accelerates tooth movement and enhances the traction of impacted canines when exposed surgically, the movement of ankylosed teeth, closure of old extraction sites, maxillary expansion, open bite correction, treatment of bimaxillary protrusion, and post orthodontic stability. 2) The technical variables involved in CAOT including the rate of activation, area of activation, the use of bone graft, and the use of flap versus flapless procedure. 3) The safety of CAOT compared with conventional orthodontics. 4) The biological principles behind CAOT in accelerating orthodontic movement in animal studies.
Methods
Search strategy
This systematic review was conducted in the Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia between 2013 and 2014. A literature survey was conducted to identify all aspects of the studies that examined the effect, indications, and the biology of corticotomy. MEDLINE in process and other non-indexed citation, PubMed, Evidence Based Medicine (EBM) reviews-American College of Physicians journal club, and all EBM Cochrane Research Systems databases from 1980 to July 2013 were searched. Keywords used included corticotomy, orthodontics, corticotomy-assisted, accelerated orthodontics, regional accelerating phenomena (RAP), piezocision corticotomy and corticision, with their respective abbreviations according to the search engine used.
Eligibility criteria
Randomized controlled trials, prospective controlled studies, and retrospective controlled trials were considered eligible to be included in the systematic review. The studies had to be in English language only, addressing at least some aspect of CAOT in both human and animals. Case reports, case series, and review articles were excluded. Eligibility of potential studies was determined by reading the title and abstract of each article identified by the search, and then full texts of the articles were retrieved from the selected abstracts/titles. Two reviewers (orthodontists) were assigned to review the full text of articles and were calibrated to use the review process adopted in the present review. A study was ordered for the full text if at least one of the 2 reviewers considered it to be potentially relevant, or if the title and abstract did not provide sufficient information. The final selection of included articles was independently performed by 2 of the authors. Any discrepancies were solved through discussion until consensus was accomplished. The reference lists of the retrieved articles were also searched manually for additional relevant publications that may have been missed in the search.
Results
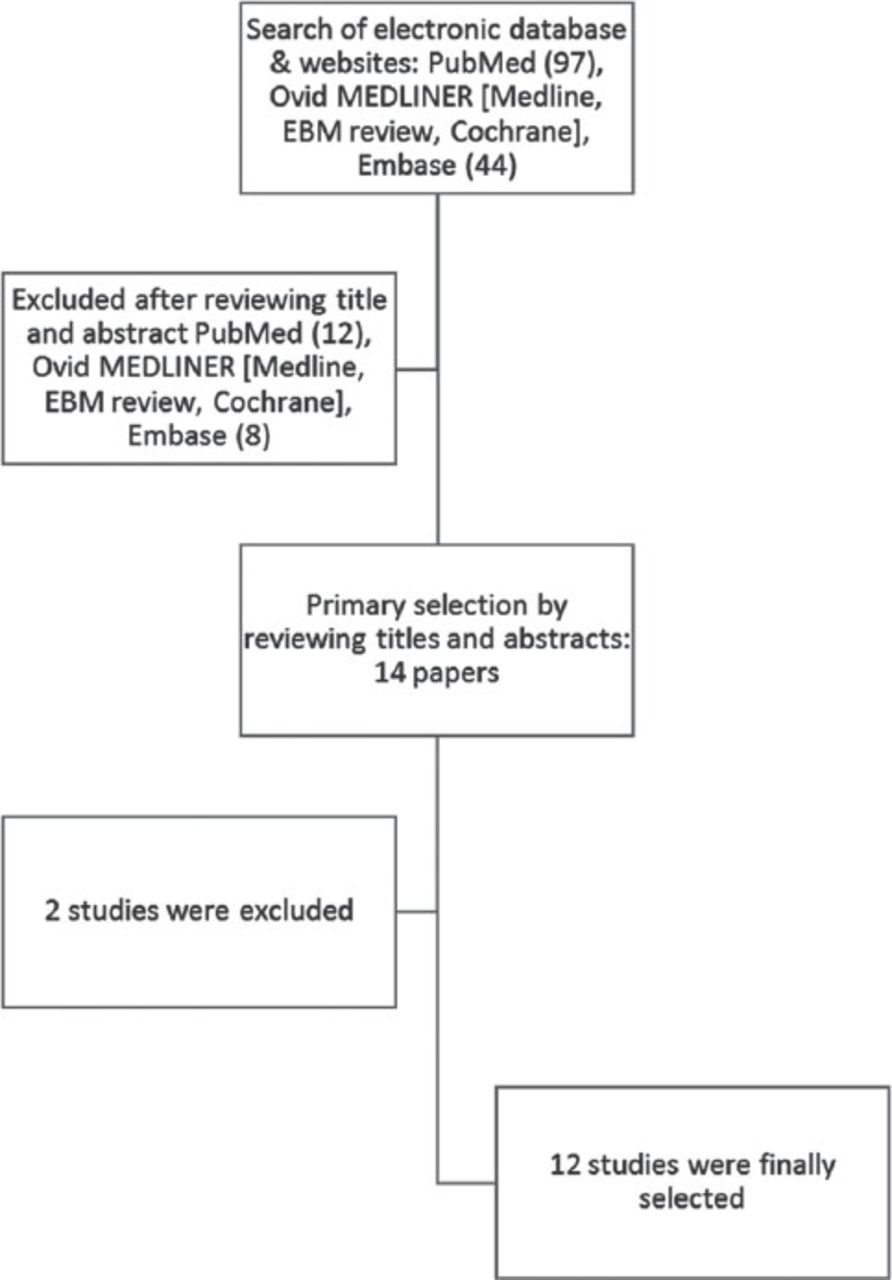
The search strategy resulted in 14 articles. All of these articles were analyzed according to the inclusion/exclusion criteria, and 12 articles qualified for the final analysis (7 animal and 5 human studies). Two articles30,31 were rejected because the surgical techniques used were combined corticotomy and osteotomy cuts,30 and the other one was performed without a control group.31 The review details and selection process is given in Figure 1 as described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.32 The inter-examiner agreement (Kappa statistics)33,34 for inclusion of studies was 0.76.
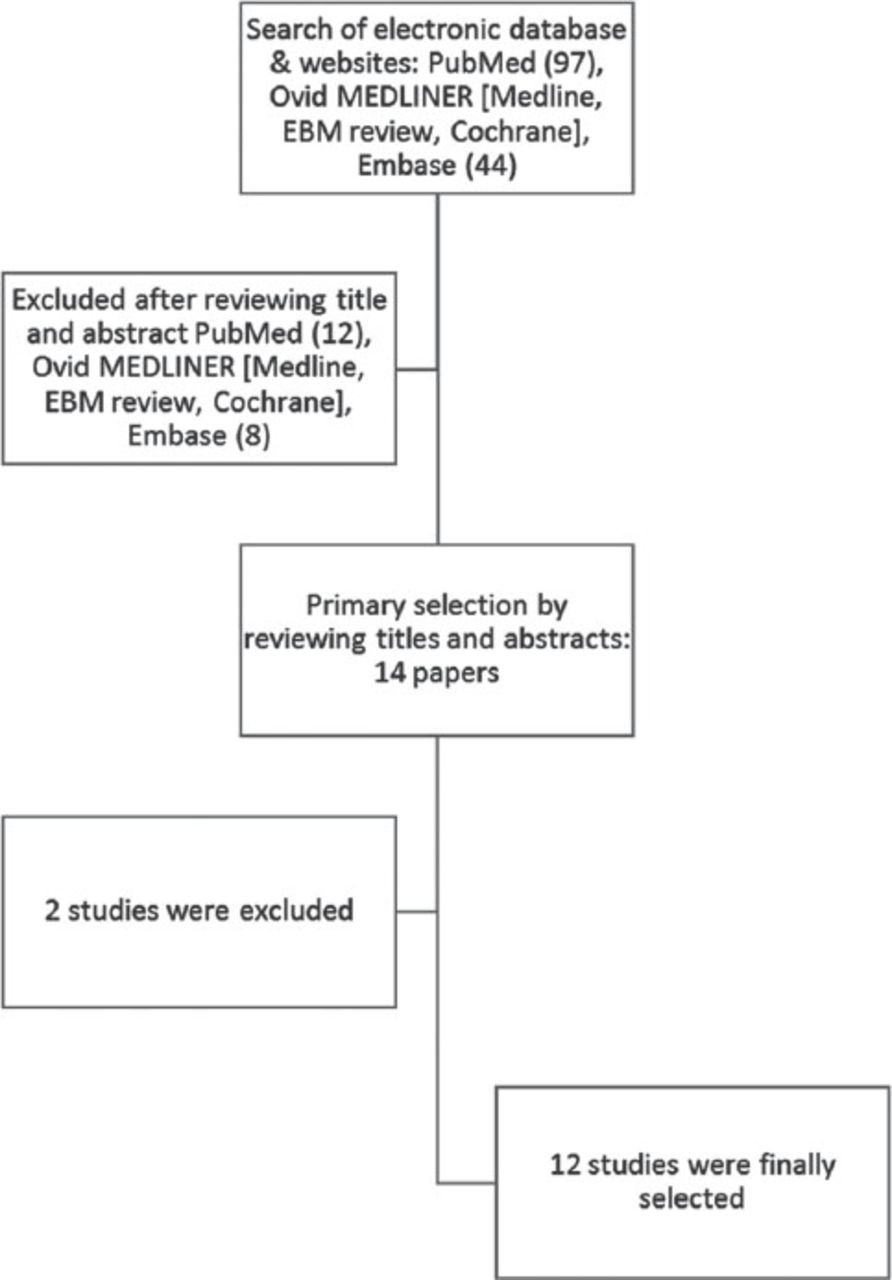
Systematic search and selection strategy as described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.32 EBM - evidence based medicine
The quality assessment criteria modified from Lagravere et al28 were applied for each article including those conducted in animals (Tables 1 & 2). However, the methodological score was modified in some aspects related to the population and selection criteria to evaluate the appropriateness of the animal model used and its equivalence to humans. All human studies were randomized, controlled, clinical trials, except one, which was a retrospective controlled trial.35 In the included studies, the average age of the patients was from 18-25 years, except in one study where the age was 11-12.9 years.13 All animal studies were longitudinal and prospective with opposite side controls in most of the studies. Animal models used were dogs and rats. Summarized data of the 12 studies included are shown in Tables 1 & 2. After the selection, the criteria and final scores for each article score are presented in Tables 3 & 4.
Animal studies related to corticotomy-assisted orthodontic treatment (CAOT) that fulfilled the inclusion criteria.
Human studies related to corticotomy-assisted orthodontic treatment (CAOT) that fulfilled the inclusion criteria.
The quality assessment criteria and final methodological scores of selected articles.
Summarized data and final methodological scores of selected articles included in a study in Saudi Arabia.
Corticotomy-assisted orthodontic treatment efficacy
Four animal studies and 5 human studies confirmed that CAOT can accelerate tooth movement by an average of 2-2.5 folds when compared with conventional orthodontic tooth movement.13,14,24 Each human study covered different aspects of CAOT. Abou-Ela et al14 presented strong evidence (score=8.5) that CAOT accelerates canine retraction by 2 folds in adult patients treated by fixed orthodontic treatment with extraction of premolars. Fischer13 presented moderate strength evidence that CAOT accelerates the traction of palatally positioned canines in children (score=7.5). Shoreibah et al24 showed that CAOT significantly reduced the treatment time of anterior crowding (score=7.5). Lee at al35 showed that CAOT reduces treatment time in the treatment of bimaxillary protrusion (score=5.5). There is no evidence to support that CAOT enhances transverse maxillary expansion, closure of old extraction site, open bite correction, or post-operative stability when compared with conventional orthodontic treatment.
Technique description. Area of activation
All the included studies, performed buccal corticotomy as the preferred area of intervention14,24,25 except Fischer13 who performed buccal and palatal corticotomies for canine dis-impaction.
Rate of activation
No study was carried out to assess the correct rate of activation. However, each study mentioned their protocol of activation. Some24,25 activated every 2 weeks to relieve crowding, while others13 started canine traction every 4-6 weeks, and then changed to a 2-week interval. The use of nickle titanium coil springs to deliver continuous force eliminated the need for activation in Aboul-Ela et al’s study.14 There is no evidence indicating that piezocision corticotomy or corticision techniques are equivalent to conventional CAOT.
Technique safety
The effect of CAOT on periodontal health was studied from different aspects, which included; probing depth, level of attachment, gingival recession, and bone density. The studies found no significant difference in all measured variables before and after the CAOT treatment in comparison with conventional orthodontic technique.13,14,24,25 Furthermore, Shoriebah et al24,25 studied the safety of the CAOT procedure and found that the procedure is safe from all studied aspects. In addition, Shoriebah et al25 reported that the incidence of apical root resorption and periodontal problems associated with orthodontic tooth movement were reduced by using CAOT. The incorporation of bone graft material significantly increased the alveolar bone density in adult patients.
Biological principle of CAOT
The biological mechanism behind the acceleration effect of CAOT was described as RAP by 6 out of the 7 animal studies. Throughout the review, it was concluded that CAOT is a broad periodontium-mediated phenomenon and the spongiosa likely plays a dominant role in rapid tooth movement through significant decalcification and increase in catabolic and anabolic activities. The accelerated tooth movement with CAOT was explained on the basis of the absence of hyalinized zone in the periodontium and a lack of the lag phase that occurred as a result of selective alveolar decortication.
Discussion
This systematic review is the first review to evaluate the effectiveness of CAOT from different aspects, and the review disclosed some interesting findings. A recent systematic review,36 which evaluated the effectiveness of several interventions of accelerating orthodontic tooth movement was not included because it did not focus on CAOT in particular.
After applying inclusion criteria, 7 animal studies and 5 human studies were included. Studies were rated according to the modified methodological score for clinical trials by Lagravere et al.28 It is a more objective method of assessment, which has been used in many systematic reviews related to orthodontics.37,38 It was modified in some aspects to be suitable for the assessment of the animal studies assessment. Kappa scores measuring levels of agreement between the 2 reviewers in assessing data extraction and quality scores of the included articles were very good, and thus indicated the results were reliable. The CAOT was found to be an effective method in accelerating tooth movement with a rate that ranged from 2-2.5 fold. The included human clinical trials found that CAOT was effective to accelerate canine and anterior teeth retraction, alleviate crowding, and enhance the traction of impacted canines with evidence ranging in strength between high to moderate levels of strength. All the human studies shared some shortcomings, such as the inadequacy of the sample size that was not pre-estimated, lack of reliability, absence of blinding, and dropouts that were not included in data analysis. In addition, the study that was carried out to assess the effectiveness of corticotomy in the treatment of palatally impacted canines did not clarify the selection criteria in terms of inclination and depth of impaction. Although the force magnitude was measured, the orthodontic technique used for traction was not identified.13 We found no evidence to support the ability of CAOT to enhance maxillary expansion, close old extraction space, open bite correction, or post-orthodontic stability when compared with conventional orthodontics, despite the presence of several case reports regarding these indications.
There was lack of consensus in the literature on the technique description of CAOT. Wilcko et al2 was the first to thoroughly describe the technique used. He advocated papillary preservative buccal and palatal flap reflection with bone grafts. All the randomized clinical studies that were included used the buccal sides as the preferred areas of intervention14,24,25 except for Fischer13 who used buccal and palatal corticotomies for canine dis-impaction, and there was no evidence on the use of bone grafting in any of the studies. The rate of activation reported was every 2 weeks in the study that used the technique to relieve crowding,24,25 while it was 4-6 weeks for canine dis-impaction and then changed to 2 weeks intervals.13 Most of the studies in our systematic review followed the protocol of Wilcko et al.2
Based on the variability in conclusions of the animal studies regarding the timing of occurrence of the localized rapid turnover of bone, which varies from occurring at the early stages, 12-21 days after the surgical intervention,8,11 a randomized clinical trial is essential to determine the appropriate time and rate of activation. Although piezocision and corticision are reported in the literature, no evidence was found to support these techniques. Beside the existing evidence that corticotomy enhances and accelerate tooth movement, the present systematic review found that CAOT is a safe procedure with no significant effects on probing depth, level of attachment, bone density, or root resorption.24,25,36 In addition, Shoriebah et al25 reported less root resorption with the technique than that reported by other studies.2,39
The biological mechanism behind CAOT was best explained by 2 studies conducted in rat models.7,12 The acceleratory effect was attributed to RAP as described earlier by Frost.22 Sebaoun et al7 described, in detail, the tissue response to selective decortication without tooth movement as an increase in a localized turnover of alveolar spongiosa, which is assumed to be extensive and pervasive. It was described as a broad periodontium-mediated phenomenon and emphasized that spongiosa likely plays a dominant role in rapid tooth movement. In Sebaoun’s study, catabolic and anabolic activities increased by 3 folds. Significant decalcification of spongiosa and increased periodontal surface were increased by 2 folds after 3 weeks, and then decreased to a steady state by the eleventh week.7 Unfortunately, corticotomy, in this study, was assessed in the absence of any tooth movement, which does not explain the RAP during CAOT. The other animal study attributed the accelerated tooth movement observed in CAOT to absence of hyalinized zone and lag phase that occur as a consequence to the selective alveolar decortication.12 Although it is claimed that catabolic and anabolic activities in rats are parallel to those in humans, the rat model had different bone turnover rates and dynamics of orthodontic tooth than that of a human.7,23 In all human and animal studies, CAOT was referred to as a reversible phenomena. A second corticotomy procedure was advised to be carried out after 4 weeks from the initial surgery to maintain the effect of corticotomy for a longer time.15
Limitations
A notable finding was that all the studies were of medium level of evidence except one human study14 that scored high evidence. Many of the studies although prospective randomized, had serious defects. The most serious shortcomings were the study design in combination with small sample size that was not predetermined. Other shortcomings were absence of blinding, reliability assessment, and the indication of drop out. The restrictions concerning the English language selected in database searching might imply that some studies were not identified. The strength of the evidence in a systematic review is probably more dependent on assessing the quality of the included studies than on the degree of comprehensiveness.
Conclusions
Corticotomy-assisted orthodontic treatment was found an effective method in accelerating tooth movement. The highest evidence for the effects of CAOT comes from only one high level, and other several human’s studies ranked as moderate strength evidences. The conclusions taken from these studies should be considered with caution. These are: CAOT accelerates space closure, traction of palatally impacted canines, and resolves crowding of incisors by 2-2.5 fold when compared to conventional orthodontic tooth movement, CAOT is a safe procedure with similar periodontal health to conventional orthodontic treatment. The CAOT exhibit no or fewer risk on root resorption. The described techniques based on buccal corticotomy without any bone grafting with possible activation every 2 weeks except during the use of Niti coil spring, which ensured a continuous force that could be adequate. Selective alveolar decortication causes an increase in a localized turnover of alveolar spongiosa, which is extensive and pervasive but reversible. A coupled mechanism of bone resorption and bone formation during the earlier stages of treatment, which allows a steady and continuous tooth movement, immediately after initial tooth displacement, without a lag phase that is usually seen during conventional orthodontic tooth movement.
Recommendations
This review recommends additional high quality randomized controlled clinical trials to compare CAOT with conventional orthodontic treatment with adequate sample size, double blinded, counting for inter-examiner reliability to strengthen the evidence.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 6, 2015.
- Accepted May 17, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}