


Abstract
Objectives: To evaluated Fetuin-A levels of patients admitted in the intensive care unit with a diagnosis of sepsis.
Methods: This study was conducted at the Faculty of Medicine, Çanakkale Onsekiz Mart University Hospital, Çanakkal, Turkey, between February 2015 and October 2015. Forty septic patients were included in the study. Subsequent to clinical suspicion of sepsis, serum levels of C-reactive protein (CRP) and procalcitonin; and white blood cell (WBC) counts were evaluated at 3 time-points: 0 (basal), 24, and 72 hours.
Results: The mean Fetuin-A levels at the 3 time-points were 58.5 ± 29.2 ng/mL, 40.9 ± 23.6 ng/mL, and 47.8 ± 25.7 ng/mL, respectively. Fetuin-A levels at 24 hours were significantly lower than the basal level (p<0.05), where as no significant difference was observed between the basal levels and those at 72 hours (p>0.05). Correlation between the temporal changes in Fetuin-A levels and the changes in other inflammatory markers (CRP, procalcitonin and WBC) was examined. Fetuin A was found to have only a negative correlation with serum procalcitonin level (p<0.05).
Conclusion: In this study, serum Fetuin-A levels in septic patients decreased significantly in the first 24 hours, followed by an insignificant increase at 72 hours. These findings suggest that monitoring of Fetuin-A levels may help predict the time of occurrence of sepsis and prognosis of sepsis.
Fetuin was first extracted from fetal bovine serum by purification in 1944.1 It is a major plasma protein of fetus. During fetal development, it is known to be secreted from many organs such as liver, brain, and the gastrointestinal tract.2-4 In adults, liver is the main source of secretion.5 Fetuin obtained from humans was earlier referred to as Alpha-2 Heremans Schmid Glycoprotein (AHSG).6 After the identification of Fetuin-B in 2000s, the term AHSG was replaced by Fetuin-A.7 Fetuin-A is known to be associated with many functions in the body. In cell culture studies, Fetuin-A was shown to play a role in cell adhesion, proliferation and differentiation8 and in the modulation of inflammatory responses9 and lipid transport.10 Owing to its effects on hyperlipidemia and calcification, it was considered as a marker for atherosclerosis.11 While Fetuin-A is a negative acute phase protein in inflammation;9 it is conversely a positive acute phase protein12 during injury. Most of the information related to the levels of Fetuin-A in inflammatory states has emanated from animal studies. Fetuin-A levels have been shown to vary depending on the time in different sepsis models.13 Its relation with specific illnesses such as kidney damage,14 liver diseases,15 and coronary artery disease16 has been shown in clinical studies. However, to the best of our knowledge, temporal variations in Fetuin-A levels in systemic infections like sepsis have not been investigated in clinical settings. In this study, we evaluated the early and late changes in Fetuin-A levels of patients admitted in intensive care unit with a diagnosis of sepsis.
Methods
This study was conducted at the Faculty of Medicine, Çanakkale Onsekiz Mart University Hospital, Çanakkal, Turkey, between February 2015 and October 2015 after obtaining the Local Ethics Committee Approval (Decision No: 2014-25, dated 24.12.2014). Forty adults patients (age >18 years) who were admitted in the intensive care unit with a diagnosis of sepsis were included in the study. Written consent was obtained from patients who were conscious, after informing them about the study. For unconscious patients, consent was obtained from their first degree relatives. Patients under the age of 18 years, post-operative patients or those diagnosed with traumatic injury or ischemic injury were excluded from the study. The criteria of International Sepsis Guidelines17 were used to establish the diagnosis of sepsis. Blood and urine culture from all patients and tracheal aspirate culture from the intubated patients were used to confirm the diagnosis of sepsis.
Personal information of patients (gender, age), primary infection site (namely, urinary tract, pulmonary, venous catheter or other), Acute Physiology And Chronic Healthy Evaluation II (APACHE II) scores18 and Sepsis related Organ Failure Assessment (SOFA) scores19 were recorded.
Venous blood samples of the participants were collected from the antecubital vein after an overnight fast. Following clinical suspicion of sepsis, serum analysis was performed at 3 time-points: 0 hour (basal), 24 hours and 72 hours. Blood samples were centrifuged at 4000 rpm 10 minutes. Serum samples were stored at -80°C until analyzed. Serum levels of Fetuin-A, C-reactive protein (CRP), and procalcitonin and white blood cell (WBC) counts were determined for all patients included in the study. Serum procalcitonin and CRP levels in fasting subjects were analyzed using ROCHE module Cobas 6000, kits were procured by ROCHE diagnostics. The WBC counts were performed in Beckmann-Coulter analyzer model LH within one hour.
Serum samples were stored at -80°C and analyzed at the end of the study period. Serum Fetuin A levels were analyzed with ELISA kits using ELISA microplate strip washer (ELX50; BioTek Instruments, USA) and ELISA microplate reader (ELX 808; BioTek Instruments). Fetuin A levels were determined using commercially available ELISA kits from MyBiosource, Inc. (San Diego, CA, USA). The optical density absorbances were read at 450nm in the microplate reader, and the concentrations of Fetuin A were calculated. The analytic sensitivity of Fetuin A was 1.0 ng/mL. The within assay, inter-assay, and intra-assay precision of Fetuin A were under 10%.
Statistical analysis
All data analyzes were performed using “IBM SPSS Statistics 19” statistical analysis software owned by the Çanakkale Onsekiz Mart University. Patient age, APACHE II and SOFA scores were evaluated as average and standard deviation; gender and primary infection site were evaluated as percentage frequency (%). Fetuin-A, CRP, procalcitonin and WBC values were evaluated as average and standard deviation. Non-parametric Friedman test was used for statistical intra-group comparison of these laboratory tests. Non-parametric Wilcoxon test was used for pairwise intra-group comparison of Fetuin-A, CRP, procalcitonin, and WBC values at the 3 time-points. Correlation between Fetuin-A and other inflammatory markers; CRP, procalcitonin, and WBC was assessed. For this purpose, first the differences between basal-24 hours, 24 to 72 hours, and basal to 72 hours were calculated for each marker. Subsequently, it was compared with Spearman correlation test. The obtained results were tabulated and relevant graphs prepared.
Results
Data pertaining to age, gender, primary infection site, APACHE II and SOFA scores of patients are summarized in Table 1.
Demographic characteristics of 40 adults patients admitted in the intensive care unit with sepsis.
Average (±standard deviation) values of CRP, Procalcitonin, and WBC and statistical results of intra-group comparison for each marker (basal-24 hours, 24-72 hours, basal-72 hours) are shown in Table 2. The CRP levels showed a progressive increase over time. Procalcitonin and WBC values were highest at 24 hours and decreased below basal level at 72 hours. All intra-group differences with respect to CRP, Procalcitonin, and WBC were statistically significant.
Intra-group statistical analysis of C-reactive protein (CRP), procalcitonin, and white blood cell counts.
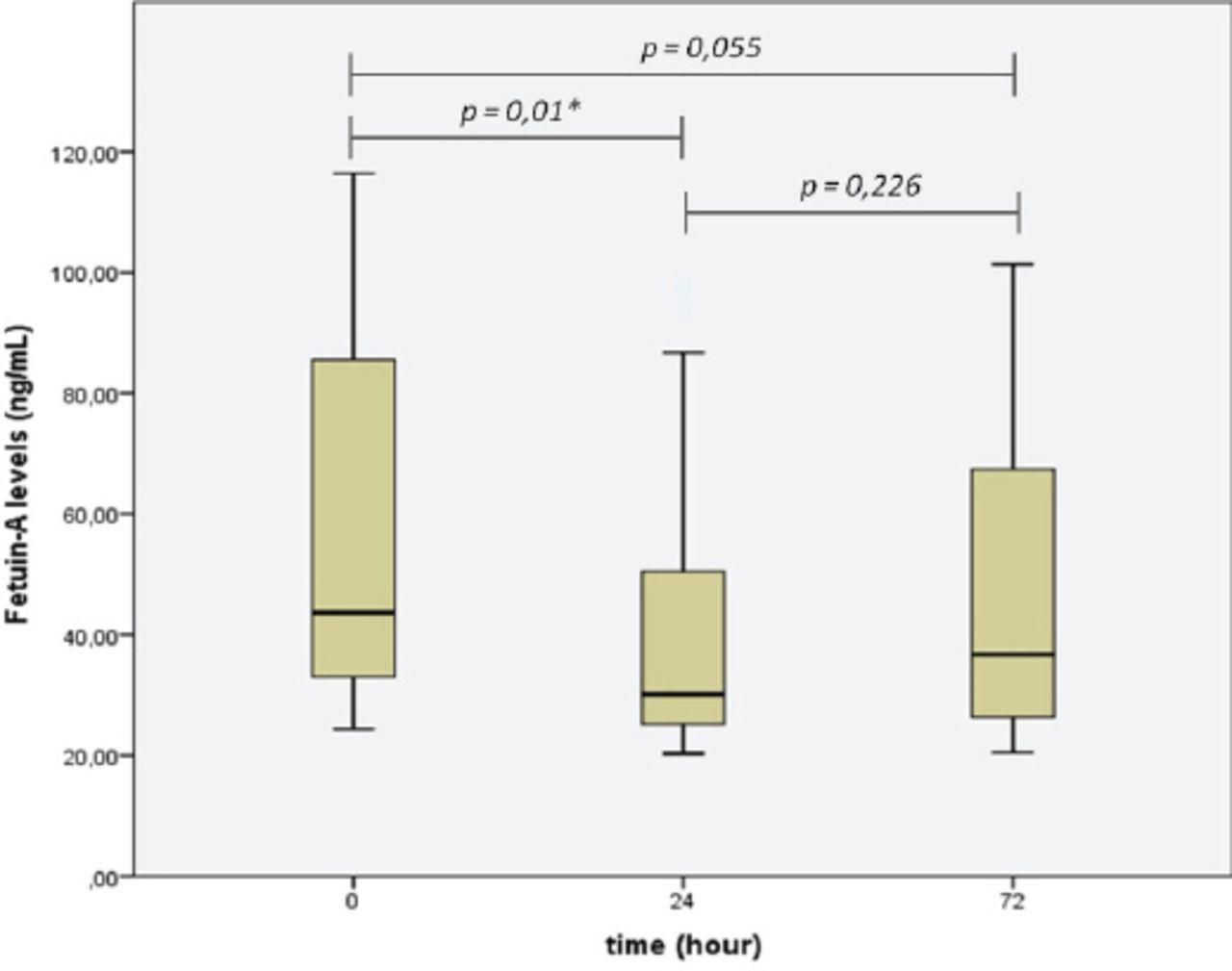
Fetuin-A levels measured at 24 hours were significantly lower (p<0.05) than the basal levels. These did not reach basal levels (p>0.05) at 72 hours despite an increasing trend. The difference between basal levels and those at 72 hours was not statistically significant (p>0.05, Table 3). The changes in Fetuin-A levels over time are summarized in Figure 1.
Intra-group statistical analysis of Fetuin-A levels (ng/mL).

Graphical display of the changes in serum concentration (ng/ml) Fetuin-A levels over time. *p<0.05
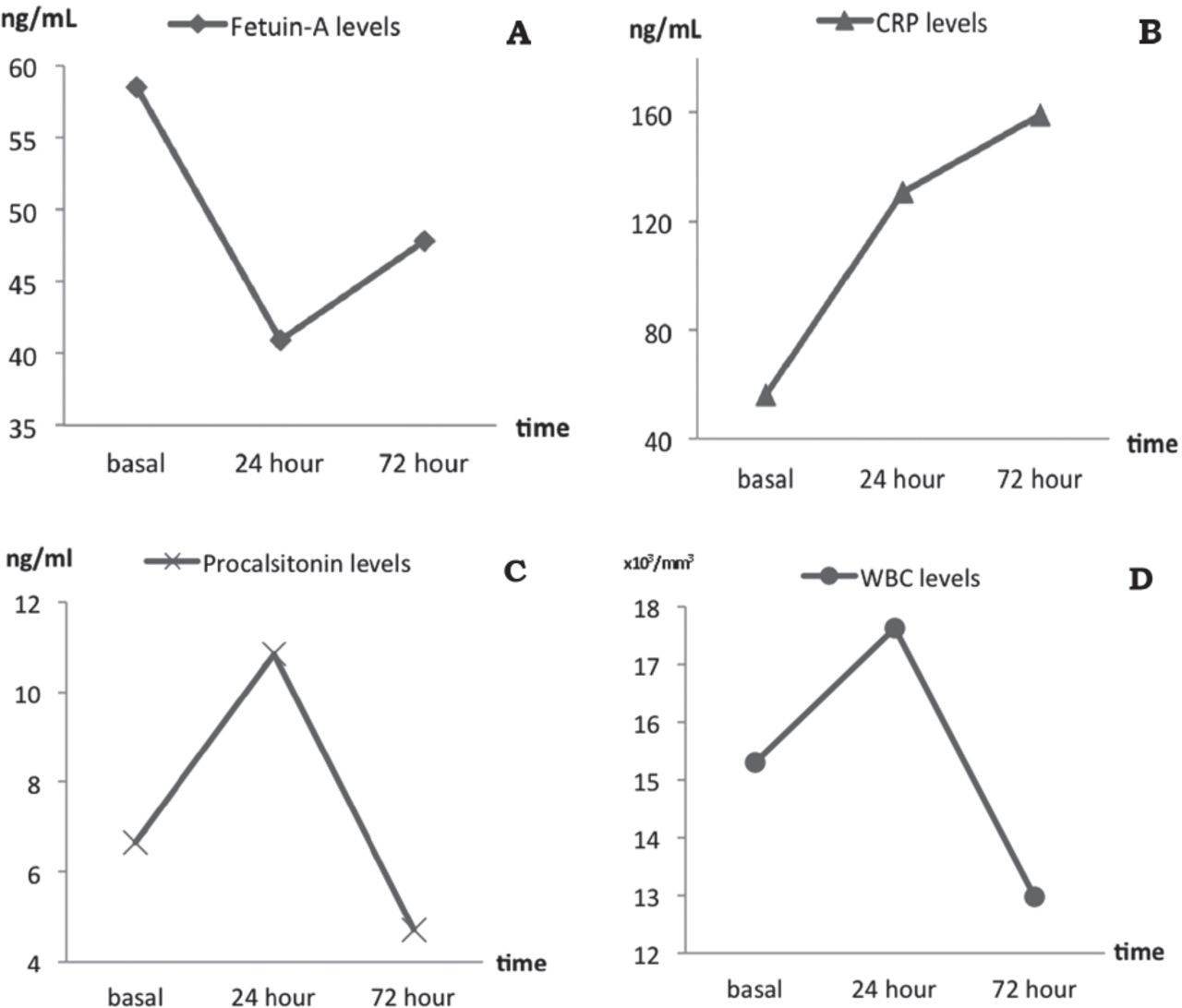
The correlation of the observed differences between Fetuin-A values and the other inflammatory markers (CRP, procalcitonin, and WBC) at the successive time-points (basal-24 hours, 24-72 hours and basal-72 hours) are shown in Figure 2 & Table 4. In Figure 2, Fetuin-A exhibits a negative relation with procalcitonin and WBC over time, but no relation with CRP. However, on statistical assessment, a negative correlation was observed only between Fetuin-A and procalcitonin levels with respect to the difference between basal-24 hours and 24-72 hours values (p<0.05, Table 4).
Correlation of the differences calculated between Fetuin-A values and CRP, procalcitonin, and WBC’s basal - 24th hours, 24th - 72nd hours, and basal - 72nd hours.
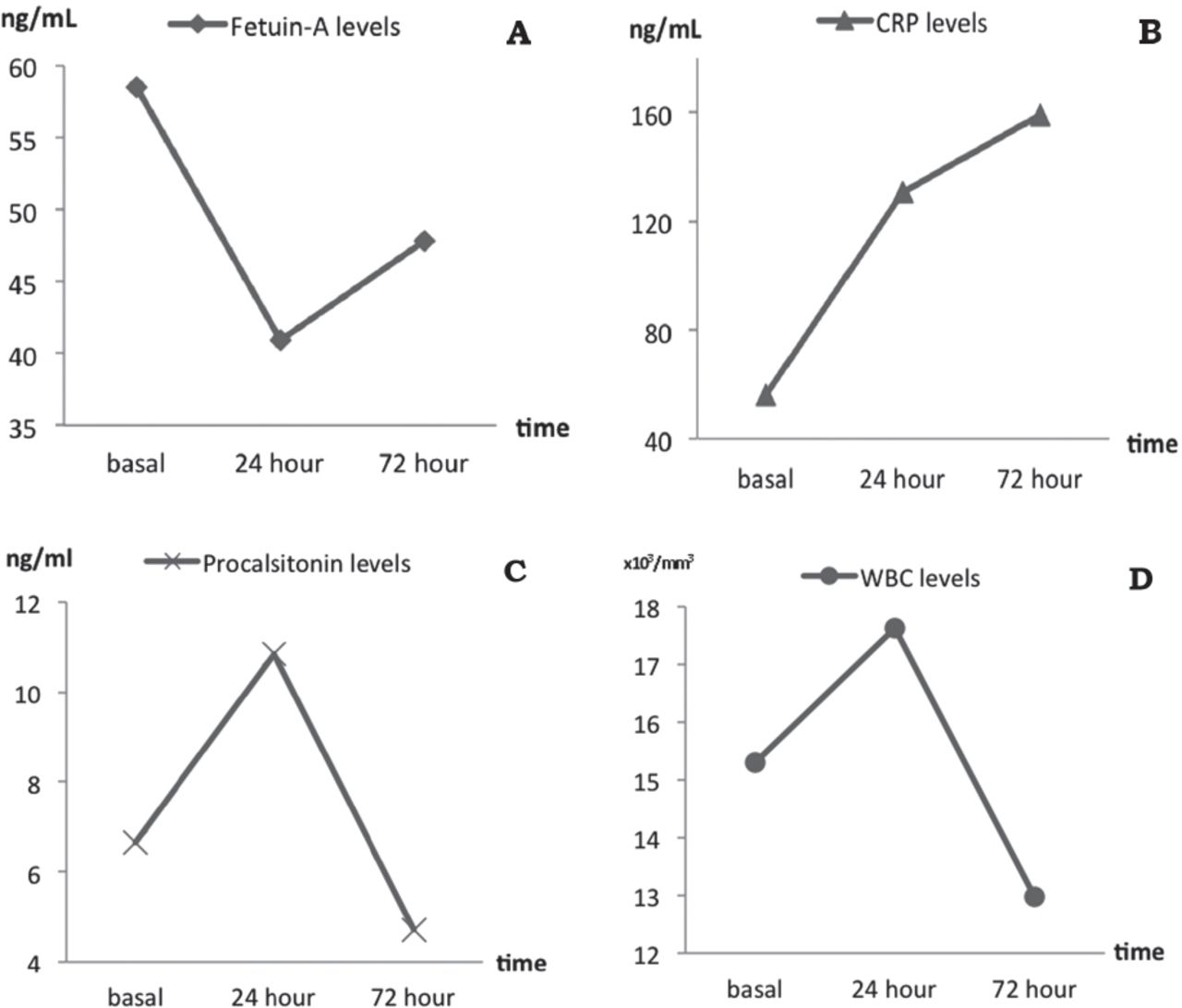
Graphical illustration of the temporal changes in serum concentration of A) Fetuin-A, B) C-reactive protein (CRP), C) procalcitonin, and D) white blood cell (WBC) counts.
Discussion
In this study, serum Fetuin-A levels of patients diagnosed with sepsis showed a significant decrease (p<0.05) in the first 24 hours following the diagnosis. Fetuin-A level measured at 72 hours revealed an increasing trend; however, this increase was not significantly higher than those recorded at 24 hours (p>0.05). Much of the currently available information pertaining to changes in Fetuin-A levels during inflammation has emanated from experimental studies. Ombrellino et al20 reported that Fetuin-A was a negative acute phase reactant and had an anti-inflammatory feature experimentally. Gangneux et al21 reported inflammation-induced down-regulation of Fetuin-A levels in Sprague-Dawley type rats. The studies on humans have generally focused on specific diseases. Decrease in serum Fetuin-A levels by 20% to 30% has been reported in pancreatitis, chronic renal insufficiency, rheumatoid spondylitis, and rheumatoid arthritis.22-25 In our study, we observed a significant decrease in Fetuin-A levels of septic patients (maximum 30.05%, p<0.05). The extent of decrease varied over time. Only a few studies have characterized the temporal changes in Fetuin-A in inflammatory states. Li et al13 reported time-dependent changes in Fetuin-A levels in a rat model of sepsis established via endotoxemia induced by intraperitoneal lipopolisaccharide injection (LPS) and cecal ligation and puncture (CLP). Fetuin-A levels in both groups started decreasing within 2-6 hours and reached their lowest value (50% to 60% decrease) between 24-48 hours. The levels started to increase again approximately 72 hours later. However, Fetuin-A values in the CLP group returned back to their initial levels at 72 h, whereas levels in the LPS group did not reach the initial values despite showing some increase. Data obtained from our study is consistent with the results obtained from animal studies. In our study, a significant decrease in Fetuin-A level was observed at 24 hours following sepsis diagnosis (69.9% of the initial value, p<0.05). At 72 hours, the values had not completely returned back to normal despite the increase (81.8% of the initial value, p>0.05). On a review of literature, we found only one study that evaluated Fetuin-A levels in human sepsis, and this study focused on acute renal damage; moreover, Fetuin-A levels were measured at a quite late period (12 weeks later) to evaluate the effect of antibiotic therapy.26 There is only one study that showed temporal changes in Fetuin-A in the context of other inflammatory diseases. Kuśnierz-Cabala et al23 evaluated the change in Fetuin-A levels over time (on 1st, 3rd, 5th, and 7th days) in 28 patients with mild pancreatitis and 12 patients with severe acute pancreatitis. They reported a notable decrease in Fetuin-A levels on the first day; however, no significant change was observed over the subsequent days.
There are many factors that can affect Fetuin-A levels in humans. Currently available evidence suggests that Fetuin-A is a positive acute phase reactant in cases such as traumatic injury, cardiovascular disease, and cerebral ischemia.27,28 Wang et al29 examined temporal changes in Fetuin-A levels in a rat model of ischemic injury. In that study, Fetuin-A levels peaked at 24-48 hours and returned back to normal levels by 72 hours. In order to minimize bias in our study, post-operative patients and those with traumatic and post-ischemic injury were excluded from the study.
Inflammatory cytokines are considered to be the reason for changes in Fetuin-A levels throughout the inflammation period. Studies have shown that pro-inflammatory cytokines such as TNF-α, IL-1, IL-6, and IFN-γ decrease Fetuin-A secretion from the liver.13 Li et al13 showed that a 50-100 ng/mL increase in TNF-α, one of the early cytokines, caused Fetuin-A levels to drop by 50% to 60%. In addition, a small increase of 10-50 ng/mL in IFN-γ levels (another early cytokine) caused Fetuin-A levels to drop by 50% to 70%. On the other hand, late mediators of inflammation are believed to cause increase in Fetuin-A levels. Serum levels of HMGB-1, which is a late-term mediator and passively excreted from necrotic cells, were shown to peak between 24-36 hours in animal models of endotoxemia and sepsis.30 Therefore, the increase in Fetuin-A levels observed at 72 hours is believed to be induced by HMGB-1.9,13 This also explains why a subsequent elevation in Fetuin-A levels was not observed until day 7 in the acute pancreatitis study of Kuśnierz-Cabala et al.23
In conclusion, this is the prospective clinical study to demonstrate a significant decrease in serum Fetuin-A levels in the first 24 hours following a diagnosis of sepsis; however, the subsequent increase in serum Fetuin-A levels during the late-period was not found to be statistically significant. These findings suggest that monitoring of Fetuin-A levels in patients diagnosed with sepsis may help predict the time of occurrence of sepsis and prognosis of sepsis. However, further studies with a larger number of patients are required to draw more definitive conclusions.
Acknowledgment
This study was supported by the Scientific Research Projects Coordination Unit, Çanakkale Onsekiz Mart University, Çanakkale, Turkey. We would like to thank Enago for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This study was supported by the Scientific Research Projects Coordination Unit, Çanakkale Onsekiz Mart University, Çanakkale, Turkey (Project Number: TSA-2015-517).
- Received March 2, 2018.
- Accepted June 11, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}