


Abstract
Objectives: To determine the prevalence of positive screening of body dysmorphic disorder (BDD) among patients seeking cosmetic surgeries in plastic surgery and oculoplastic surgery clinics.
Methods: The survey of this cross-sectional study was self-administrated and distributed among adults pursuing cosmetic surgeries in plastic surgery and oculoplastic surgery clinics at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, between March 2019 and March 2020. The BDD questionnaire was validated, and a highly sensitive and specific tool was used to identify patients with BDD. Ethical approval was granted by the Research Ethics Committee. All analytic studies were performed using IBM SPSS, version 24.
Results: A total of 344 patients participated in this study with a mean age of 39.66 ± 13.76 years. Of these, 296 (86%) were women and 298 (86.6%) were Saudi. The prevalence of positive screening for BDD was 19.2%. The most commonly requested procedures were abdominoplasty (21.2%) and skin lesion removal (21.2%). Smoking was found to be significantly associated with BDD with 21.2% of smokers having it (p<0.010).
Conclusion: Body dysmorphic disorder was unrecognized among patients pursuing cosmetic surgeries. One-fifth of patients requesting cosmetic procedures are potential cases of BDD requiring psychiatric evaluation and treatment. We recommend implementing screening protocols to identify cases before surgical plans.
Body dysmorphic disorder (BDD), also recognized as dysmorphophobia, is a DSM-V somatoform condition characterized by concerns about an imagined defect in appearance causing clinically major distress or functional damage that may extend to suicide.1-4 Patients tend to exhibit repetitive skin picking, mirror checking, and grooming behavior. While different body parts can be involved, BDD mostly involves parts related to appearance, such as the face.2 Moreover, most individuals have minor dissatisfactions related to personal image, which is not considered to be serious unless this dissatisfaction consumes most of the individual’s thoughts and actions that might progress to severe disorders such as self-harm, anxiety, depression, and undergoing unneeded plastic surgery procedures.5 Furthermore, almost 76% of BDD patients visit a plastic surgeon to undergo cosmetic surgery, and more than half (60%) of patients with BDD undergo unneeded cosmetic surgery due to apparent imperfections.6,7 Most plastic surgeons (84%) reported that they had previously operated on a query BDD patient, and a vast majority (82%) of patients with BDD had poor results.8,9 Multiple previous studies have shown that patients with BDD usually have negative outcomes as well as dissatisfactions after the procedure.7,10 Consequently, it is vital to correctly identify BDD patients in any cosmetic surgery-related practices because the appropriate management for these individuals involves psychiatric evaluation rather than plastic surgery.11,12 The overall prevalence of patients with BDD among the general population is about 2.4%.13 However, among cosmetic-related practices, the prevalence of BDD is substantially higher, with a prevalence of 13% among patients pursuing plastic surgery clinics, 14% among patients in cosmetic dermatology, 6.9% in an oculoplastic surgery setting, and 10% in the maxillofacial clinic.14-17 The aforementioned prevalence of BDD in patients differ dramatically across practices, likely due to different patient populations and unpredictable screening approaches.10-13 Moreover, due to the uncommon and unusual screening of patients with BDD, there is usually an underdetection of patients with BDD.6,8,18 Body dysmorphic disorder patients who undergo cosmetic surgery usually consume the surgeon’s effort and time with multiple requests for multiple procedures and consultations. Moreover, patients with BDD are also more prone to consider lawsuits against their surgeons or even become physically violent.18-20 These major concerns emphasize the importance of accurately diagnosing patients with BDD attending cosmetic management. Cross-sectional studies are required to offer data on the prevalence of BDD in plastic surgery and oculoplastic surgery clinics. A better understanding of this condition in patients seeking facial and oculoplastic surgeries can decrease the economic burden on health care systems and help redirect patients with BDD to seek the care they need, particularly if it is psychiatric doctor rather than plastic surgeon. As psychological intervention by mental health professionals is an important treatment approach, it mainly focuses on altering negative thoughts and behavior through specific supported strategies. Different screening tools were identified in the literature for screening of BDD, including the Dysmorphic Concern Questionnaire (DCQ). This questionnaire contains 7 items that examine physical appearance concerns. It has been validated with good internal consistency (Cronbach’s alpha: 0.88).21 However, the sensitivity (72%) and specificity (90.7%) with a cut-off value of ≥14 (35) were much lower than the screening tool used in this study (Body Dysmorphic Disorder Questionnaire [BDDQ]), which has a sensitivity of 100% and specificity of 89-93%.22 Another available screening tool for BBD is the Body Dysmorphic Symptom Scale (BDSS); this screening tool is a self-reported 10-item questionnaire, focusing on patient physical appearance concerns. However, there is no specific accepted cut-off point for positive BDD screening in this questionnaire. Furthermore, it lacks validity.23 For these reasons, this was not the screening tool used in this study. Another available screening tool is the BDDQ-Dermatology Version (BDDQ-DV). However, as the name implies, has most commonly been used in dermatology clinics. Little is known about such a disorder in patients from Jeddah. This study aim at identifying the prevalence of positive screening for BDD among patients pursuing cosmetic surgeries in plastic surgery and oculoplastic surgery clinics, and the association between BDD and the desired cosmetic surgical procedure at King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia.
Methods
After obtaining ethical approval from the ethics committee, this cross-sectional study was distributed randomly between March 2019 and March 2020 among adult patients pursuing cosmetic surgery in plastic surgery and oculoplastic surgery practice at KAUH. All patients aged 18 years or older who arrived for a new consultation to pursue cosmetic surgery in plastic surgery and oculoplastic surgery clinics were included in the screening survey during the pre-consultation process. Participants with medical indications for surgery for example visually significant ptosis and recurrent infected chalazions were excluded from the study. The main reason for undergoing surgery in our participants was for cosmetic purposes.
Individuals who agreed to fill out the questionnaire were offered a self-administered questionnaire. Randomly selected medical students volunteered as data collectors, informed patients about the study, and asked for the consent. Patients completed the questionnaire in the waiting room. After completing the survey, patients proceeded to their respective clinic appointments. The total sample size was calculated as 376 while keeping the margin of error as 5%, confidence level as 95%, population size as 20,000, and response distribution as 50% by using raosoft sample size calculator.24 Participants completed a validated, anonymous, self-administered questionnaire.
Study variables
The questionnaire of this study had 3 main categories including: i) Sociodemographic (age, nationality, marital status, educational level, monthly household income, smoking status, comorbidities); ii) Previous oculoplastic/plastic surgery clinic visit; iii) most desired cosmetic surgical procedure; and iv) a validated and reliable questionnaire (such as BDDQ).
The BDDQ
The questionnaire used in this study was the BDDQ due to its high sensitivity (100%) and specificity (89-93%) for BDD screening in cosmetics clinics; also, it also showed good validity.25 The BDDQ was the primary survey used to identify patients who exhibited symptoms consistent with BDD. The BDDQ is a validated, brief, self-administered questionnaire that has been extracted from DSM-V diagnostic criteria for BDD developed by Pillips.26 It uses close-ended variables and asks the participants whether their general concerns about appearance are a source of preoccupation. Consequently, it also assesses the grade to which these concerns cause distress or interfere with the person’s social or work-related functions. The survey was originally developed among psychiatric patients, but since then it has been validated in a number of different patients, including facial plastic and oculoplastic surgery patient population. Among the plastic surgery and oculoplastic surgery patient population, the survey was established as having a high sensitivity (100%) and high specificity (90.3%).27 The English version of the BDDQ was translated by an expert bilingual and tested for validity, which showed reasonable internal consistency (Cronbach’s α = 0.659). Body dysmorphic disorder was diagnosed according to the DSM-V criteria. The scores were calculated in Table 1.
Scoring of body dysmorphic disorder questionnaire (BDDQ).
The severity scale of BDD was used from 0 to 4 (0 = level 0, 1 = level 1, 2 = level 2, 3 = level 3, 4 = level 4). A score of 4 was regarded as BDD. A score of 0 to 3 was considered negative for BDD. The reliability of the BDD score measurement was calculated using Cronbach’s alpha. An alpha value of 0.758 was observed, which indicated an acceptable reliability (Table 2).
Reliability of the body dysmorphic disorder questionnaire (BDDQ).
Furthermore, it is worth noting that BDDQ is not a diagnostic tool. It is a screening tool and a patient who screen positive is a possible case of BDD. A mental health specialist has to confirm the case.
Ethical considerations
This study was carried out after receiving ethical approval from the research ethics committee of King Abdulaziz University, Jeddah, Saudi Arabia. The contribution of patients in this study was entirely on a voluntary basis. Prior to participation in the research, written informed consent was obtained from all patients.
Statistical analysis
Data were checked for completeness and correctness. Categorical data were presented as frequencies and percentages, and continuous data were presented as mean ± standard deviation. An alpha value of 0.758 was observed, which indicated acceptable reliability. Prevalence rate for all cases and different subgroups were calculated. The age of the respondents were normally distributed according to Shapiro Wilk test. Age was compared between BDD cases and non BDD cases; clinic visit (plastic and reconstructive surgery versus oculoplastic surgery) by independent samples t-test. The rest of the variables were categorical and were compared between the above-mentioned subgroups by Chi-square test. A binary logistic regression was carried out to identify the factors responsible for the development of BDD. The analysis was carried out in 95% confidence interval using the Statistical Package for Social Sciences, version 24.0 (IBM, Armonk, N.Y., USA).
Results
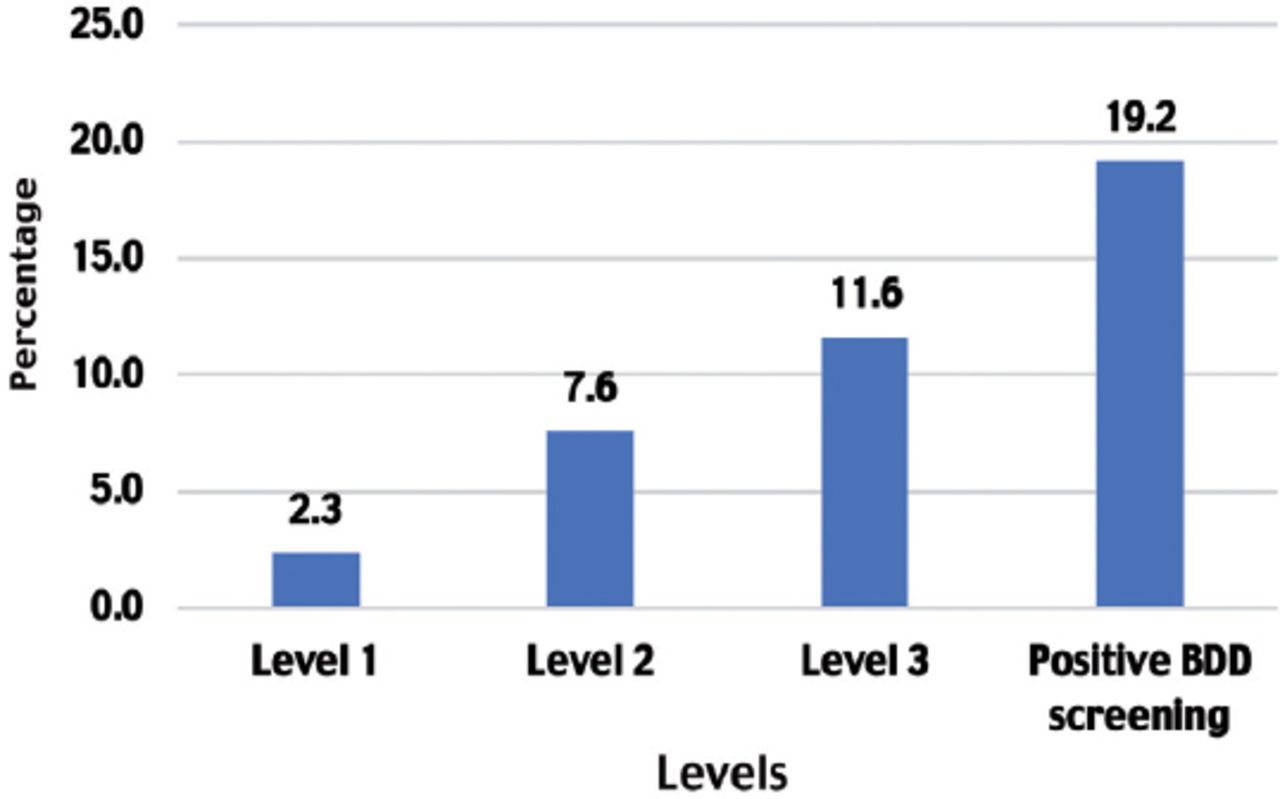
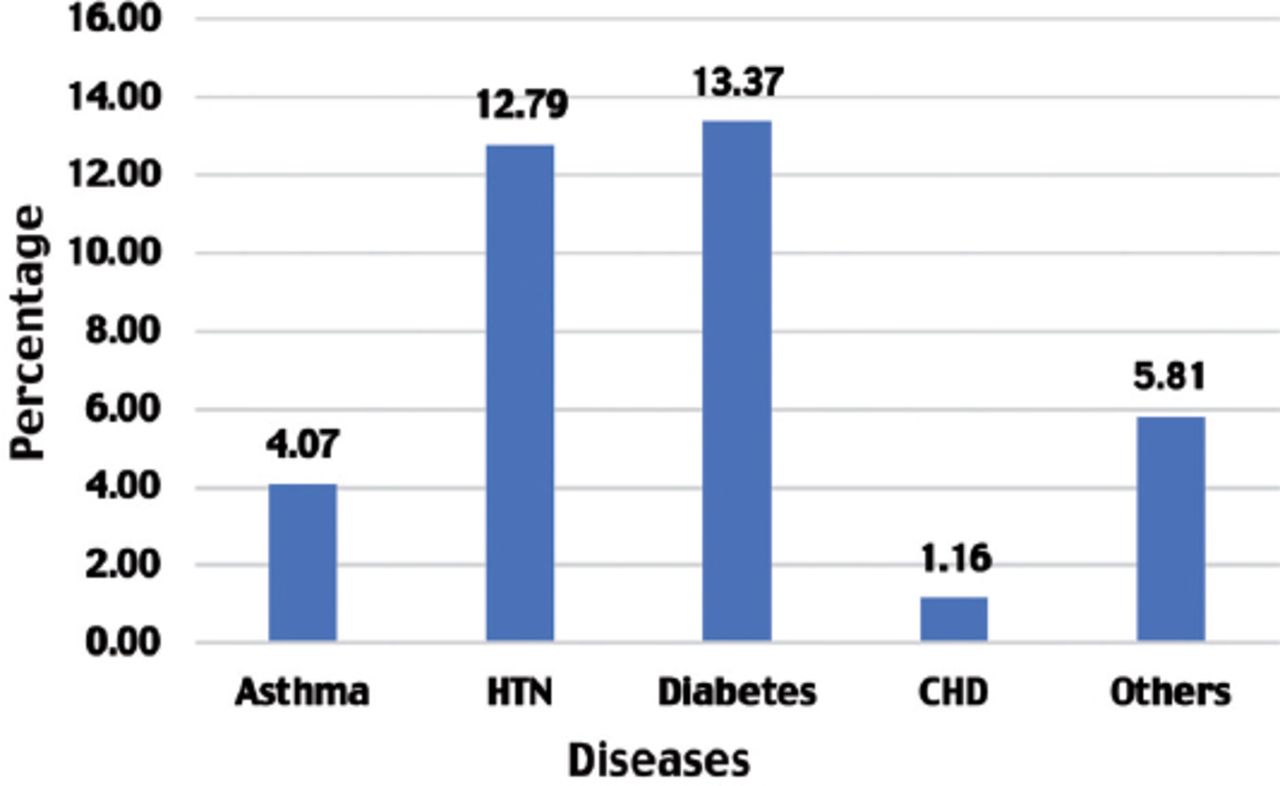
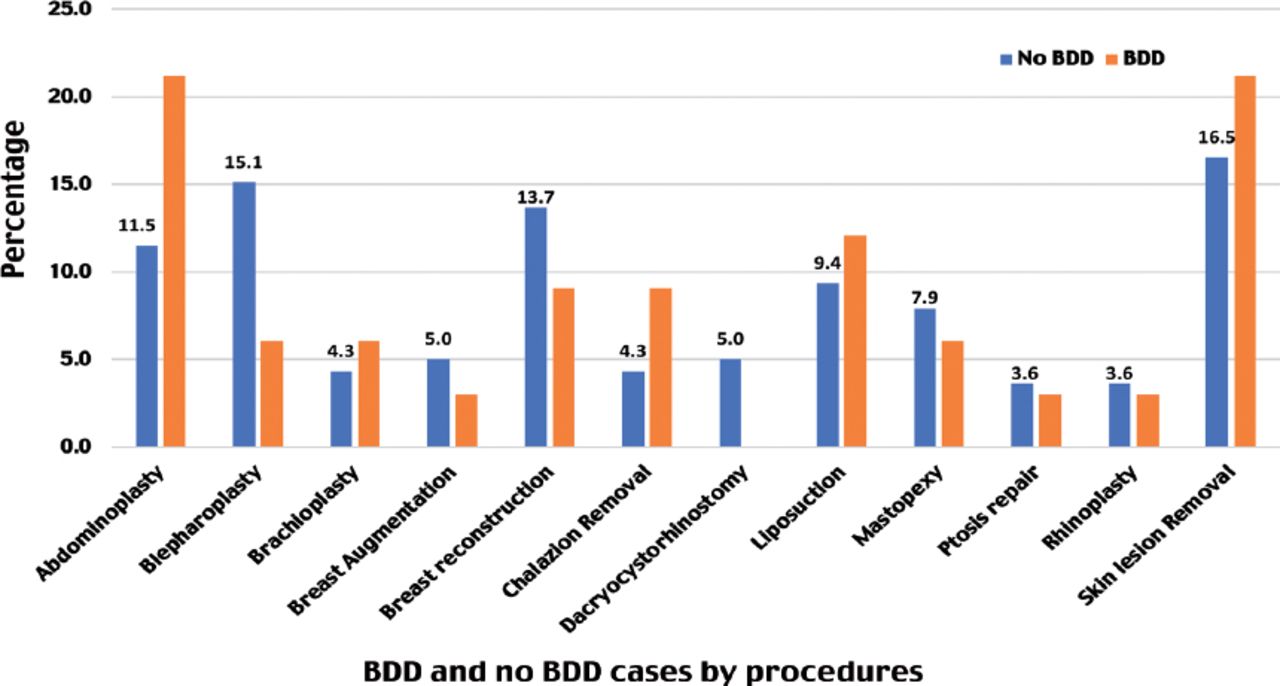
A total of 344 cases were included in this cross-sectional study, and 66 of them had BDD (prevalence rate of 19.2%). The prevalence of BDD among occuloplasty clinic visitors (13.3%) was lower than plastic and reconstructive surgery clinic visitors (21.3%) (Table 3). The majority, 278 cases, did not have BDD, but they had level 1 to 3 BDD as presented in Figure 1. The prevalence of chronic disease was 33.72% among all cases and the most common chronic disease was diabetes mellitus, present in 13.37% cases (Figure 2). All included cases underwent plastic and reconstructive surgery or oculoplastic surgery. The most popular surgeries underwent or will be undergone by the BDD cases were abdominoplasty (21.2%), and skin lesion removal (21.2%). The most popular surgery among the non-BDD cases were skin lesion removal (16.5%), and blepharoplasty (15.1%) (Figure 3).
Prevalence of body dysmorphic disorder among all cases.
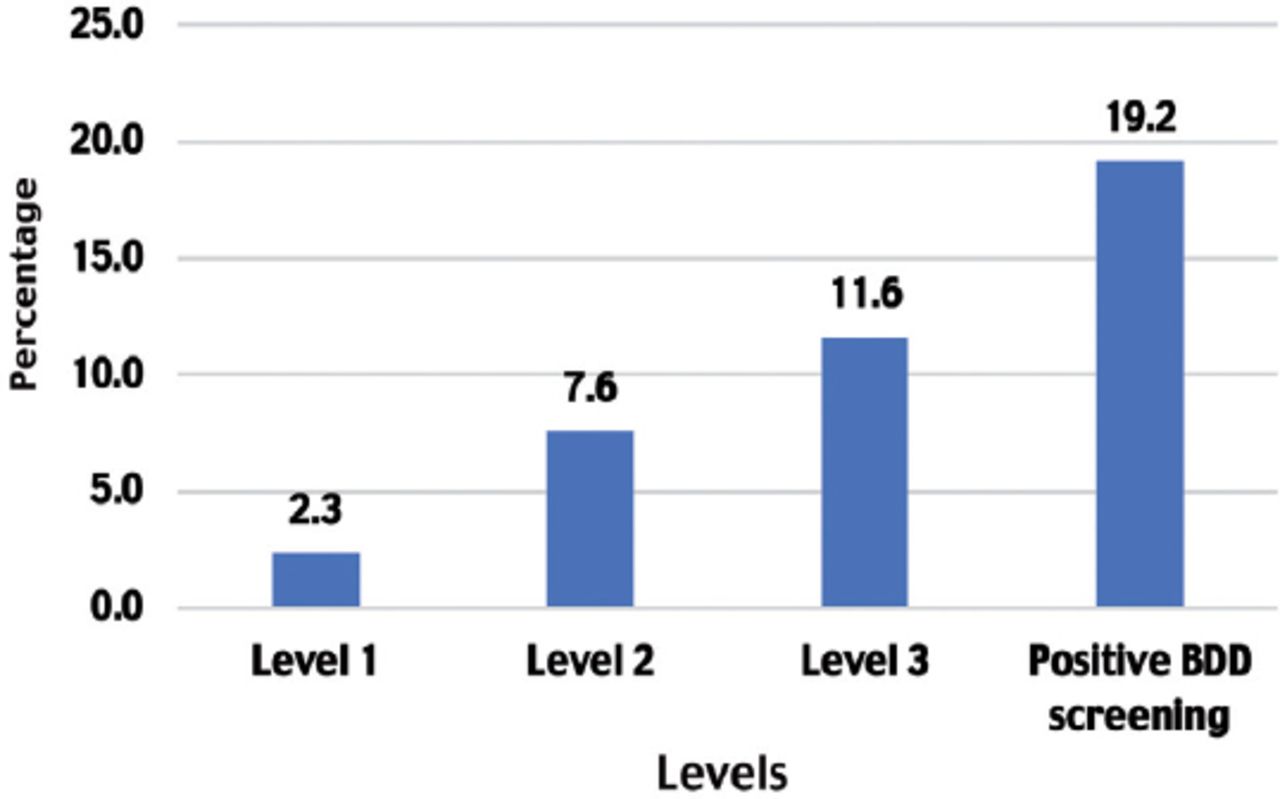
Body dysmorphic disorder questionnaire levels. BDD: body dysmorphic disorder
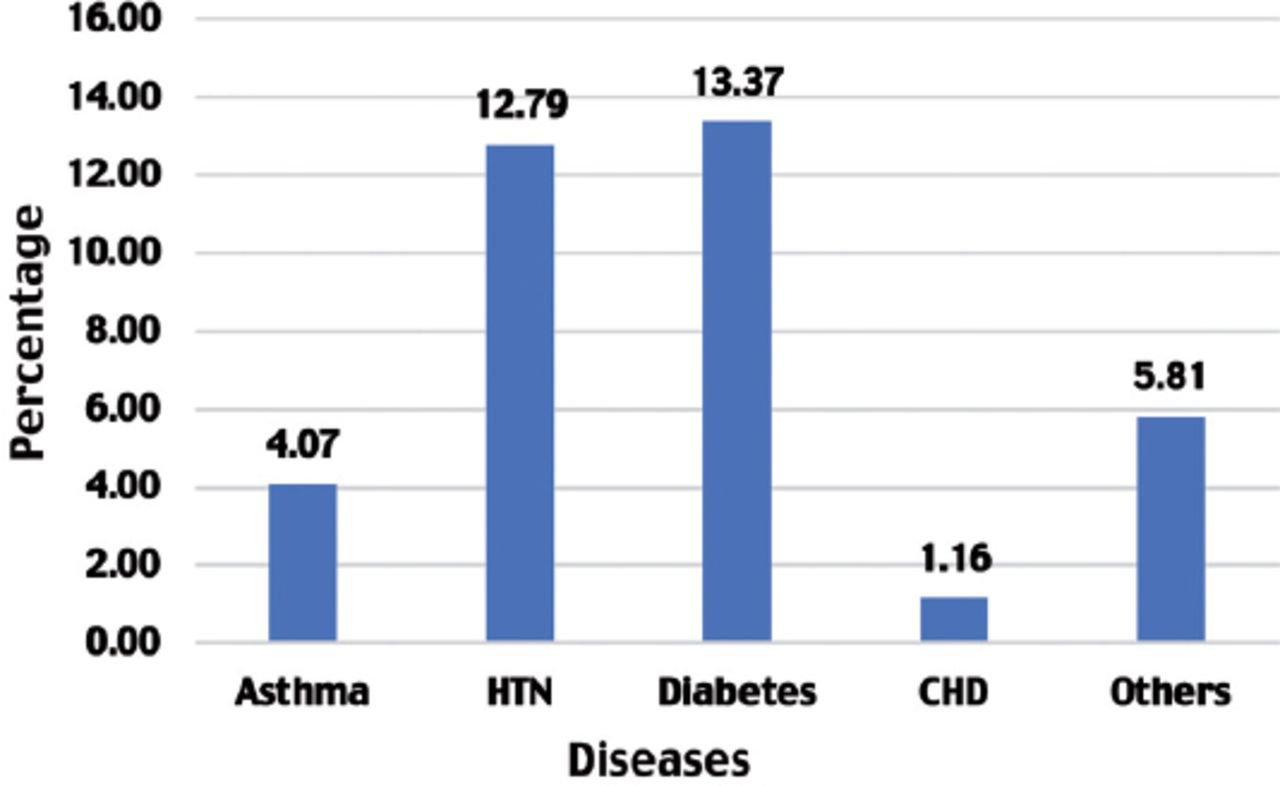
Prevalence of chronic disease among all cases. CHD: coronary heart disease, HTN: hypertension

Distribution of body dysmorphic disorder (BDD) and no BBD cases by procedure about to undergo/ have undergone /consult the doctor about.
The mean age of all cases was 39.66 ± 13.76 years. Age distribution between BDD cases and non-BDD cases was not statistically significantly different, p=0.260. A considerably higher percentage of females (93.9%) had BDD compared to males (6.1%), (OR=0.343, p=0.040). Smoking was found to be significantly associated with BDD, 21.2% of smokers had it, p=0.010. The prevalence of BDD among those who had previous surgery was staggering, 60.6%, p=0.002. However, nationality, marital status, education level, monthly household income, and city of residence was not significantly associated with BDD (all p-values of >0.050). Among all cases, 254 (73.8%) were visiting plastic and reconstructive surgery clinic, and the remaining 90 (26.2%) cases were visiting oculoplastic surgery clinic. These 2 groups were compared in terms of all socio-demographic characteristics. The important observations were as follows: both clinics were predominantly visited by female cases but slightly higher percentage of females visited oculoplastic surgery clinic (93.3%) compared to plastic and reconstructive surgery clinic, (OR=2.774, p=0.020). Almost half of the plastic and reconstructive surgery visitors had previous oculoplastic/plastic surgery clinic visit, 126 (49.6%) whereas only 24 (26.7%) of the oculoplastic surgery clinic visitors had previous oculoplastic/plastic surgery clinic visit, (OR=2.707, p<0.001). It was also observed that, higher percentage (60.6%) BDD cases previously visited oculoplastic/plastic surgery clinic compared to non-BDD cases (39.6%) (p=0.002). The other studied socio-demographic variables were not significantly different between 2 clinic visitors (all p-values of >0.050) (Table 4).
Association between BDD (yes/ no) and sociodemographic variables; clinic type and sociodemographic variables.
The percentage of cases underwent specific breast- related procedures and face-related procedures were as follows: i) mastopexy 7.6%, breast augmentation 4.7%, breast reconstruction 12.8%; ii) blepharoplasty 13.4%, ptosis repair 3.5%, rhinoplasty 3.5%, chalazion removal 5.2%, and dacrocystorhinoplasty 4.1%. None of these specific surgeries were associated with positive BDD (p>0.050) (Table 5). A binary logistic regression was performed to find out the factors collectively predictive of developing BDD. Variables included in the regression analysis were clinical type, age, nationality, gender, marital status, education level, income, smoking, and history of previous surgery. The analysis showed that the age (OR=0.943, p<0.001) and marital status - single (OR=0.076, p=0.002) were the significant predictors of the model (Table 6).
Relationship between specific breast related procedure, facial procedure and positive body dysmorphic disorder (BDD).
Binary logistic regression analysis to identify the factors responsible for developing body dysmorphic disorder (BDD).
Discussion
Plastic surgeries are often sought by individuals with BDD. This is consistent with the intense surge in the last decade of cosmetic surgical procedures in the United States, Germany, England, and Brazil.28-31 However, studies show that most of these patients have a poor level of satisfaction after surgery and very little benefit.27,32 Body dysmorphic disorder is considered to be a relative contraindication for undergoing plastic surgery; however, routine screening in practice is not common. This could be attributed to clinicians’ underestimation of BDD prevalence and a lack of knowledge of available validated screening tools.27 In our study, the prevalence of patients with positive screening for BDD was 19.2%. This is in contrast to another study conducted in the United States, where the prevalence was 9.7%.33 This discrepancy might be explained by the fact that their study population included a smaller number of female patients compared to our study. Furthermore, in our study, we found that 93% of female subjects screened positive for BDD. This is consistent with another study by Ishigooka et al,19 who found a clear relationship between body image and identity in females compared to males. Moreover, it was found by Salehahmadi et al33 that education levels were the most important influential factor in undergoing plastic surgery followed by age and gender. This agrees with our results, since more than half (54.4%) of the participants who screened positive for BDD in our study population had a bachelor’s degree. Of the positively screened participants in our study, 72.7% were non-smokers; this is in contrast to another study conducted in the United States,34 where they found a relationship between perceptions of physical appearance and smoking. They suggested that female smokers are more likely to evaluate both their physical health and appearance negatively. This discrepancy could be due to the higher number of female smokers in the United States (12%),35 compared to Saudi Arabia (9%).36 Interestingly, we found a statistically significant difference between the prevalence of BDD and recurrent visits to oculoplastic/plastic surgery clinics as 60.6% of participants with a positive BDD screening test reported having at least one previous visit to the clinic. This is consistent with the findings of Joseph et al,27 who concluded that most BDD patients were unhappy with the outcome of their surgeries,31 which results in recurrent visits and appointments to clinics, seeking further opinions and possible unnecessary cosmetic surgeries. In our study, chronic chalazion removal had the highest association with BDD in the oculoplastic clinic (9.1%), as most of the patients screened positive for BDD reported being inpatient for the conservative methods used for treating such conditions. The second highest association with BDD in the oculoplastic clinic was blepharoplasty (6.1%), which is carried out to alter either the natural anatomy or age-related changes. On the other hand, we found that in plastic surgery clinics, abdominoplasty and skin lesion removal had the highest associations with BDD (both, 21.2%) followed by liposuction (12.1%). These patients reported being inpatient for seeking the desired body shapes with conservative methods such as diet and exercise. They reported being self-isolated and ashamed with suicidal thoughts. In recent years, with an increasing prevalence of obesity (35.6%),37 and sedentary lifestyles in Saudi Arabia, an increase in the number of BDD patients seeking such surgeries after massive weight loss is expected.
In Saudi Arabia, there are several studies that were conducted on the prevalence of BDD. The first study by AlShahwan,38 concluded that BDD was common among female patients seeking dermatology clinics at King Khalid University hospital. Another study by Kattan et al,39 discovered that cosmetic treatment providers were actually knowledgeable about BDD. In addition, a study that was carried out in Al Ahsa reported the prevalence of BDD among individuals undergoing facial plastic surgery was 14.19%.40
Study limitations
Although our sample size was reasonable, and the study objectives were accomplished, this study has a number of limitations. First, this research was performed among patients in a single center; therefore, there is a limitation in the generalizability of the findings. Second, our research was cross-sectional, which covers a limited period of time. Consequently, the study population may have not represented the entire population in Saudi Arabia. We recommend future studies that include different institutes from different regions in Saudi Arabia. In addition, we recommend establishing a routine BDD screening tool in oculoplastic/plastic surgery clinics prior to undergoing any procedures. For health professionals who cannot screen with a tool such as the BDDQ, they can ask appearance specific questions. For example, “does your appearance worry you?” “Do you spend much time worrying about your appearance?”
If a procedure is to be performed, patients should be informed of the possibility of little benefit and poor satisfaction postoperatively. It is recommended for physicians not to make a decision to operate based on patient preference alone, and to prioritize clinical judgment. We recommend future randomized control trial studies to identify high risk groups for BDD. Lastly, we also recommend referring patients with positive BDD screening to psychiatrists for proper evaluation and management.
In conclusion, BDD is most likely an undetected mental health issue among our patients pursuing cosmetic surgeries in plastic surgery and oculoplastic surgery clinics and a potential source of post-operative patient dissatisfaction. Cosmetic surgeons should consider screening their patients as a standard protocol to guarantee the best outcomes.
Acknowledgment
The authors gratefully Editage (www.editage.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 13, 2020.
- Accepted August 29, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.