


Pregnant women are at an elevated possibility of getting COVID-19 infection because of the functional changes in their immunology and physiology. Earlier findings have suggested that if pregnant women get infected by Severe Acute Respiratory Syndrome (SARS), they pose a major risk of restricted fetal growth, premature labor, and unprompted miscarriages.
In a current study, it has been stated that there is a considerable effect on the coagulation, respiratory, immune, and cardiovascular functions in pregnant women due to physiological variations and this may highly affect the COVID-19 progression in them positively or negatively.1 To date, pregnant women who were ill by COVID-19 have shown few neonatal and maternal problems.2 The effects of COVID-19 in pregnancy needs to be ascertained.
The aim of this review is that since pregnant women are at an elevated risk of getting COVID-19 infection, the present review deals with the specific etiological characteristics of COVID-19, its indications and prognosis, causes of pregnant women’s vulnerability, its consequences on fetuses, preventative measures in pregnancy, precautionary neonatal attention, and an understanding of the selection of medications for clinically treating COVID-19 and for managing it in pregnancy to safeguard the life and health of pregnant women and neonates in this grave pandemic.
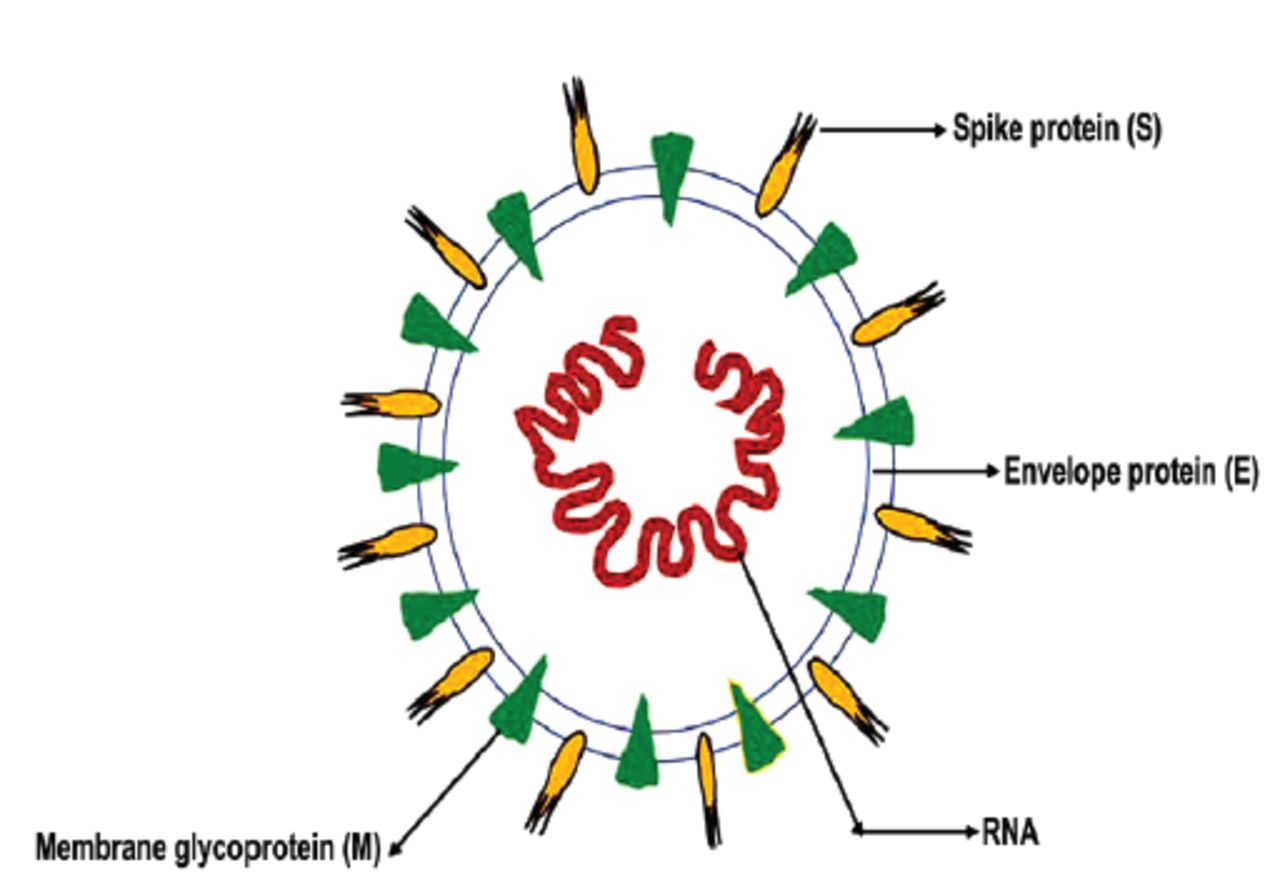
COVID-19 has only one ribonucleic acid (RNA) strand, which is an enveloped, non segmental virus. It can survive on both humans and animals; hence, they are zoonotic. The capsule of coronavirus is composed of a bilayer of lipid and transmembrane proteins. The outer side of the covering looks like a crown under the electron microscope because of spike-like projections. It has a positive strand RNA and capsid protein with helically symmetric composition that forms its nucleocapsid. Its genome size is 26-32 kb, and its arrangement is preserved, such as protein-membrane (M), protein-envelope (E), replicase-spike (S), and nucleocapsid protein (N). For the purpose of coding for replication enzymes, approximately 67% of the genome is utilized, and the remaining portion is consumed for coding structural and helper proteins3,4 as depicted in Figure 1.
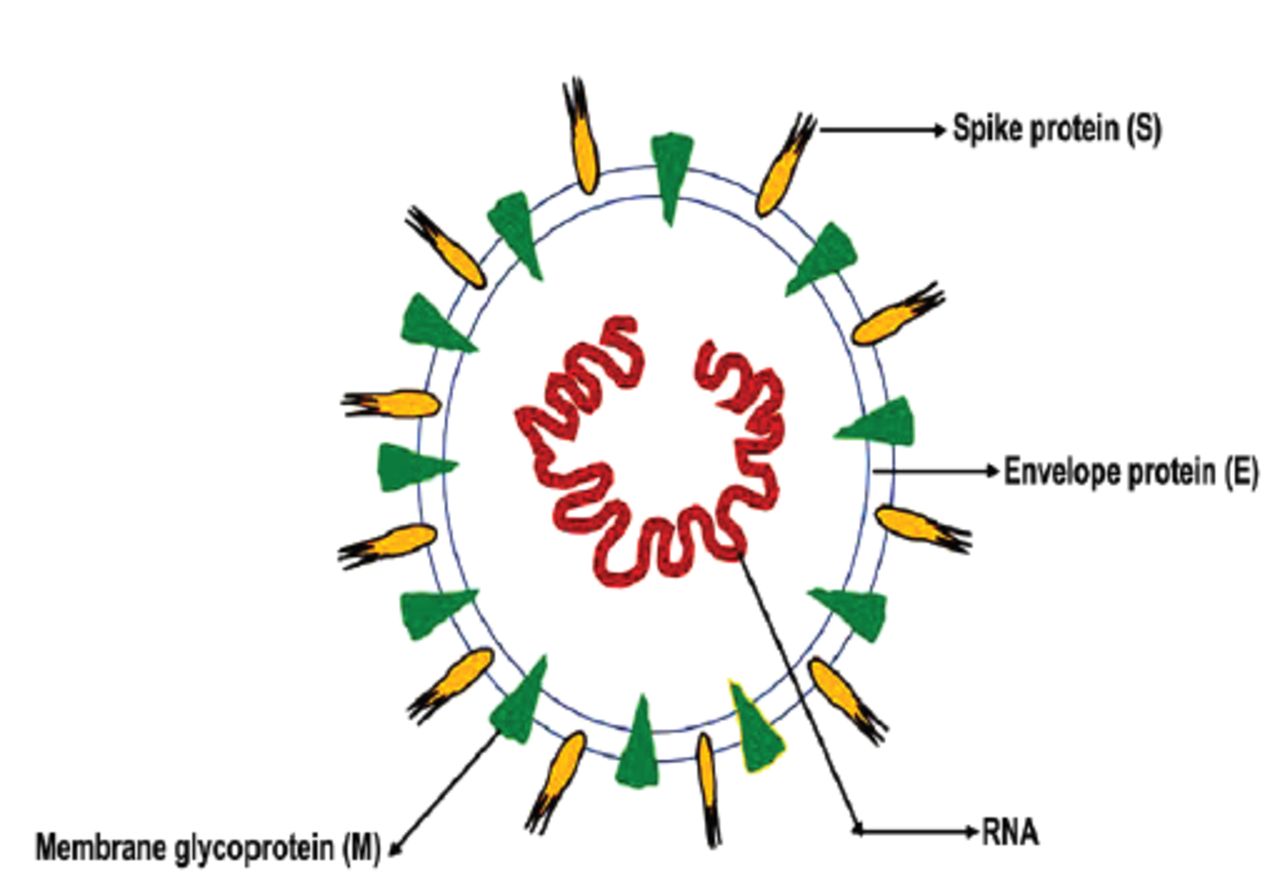
- Structure of COVID-19. RNA: ribonucleic acid
There are 7 forms of coronavirus that can infect human beings.5 Among them, Middle East Respiratory Syndrome, SARS, and COVID-19 are deadly pathogens. They are spread mainly by human-to-human contact.6 The principal source of transmission is respiratory droplets released by coughing or sneezing, which are deposited in the surrounding areas. There are good chances of transmission of infection to persons who come in 6 feet of the infected patient. It is necessary to regularly clean surfaces and objects which have come into contact with an infected person since COVID-19 can remain alive on surfaces that are nonliving. Hence, prevention is most crucial to avoid COVID-19 from multiplying further.
Within 2 to 14 days of exposure to COVID-19, different types of symptoms start appearing, such as cough, sore throat, running nose, headache, chest pain, fever and difficulty breathing. Severe symptoms such as liver, heart, and kidney injury are also reported.7 The severity of infectivity might be reliant on the health of the individual. If a person has preexisting health problems like abnormal blood pressure, lung illnesses and diabetes, the infection might be more severe. Elderly people are at greater risk of COVID-19 infection. For the identification of virus-causing respiratory diseases and for the prognosis of COVID-19, computed tomography (CT) scans and reverse transcription polymerase chain reaction (RT-PCR) tests are carried out.4,8 Viral isolates are utilized as prime substrates for doing an assay that detects a particular virus and sequencing the gene in the RT-PCR method. In comparison to RT-PCR, a CT scan is more accurate and could be utilized to gather more information after a confirmed RT-PCR test.4 A specimen of saliva, throat swabs, stool, and urine were utilized to perform the RT-PCR test. In a sole patient, nucleic acid tests are performed repeatedly to obtain a precise outcome. In the case of a specimen of throat swabs, if the virus is not detected, tests are carried out twice, one after another, at an interval of one day. For the purpose of diagnosis, a serological test might also be performed when there is no facility available to perform an RT-PCR.7
For efficient management, pregnant women ill with COVID-19 must be kept in isolation and then transferred to a well-equipped hospital with adequate health amenities and expert heath care workers. After the checkup, the pregnant woman is sorted as having mild illness, which means symptomatic having steady essential symptoms; severe illness, which means frequency of respiration is greater than or equal to 30 per minute and oxygen concentration is less than or equal to 300 mm Hg; or critical illness, which means mechanical ventilator is essential because of respiratory failure and shock associated with organ collapse.7,8
During pregnancy, preventative methods should be adopted, such as avoiding unnecessary outdoor work, community get-togethers and handshaking, hand wash, practicing social distancing, and wearing protective face masks. Pregnant women must regularly observe their vital symptoms like breathing, pulse rate, fever and must update their care providers on their health status on a consistent basis. They should also carefully follow any advice given to them by their care provider.7 Pregnant women should examine their body temperature frequently and should consult a physician right away if they suffer any health problems like fever, difficulties in breathing, or the common cold.9 They should make the necessary preparations for delivery and provisions to reach the hospital safely and on time. Even in the current ongoing pandemic, it is safe to give birth to a child in a hospital. Additionally, if they recently have traveled or exhibit COVID-19 symptoms, they should be quarantined for 2 weeks. As per the Chinese National Health Commission, suspect or lab-confirmed neonates must be put under watch and not breastfed.9 Moreover, there are no cases of transmission of COVID-19 via mother’s milk.
COVID-19 is highly infectious. Therefore, there is an elevated probability of infection in neonates during pregnancy. COVID-19 has an awful effect on the health of neonates, instigating difficulty in breathing, gastrointestinal problems, and higher pulse rates. However, vertical transmission, for example, infection to infants from mothers before and after birth through blood of placenta and germ cells, has not been reported.12 Based on a review study conducted in China, 9 pregnant women ill with COVID-19 gave birth to 10 neonates, but no vertical transmission in neonates has been reported.3 In a recent study, Dong et al10 states that there are chances of vertical transmission by intrauterine route. The report indicates that 2 neonates got COVID-19 postpartum from their mothers who got infected by COVID-19.11 To minimize the vertical transmission risk, delay cord clamping is not advised. Also, closer contact among the baby and mother is not recommended.12 Furthermore, neonates must be isolated for 2 weeks as a preventive measure.
For preventing COVID-19, different types of vaccines are available, such as Comirnaty (BNT162b2) by Pfizer–BioNTech, Moderna COVID-19 vaccine (mRNA-1273) by Moderna, Sputnik V by Gamaleya, Covishield by Oxford-AstraZeneca, Covaxin by Bharat Biotech, and ICMR and COVID-19 vaccine Janssen (JNJ-78436735; Ad26.COV2.S).13 Various clinical trials are ongoing to investigate different potential therapies, for example monoclonal antibodies.
For treating COVID-19, only Remdesivir medicine is authorized by the United States Food and Drug Administration (USFDA) and it is being used on hospitalized patients who are given supplemental oxygen treatment.14 Doctors must select existing medicines based on their previous experience regarding antiviral or host targeted therapeutics or direct-acting antiviral drugs. In a few cases, there is an improvement with antiviral therapy with ritonavir-100 mg and lopinavir-400 mg twice in a day plus α-interferon (for the purpose of injection, in 2 ml sterile water, there should be 5 million IU) in clinical settings.7
The chances of secondary illness instigated by bacteria is increased due to injury to alveola caused by COVID-19. Ceftriaxone is given intravenously in cases of secondary illness triggered by bacteria. Corticosteroids are used in treatment if supplemental oxygen is required, and 40 mg prednisolone is recommended once in a day orally. In case where it is difficult to give medicine orally, 80 mg hydrocortisone is given twice a day intravenously.15 Methylprednisolone might be administered to seriously ill hypoxic patients.7
The World Health Organization (WHO) has recommended not to give COVID-19 vaccines to pregnant women except in case of higher risk of them getting COVID-19. American College of Obstetricians and Gynecologists (ACOG) has recommended that COVID-19 vaccines must be given to pregnant women and maintained that it should be given to lactating women like other women. Both ACOG as well as Society for Maternal-Fetal Medicine (SMFM) emphasize that both the vaccines Pfizer-BioNtech (BNT162b2) and Moderna mRNA-1273 approved by USFDA must be provided to pregnant women who are willing to have it. The International Federation of Gynecology and Obstetrics maintains that COVID-19 vaccines must be given to pregnant and lactating women.
To avert COVID-19 proliferation, preventative anti-viral practices should be adopted. Good personal hygiene should be practiced. There should be preliminarily screening at every entrance in hospitals. Prioritized attention and special care must be given to all pregnant women. Doctors and nurses must wear N-95 masks, disposable gloves, specialized glasses for eye protection, and personal protective equipment kits and must practice standard procedures.
All nations must collaborate to drive down the ongoing pandemic. Researchers and doctors must share important information regarding COVID-19 and should adopt effective measures to diminish the multiplying of COVID-19, specifically in regions with limited medical facilities. For the purpose of notifying every substantial fetal and maternal data regarding pregnant women having COVID-19, a surveillance system must be installed.
Acknowledgment
The authors would like to express their gratitude to King Khalid University, Abha, Kingdom of Saudi Arabia for providing administrative and technical support and also thankful to the Deanship of Scientific Research, King Khalid University. The authors also acknowledge Scribendi (www.screbendi.com) for English language editing.
Footnotes
Disclosure.
Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 25, 2021.
- Accepted April 19, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.