


Abstract
Objectives: To assess the sex hormone levels in young Saudi female migraineurs during a migraine attack and during pain-free periods and compare them with control subjects.
Methods: A case-control study involving 14 Saudi female migraineurs and 21 control subjects was conducted between December 2019 and March 2020. Demographic and disease history data were collected through participant interviews. Blood samples were drawn during the migraine attack and pain-free periods.
Results: Follicular (30.00±19.60; p<0.001) and luteal (39.79±11.45; p=0.037) estrogen levels were significantly higher in patients with non-menstrual related migraine (NMM), while luteal testosterone levels (1.10±0.31; p=0.023) were significantly higher in patients with menstrually related migraine (MM). Body mass index (BMI) was higher in patients with NMM (25.77±6.53; p=0.013), and it was found to be associated with follicular estrogen (p=0.016), progesterone (p=0.018), and pain intensity (p=0.042). Luteal estrogen level was significantly lower (13.96±7.88; p=0.036) in patients with luteal onset of attack.
Conclusion: High estrogen levels were found to mediate NMM, their effect being more pronounced with increase in BMI; whereas low luteal estrogen levels mediated MM. Young females with MM might have high luteal testosterone levels, and a compensatory protective role could be surmised accordingly.
Migraine is a debilitating disease manifested by recurrent headache attacks and associated symptoms.1 Migraine commonly affects individuals between the ages of 18-44 years and is more common in females than in males.2 A recent epidemiological survey in the Kingdom of Saudi Arabia (KSA) reported the overall prevalence of migraine as 26.97%, with the incidence in females being 3 times as high as that in males.3 Migraine is classified into 2 main types: migraine without an aura and migraine with an aura. The aura is a neurological symptom that precedes the headache attack.4 Migraine in females can be classified into menstrual migraine, menstrually related migraine (MM), and non-menstrual migraine (NMM). These types are defined in the International classification of headache disorders, 3rd edition (ICHD-3).5
Some reports have postulated the role of sex hormones in the pathophysiology of migraine. This notion emerged due to the higher prevalence of migraine in females than in males. Furthermore, the rate of incidence of this disease changes throughout the female life. While migraine prevalence is identical in male and female children, the incidence rises rapidly after puberty in females, reaching approximately 2-3 times than seen in males. The course of the disease also changes during pregnancy, perimenopausal, and menopausal periods.6 Therefore, some studies have estimated the level of sex hormones in migraineurs, particularly females. Estrogen is the most studied hormone in this regard, and multiple theories have been postulated correlating estrogen to the pathophysiology of migraine.7 However, there is still a lack of consensus regarding the role of estrogen in migraine pathology, and this could be attributed to the multiple mechanisms involved in the disease pathophysiology as well as the presence of diverse sub-classes. Progesterone and testosterone are less investigated in this regard, but few available data propose a protective effect of these hormones in some cases.8
Therefore, in the present study we aimed to explore the possible association between sex hormones and migraine attacks in Saudi females. We planned to compare the serum levels of sex hormones, including estrogen, progesterone, and testosterone, between Saudi female migraineurs and healthy controls. The hormone levels were assessed on 2 occasions; once during the attack and once during an attack-free period.
Methods
This case-control study was carried out in the Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University (IAU), Dammam, Saudi Arabia. A total of 35 Saudi females (14 migraineurs and 21 controls) aged 18-30 years (mean age 21.91±2.78 years) were recruited by convenience sampling during the period from December 2019 to March 2020.
The target sample size was evaluated using G-power 3.1 software and the following values: power of the test (1-β) = 80%, type I error (α) = 5%, mean luteal estradiol level in female migraineurs = 127.71±59.9 pg/mL, and mean luteal estradiol level in normal controls = 189.26±42.21 pg/mL.9 Finally, the sample size calculation revealed the need for 11 subjects per group.
The participants were selected according to the following criteria: a young female (18-35 years) with a regular menstrual cycle who had a migraine diagnosed by a neurologist and fulfilled the ICHD-3 criteria for the same.5 We excluded those females who had undiagnosed headache, had disorders affecting sex hormones, were lactating or pregnant, or were on hormonal contraceptives.
All participants signed an informed written consent for participation in the study. The study followed the principles of Helsinki Declaration and received approval from the Institutional Review Board of IAU (IRB-UGS-2019-01-293). The participants were screened using the ICHD-3 diagnostic tool. Then the eligible candidates were asked to fill a data to collect information on demographic data such as age, body weight, height, and body mass index (BMI). It also included migraine-related questions such as type of migraine, onset of the disease, relation to menstruation, duration, number of attacks per month, severity of the attacks, family history of the disease, and triggers of pain. The migraineurs were divided into 2 groups: MM group, wherein the migraine attacks occurred during last 2 luteal days to day 2 or 3 of menstruation in at least 2 out of 3 menstrual cycles, but could also occur during other periods of the cycle, and the NMM group, wherein the attacks did not meet the MM criteria.5
The first blood samples were drawn when the participants visited during a migraine attack. At this time, they were asked to indicate the severity of pain using a visual analogue scale (score: 1-10) and mention the day of the menstrual cycle. The second blood samples were collected from the patients when they were in a pain-free period and in the opposite menstrual cycle phase compared to that during the first blood collection, that is, each migraineur had one follicular (day 1-10) and one luteal phase (day 18-27) blood sample. Similarly, 2 blood samples were collected from the controls during follicular and luteal phases. The migraineurs were also classified according to the onset of the actual attack into follicular or luteal actual onset of migraine pain.
Serum levels of estrogen, progesterone, and testosterone were estimated on 2 occasions (follicular and luteal samples). The analyses were performed using the following enzyme-linked immunosorbent assay kits: AccuDiag™ Estradiol, AccuDiag™ Progesterone, and AccuDiag™ Testosterone (Diagnostic Automation & Controls Private Limited, Calabasas, California 91302 USA) at the Institute for research and medical consultations, IAU, according to the manufacturers’ instructions, and readings were obtained with a Synergy Neo2 Hybrid Multi-Mode Reader (BioTek, Germany). All analyses were conducted in duplicate.
Statistical analysis
Data was analyzed using the Statistical Package for Social Sciences (SPSS) statistics for Windows, version 21 (IBM Corp., Armonk, NY, USA). The data was compared between the control subjects and migraineurs using an independent-sample student’s t-test. Analysis of variance (ANOVA) and least significant difference (LSD) post hoc tests were used to compare the hormonal levels in the luteal and follicular phases among the following groups: MM, NMM, and controls. The hormone levels were further compared between the groups of follicular and the luteal actual onset of migraine pain using an independent-sample student’s t-test. Correlation of hormone levels to the migraine features were performed using a Pearson correlation analysis. A p-value<0.05 was considered significant.
Prior related research was obtained from the PubMed database using the following key words: migraine and sex hormones, estrogen, progesterone, testosterone, menstruation.
Results
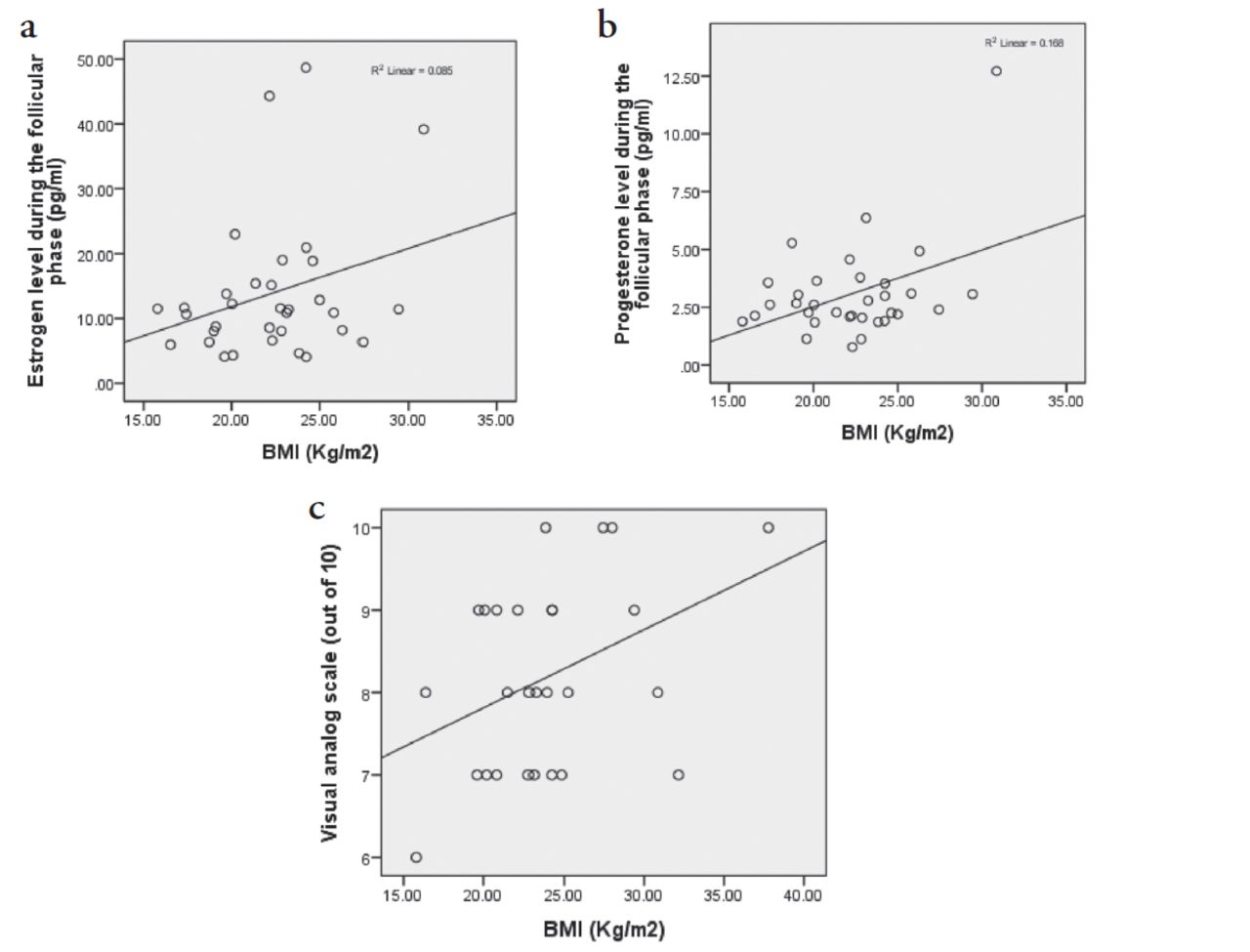
The general characteristics and hormonal levels were compared between the controls and migraineurs, and no significant difference was found in any of the tested variables (data are not shown). Then the same parameters were compared between MM, NMM, and control subjects using ANOVA and LSD post hoc test; the results are presented in Table 1. Body mass index was found to be significantly correlated with follicular estrogen (p=0.016) and progesterone levels (p=0.018) and the visual score of migraine intensity (p=0.042), (Figure 1).
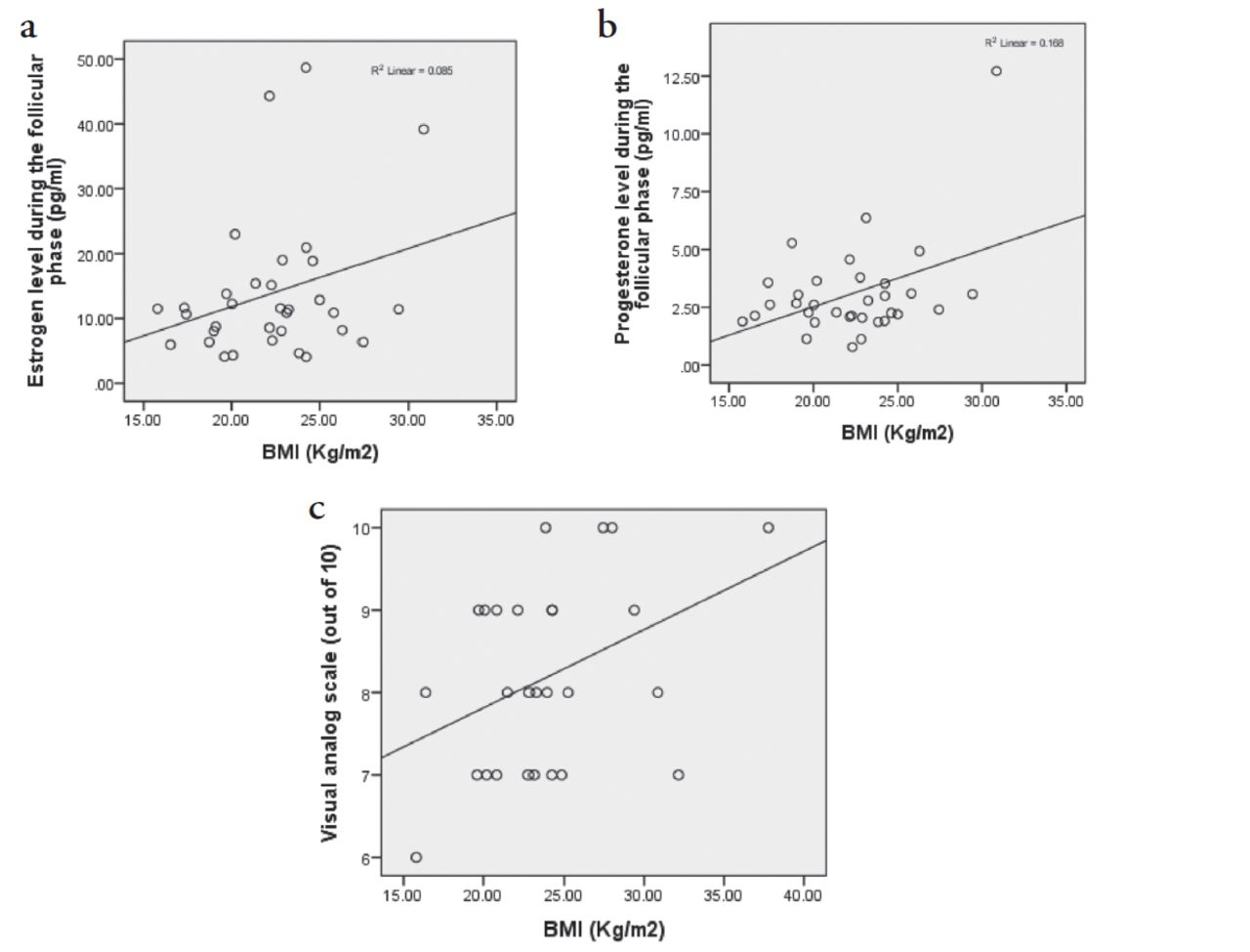
- Linear regression lines demonstrating the correlation of BMI with (a) estrogen during the follicular phase, (b) progesterone during the follicular phase, and (c) Migraine pain intensity by the visual analog scale.
- Comparison of the general characteristics and the hormonal levels between the migraineurs of MM, NMM migraine types and the controls during the follicular and luteal phases using ANOVA and LSD post hoc test.
The comparison of the hormonal levels between the groups of follicular versus luteal migraine onset is shown in Table 2.
- Comparison of the sex hormone levels during the actual attacks of follicular versus luteal onset. (using independent samples student t-test).
Discussion
The current study aimed to identify the possible associations between sex hormones and migraine attacks in young Saudi females.
The comparison of sex hormone levels during the 2 phases of menstrual cycle, namely, the follicular and luteal phases, between the migraineurs and controls revealed no significant difference. A prior study that tracked the urine levels of sex hormones, including estrogen and progesterone, on a daily basis found no difference between migraineurs and controls.10 However, this finding was not sufficient to overlook the influence of these hormones in migraine pathology. When the hormones were compared between the different classes of migraineurs, a dissimilarity in their sex hormone profiles was detected accordingly. Therefore, our data can shed light on the complexity of the role of the sex hormones, particularly estrogen, in the pathophysiology of migraine. Estrogen levels during the 2 phases of the menstrual cycle were significantly higher in the NMM group than in the control group. Therefore, the estrogen level might be a triggering or facilitating factor for the pain attacks in NMM. Some studies indicated that in female migraineurs, a high estrogen level might contribute to cortical spreading depression (CSD) and modulation of serotonin levels.11 Experimentally, an estradiol supplement administered to oophorectomized female rats induced CSD.12
The NMM group showed significant higher body weight and BMI compared to the other groups. Concurrently, a significant correlation was found between estrogen level and body weight. Estrogen can be stored in the adipose tissue, which acts as an extraovarian source of the hormone and contributes to the non-controlled elevation of blood estrogen level. Thus, increased body weight in this group of female migraineurs can aggravate the migraine pathology. In line with this finding, a clinical study on 110 overweight or obese females with migraine showed that the women responded positively to a weight loss program and demonstrated reduction in migraine pain and related disability.13
On the other hand, a significant lower luteal estrogen level was demonstrated in the migraineurs with a luteal attack onset than in those with a follicular attack onset. A migraine attack during the luteal phase is most probably an MM, as defined by ICHD-3.5 Nevertheless, the significantly lower estrogen level during the luteal phase that coincides with pain attack plausibly concurs with the explanation of the withdrawal theory. A sudden drop in estrogen level during the late luteal phase can activate an inflammatory response and facilitate the release of proinflammatory markers such as calcitonin gene-related protein, neurokinin, apolipoprotein E, and substance P.11
Furthermore, the MM group demonstrated a significantly higher luteal testosterone level compared to that of controls, with no significant difference seen with the testosterone level of the NMM group. In contrast, Rustichelli et al,14 demonstrated no difference in the level of testosterone between MM patients and controls; however, the subjects of Rustichelli et al’s study were older (19-45 years). Testosterone is believed to have a protective effect against the pathogenesis of migraine. It was found that testosterone levels negatively correlate with migraine disability assessment questionnaire scores (MIDAS) and the frequency of pain attacks.9 Thus, the elevated level of the luteal testosterone in our young MM patients might be a protective physiological mechanism and explain the progression of the disease and the increase in the pain frequency and intensity in older females who demonstrated a decrease in testosterone level, as reported by Li et al.9,15 Progesterone levels were not different in any of the studied groups during follicular as well as luteal phases of the menstrual cycle. Our findings were consistent with those reported by Rustichelli et al,14 and Li et al,9 who found no difference in progesterone levels between patients with MM and controls.
Study limitations
The current study might be limited by its small sample size. However, the narrow age group of our sample minimized the effect of confounding factors and highlighted the significant differences in the hormonal profiles of the studied groups.
In conclusion, we can conclude from our study that female migraineurs had a distinguished sex hormonal profile, that is not only differed from that of healthy controls but also differed between the types of migraine, MM and NMM. The latter presented with high estrogen level during both the follicular and luteal phases of the menstrual cycle, while MM was associated with low luteal estrogen levels. High estrogen level in NMM might culminate in CSD, whereas low luteal estrogen might justify the notion of the withdrawal theory and the inflammatory consequences of sudden drop of estrogen in MM. Our young MM migraineurs exhibited high luteal testosterone level that might act as a mitigation factor against headache attacks in young females.
Acknowledgment
The authors gratefully acknowledge Mr. Ranilo M. Tumbaga from the Department of Genetic Research, Institute for Research and Medical Consultations (IRMC), Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia for his assistance in the enzyme-linked immunosorbent assay analysis, and we would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. This study was funded by the College of Medicine, Imam Abdulrahman Bin Faisal University, Damman, Kingdom of Saudi Arabia.
- Received February 17, 2021.
- Accepted May 30, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.