


Abstract
Objectives: To investigate whether gastric Helicobacter pylori (H. pylori) infection is associated with the progress of nonalcoholic fatty liver disease (NAFLD) in Dali city, China.
Methods: One thousand and one hundred eighty-five adults who had visited a health examination center were enrolled. Nonalcoholic fatty liver disease and H. pylori infection were assessed by abdominal color ultrasound and 13C-urea breath test, respectively. Serum lipid metabolic indices were compared between NAFLD subjects without and with H. pylori infection.
Results: The prevalence rate of NAFLD for the entire study population (n=1185) was 44.6% (n=529), including 167 women and 362 men. Among 529 NAFLD subjects, H. pylori was confirmed as a significant and independent risk factor for NAFLD (95% CI 1.02-1.79, p=0.036, OR =1.35). Compared with H. pylori non-infected individuals (n=721), higher contents of LDL-C (p=0.012) along with TC (p=0.014) were also observed in H. pylori-infected individuals (n=464).
Conclusion: A positive correlation is identified between H. pylori infection and NAFLD.
Nonalcoholic fatty liver disease (NAFLD) is a frequent metabolic condition in humans, creating a global public health concern.1 An estimated 400 million people have NAFLD in China, and it has been linked to more than 100 thousand deaths.2,3 Research evidence shows that NAFLD is strongly related to insulin resistance, metabolic syndrome, as well as obesity.4 However, the association of gastrointestinal microbes to the pathogenesis of NAFLD remains unclear.5
Helicobacter pylori (H. pylori) pose a threat to nearly half of the world’s population.6,7 Infection of H. pylori is commonly responsible for gastritis, gastric cancer, as well as peptic ulcer disease. In particular, novel research findings have opined a strong link between H. pylori infection and extra-digestive manifestations, namely, diabetes, obesity, liver tumors, cardiovascular disease, and lipid metabolism disorders.8 Notably, in recent years, H. pylori infection has been viewed as a potentially important causative agent associated with the development of NAFLD.
However, connection linking H. pylori infection to NAFLD remains debated. Positive associations of NAFLD with H. pylori infection have been investigated in numerous studies,9-11 whereas some studies have reported conflicting results.12-15 Under these circumstance, more clinical data are needed to address the connection of NAFLD with H. pylori infection. Locally, no studies regarding NAFLD and H. pylori association are available. Therefore, herein, we primarily purposed to explore the association of NAFLD with H. pylori infection in medical check-ups in Dali city, a Bai ethnic minority area in western Yunnan province of China.
Methods
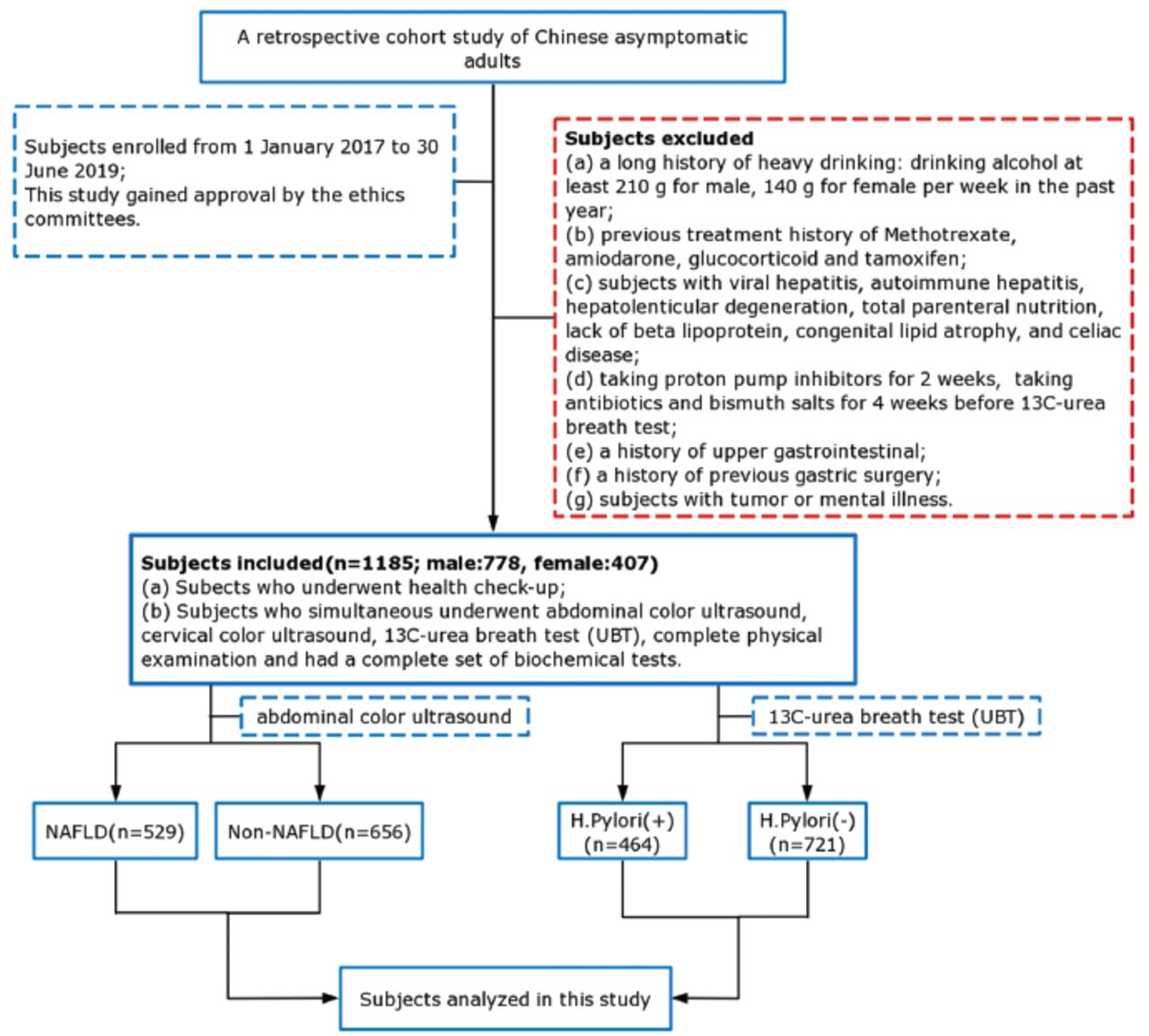
We conducted this retrospective research using electronic medical data from participants (age, >18 years) who underwent comprehensive health check-ups at a tertiary hospital in Dali city between January 2017 and June 2019 (Figure 1). We included data from participants consisting of anthropometric parameters and results of 13C-urea breath test (UBT), serum biochemistry, ultrasound color imaging of the abdomen, and ultrasound color imaging of neck. We excluded subjects who had (i) a history of significant alcohol intake: females (≥140 g/week), and males (≥210 g/week); (ii) a treatment history with amiodarone, methotrexate, glucocorticoid and tamoxifen; (iii) individuals with celiac disease, Wilson’s disease, viral hepatitis, lack of beta lipoprotein, autoimmune hepatitis, total parenteral nutrition, and congenital lipid atrophy; (iv) those under treatment with proton pump inhibitors (PPI) for 2 weeks or under treatment with bismuth salts and antibiotics for 4 weeks prior to the 13C-UBT; (v) individuals with upper gastrointestinal disorders’ history; (vi) participants with cancer or mental conditions; and (vii) previously underwent gastric surgery. The ethical committee of Dali University Hospital granted the study protocol and ethical approval (No: 20200118).
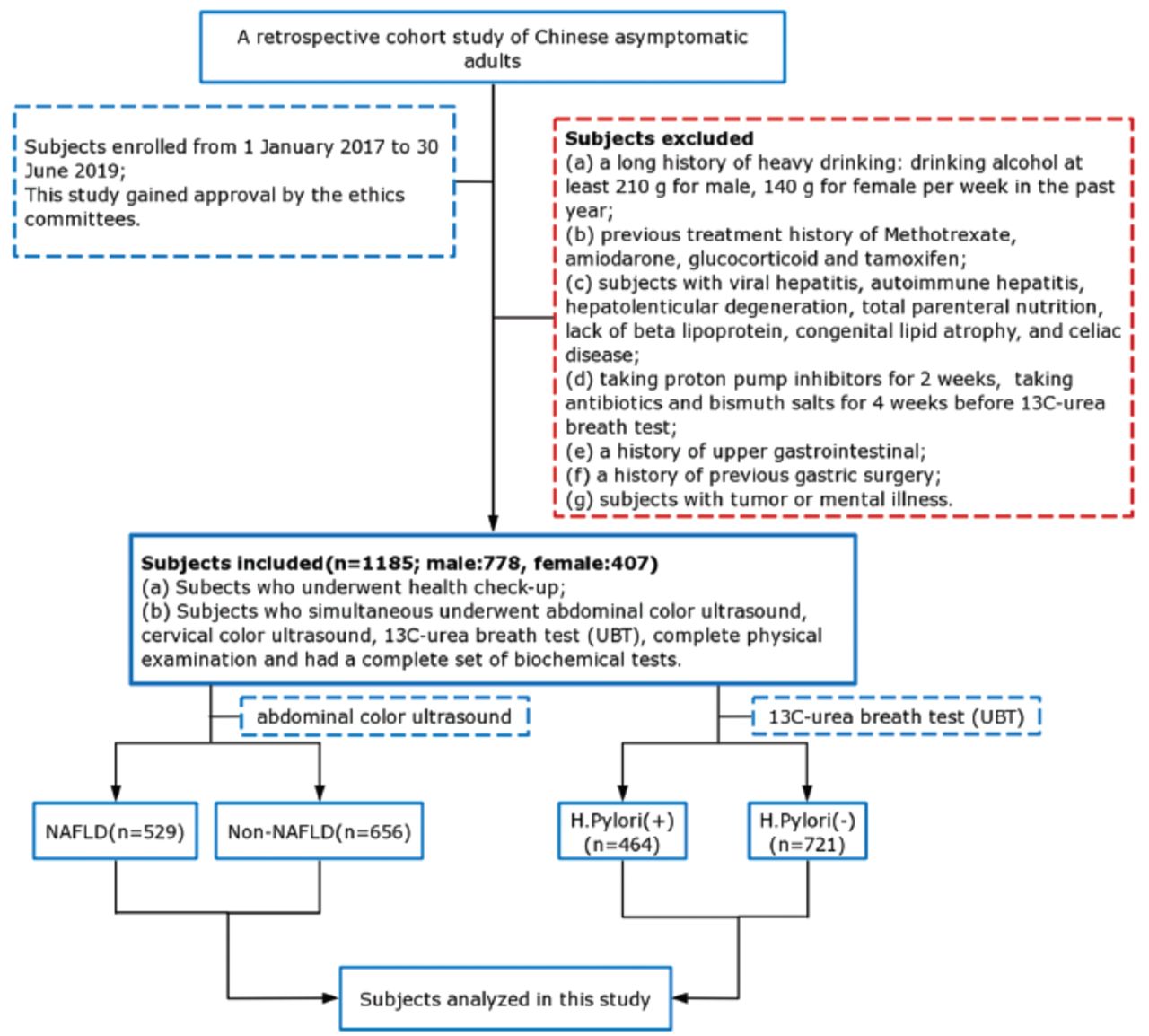
- Flowchart of study population selection flowchart. NAFLD: nonalcoholic fatty liver disease, H. pylori: Helicobacter pylori
Physical examinations and serum biochemical examinations
Anthropometric parameters (weight along with height) were also assessed. And body mass index (BMI) was determined as kg/m2. We recorded the systolic, as well as diastolic blood pressure during the physical examination. A fully automatic biochemical system (Hitachi 7600, Tokyo, Japan) was used to test the serum biochemical indices: alanine aminotransferase (ALT), total cholesterol (TC), aspartate aminotransferase (AST), low-density lipoprotein cholesterol (LDL-C), fasting plasma glucose (FPG), urea, albumin (ALB), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), creatinine, and uric acid.
Assessment of NAFLD
Each of the participant was subjected to Color Doppler ultrasound imaging of the abdomen by an independent radiologist with a Logiq E8 radiology ultrasound equipment (GE Corp., Chicago, IL, USA). We diagnosed NAFLD on the basis of the results of the ultrasound photographs and the current diagnostic reference criteria.16
Establishment of H. pylori infection
Each subject was assessed for H. pylori infection using 13C-UBT kit (Headway, Zhonghe, Shenzhen, China). After ≥8 hours of fasting overnight, we orally administered a 75 mg 13C-urea capsule to all subjects and collected 2 samples of exhaled breath at baseline, as well as 30 mins after the capsule was consumed. We analyzed the samples using a HCBT-01 13C detection system (Headway, Shenzhen, China). If the results of 2 samples differed by >4/thousand (δ‰) meant a participant was positive for H. pylori infection, as previously described.17
Statistical statistics
The characteristics of the subjects are presented as mean ± SD for normally distributed continuous variables and as percentages for categorical data. We compared the characteristics of subjects across the NAFLD status with the Chi-square test or t-test. Then logistic regression was employed to investigate the effect of various parameters on NAFLD and H. pylori infection association by adjusted odds ratios (ORs). We also constructed 4 different models. Model 1 included only H. pylori infection. Age and carotid plaque status were added to Model 2. Model 3 was Model 2 with further adjustment for ALT, AST, and UA levels. Finally, more potential indicators and confounders, including FPG, TC, TG, SBP, DBP, LDL-C, and BMI were added to Model 4. Point-biserial correlation was employed to evaluate the correlation between H. pylori infection and TC, as well as LDL-C.
Statistical analysis was implemented in the SPSS Statistics 23.0 software (for windows, IBM, Armonk, NY, USA). P-value of <0.05 signified statistical significance.
Results
Overall, 1185 participants (407 women and 778 men) were enrolled. The prevalence rate of NAFLD for the entire study population (n=1185) was 44.6% (n=529), including 167 women and 362 men. Participants with NAFLD were significantly older, with lower levels of HDL-C and higher weight, SBP, and DBP, as well as elevated contents of TC, AST, TG, FPG, LDL-C, and ALT (all p<0.05). Differences in ALB contents and height between the NAFLD and non-NAFLD subjects were not significant (p>0.05). A higher prevalence rate of H. pylori infection was reported in the individuals with NAFLD (43.5%) relative to that of in the individuals without NAFLD (35.7%, p=0.007) (Table 1).
- Comparison of study participants demographics and biochemical profiles between cgroup and non-NAFLD group.
Table 2 summarizes several risk factors related to NAFLD after logistic regression analysis. The levels of ALT (OR =1.02, 95% CI 1.01-1.03), BMI (OR=4.38, 95% CI 3.29-5.84), FPG (OR=2.29, 95% CI 1.31-3.40), TG (OR =2.33, 95% CI 1.73-3.14), and DBP (OR =1.73, 95% CI 1.17-2.56) were independent risk factor of NAFLD (all p<0.05). Notably, H. pylori was similarly a strong independent risk factor for NAFLD (95% CI 1.02-1.79, OR=1.35, p=0.036). These findings illustrate that H. pylori functions as a mediator of NAFLD.
- Univariate regression analysis for risk factors associated with nonalcoholic fatty liver disease (NAFLD).
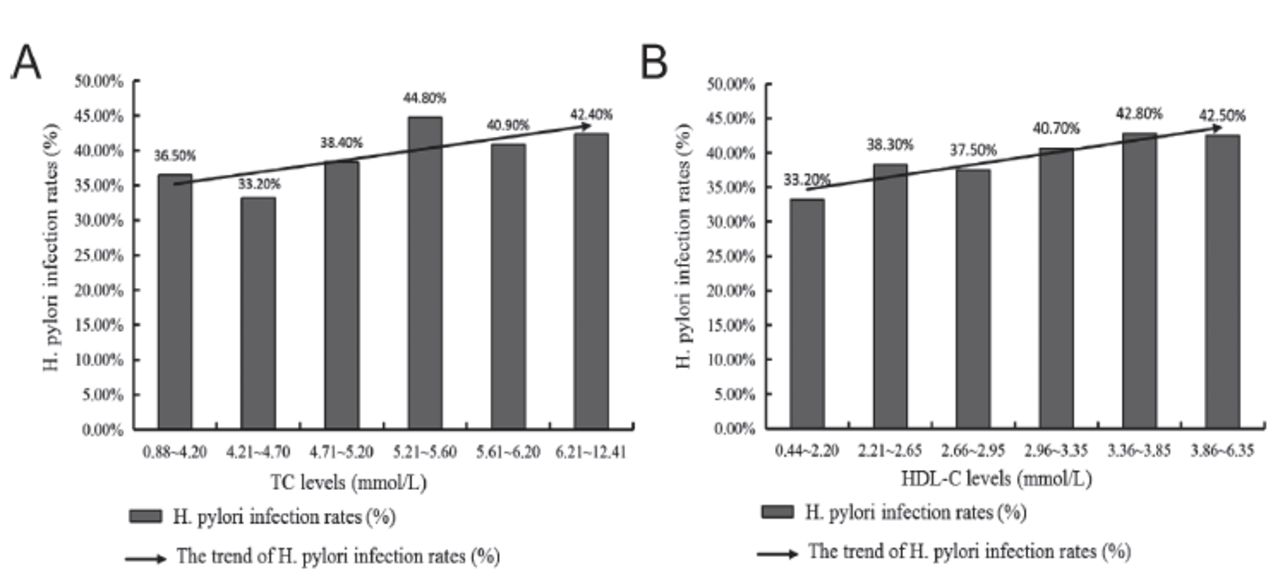
Furthermore, to clarify the link between NAFLD and H. pylori infection, we constructed 4 different models. Consequently, H. pylori infection (unadjusted OR=1.38; for 95% CI 1.09-1.75, p=0.007) was remarkably linked to NAFLD as indicated in Table 3. Additional adjustment for carotid plaque and age attenuated the result was 95% CI 1.05-1.68, OR =1.33, p=0.020. However, after adjusting the model for AST, UA, and ALT, the OR for NAFLD was escalated (95% CI 1.10-1.83, OR=1.42, p=0.008). In the fully adjusted model (Model 4), infection of H. pylori correlated with an elevated risk of NAFLD (95% CI 1.02-1.79, OR 1.35, p=0.036). To elucidate the potential underlying mechanisms of H. pylori infection in NAFLD, we conducted an analysis to determine the correlation of H. pylori infection with several metabolic syndrome constituents. Compared to the H. pylori (-) individuals, the H. pylori (+) individuals had elevated TC and LDL-C contents (all p<0.05, Table 4). However, the differences in FPG (p=0.492), TG (p=0.409), DBP (p=0.614), BMI (p=0.142), SBP (p=0.776), and HDL-C (p=0.087) between these 2 groups were not significant. Furthermore, point-biserial correlation was employed to evaluate the correlation between H. pylori infection and TC, as well as LDL-C. As presented in Figure 1, there was a positive correlation between H. pylori infection and TC (p=0.015, r=0.071, Figure 2A). And H. pylori infection was also positively correlated with LDL-C (p=0.013, r=0.072, Figure 2B). Collectively, our results provide evidence that infection of H. pylori may be involved in the pathogenesis of NAFLD by influencing the metabolism of cholesterol.
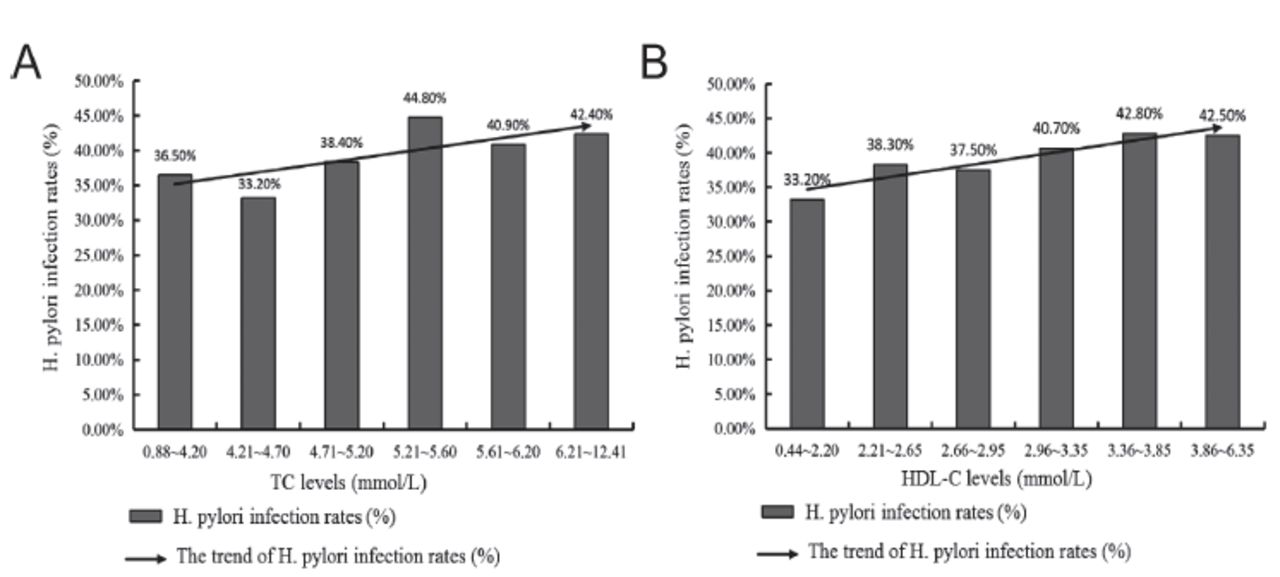
- Helicobacter pylori (H. pylori) infection rates in nonalcoholic fatty liver disease (NAFLD) individuals categorized by A) total cholesterol (TC) and B) low-density lipoprotein cholesterol (LDL-C).
- Multivariate logistic regression analysis for nonalcoholic fatty liver disease (NAFLD) after adjusting effects of confounders.
- Effect of Helicobacter pylori (H. pylori) infection on metabolic syndrome indicators in nonalcoholic fatty liver disease (NAFLD) individuals.
Discussion
Nonalcoholic fatty liver disease is a frequent metabolic affecting nearly one-third of the world’s population, but the underlying mechanism remains poorly understood. Many factors, namely, metabolic, behavioral, genetic, and environmental, may be responsible for NAFLD pathogenesis.18 Findings over recent years have established possible associations of H. pylori infection with NAFLD.19 Herein, a positive influence of H. pylori infection on NAFLD was demonstrated. Remarkably, after ruling out additional confounders, consisting of age, blood lipids, carotid plaque, blood glucose, liver enzymes, and blood pressure, H. pylori infection (95% CI 1.02-1.79, OR 1.35, p=0.036) remained the only independent factor for NAFLD. This finding is in accordance with that of a previous report which documented a positive correlation between NAFLD and H. pylori infection.20
The initial view of NAFLD is a hepatic indication of the metabolic disorder has been changing, and it is currently regarded that the occurrence of NAFLD may precede metabolic syndrome.21 Thus, when combined with the analysis of several metabolic indices, we obtained higher weight, DBP, and SBP and elevated contents of TG, FPG, TC, BMI, and LDL-C (all p<0.05) in individuals with NAFLD in contrast with those without NAFLD. We also identified DBP, BMI, FPG, and TG, as remarkable risk factors of NAFLD. Therefore, we speculated that a potential interaction exists between the NAFLD and metabolic syndrome constituents. As noted in another study, metabolic syndrome itself may contribute to the onset and progress of NAFLD, and vice versa.22
Abundant published research has demonstrated that infection of H. pylori is strongly associated with NAFLD, as well as metabolic syndrome.23-26 Herein, we also evaluated whether H. pylori infection affected various metabolic syndrome indicators (namely, HDL-C, SBP, FPG, TC, DBP, BMI, TG, and LDL-C). Notably, both LDL-C and TC contents were elevated in the H. pylori (+) group (p<0.05). Consequently, H. pylori infection may contribute to an escalation in LDL-C and TC contents. This finding is in accordance with a previous meta-analyses report that confirmed the influence of H. pylori infection on the lipid profile in serum.27 However, herein, the effects of H. pylori infection on other metabolic indicators were not verified. Here, we enumerate some possible reasons for our results. First, some guidelines before blood collection were provided to the participants. Some biochemical and physiological indicators of the participants in their original living environment (namely, kidney function, blood lipid, liver function, blood pressure, and blood glucose,) may have been underestimated. Second, the study included only subjects with higher education level working in government-affiliated institutions in Dali City. They are likely to have a higher level of health awareness than rural populations. Therefore, these study findings may be biased toward participants with better living standards, better dietary profiles, as well as good health awareness.
Study limitations
Our findings merit consideration, along with several potential limitations. First, this was a retrospective, single-center research. Another limitation of this study is the possible sample bias. Only subjects who underwent health check-ups were enrolled in the analysis. Thus, generalizing the findings to other populations is a challenge. Our present results require further verification using larger samples with different socioeconomic backgrounds. Third, no follow-up of the participants was performed. Fourth, we only confirmed that the infection of H. pylori was an independent risk factor for NAFLD in present study. The underlying mechanism of H. pylori infection evoking NAFLD was mere speculation. More in-depth prospective studies are required for the precise mechanistic association between H. pylori infection and NAFLD.
In summary, H. pylori infection may be a potential important contributor of NAFLD. However, further studies are needed to elucidate the precise mechanism of the relationship between H. pylori infection and NAFLD.
Acknowledgment
This work was funded by Yunnan Health Training Project of High Level Talents (#H-2019045), the Special Basic Cooperative Research Programs of Yunnan Provincial Undergraduate Universities’ Association (#202001BA070001-040 & 202001BA070001-055), and the National Natural Science Foundation, China (#81960363). We thank the Editage company in Shanghai (www.editage.cn) for their English language editing services of this manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 18, 2021.
- Accepted May 11, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.