


Abstract
Objectives: To systematically review the occurrence of magnet or receiver/stimulator displacement following cochlear implant (CI) placement complication and evaluate the existing literature on this topic.
Methods: A systematic literature search was conducted using PubMed, Scopus, Web of Science, Virtual Health Library (VHL), and Cochrane Library. Original studies reporting cases of magnet or receiver-stimulator migration occurring as a complication after CI placement were included. The quality of the included studies was evaluated using the National Institutes of Health Quality Assessment Tool for observational studies and CARE checklist for case studies.
Results: A total of 36 studies, including 6469 patients, were included. Magnet migration was reported in 82 (1.3%) patients, while receiver/stimulator was reported in 4 (0.1%) cases. The cause of magnet migration was identified in 78 cases; MRI-induced movement was the most frequently reported cause (n=43, 55.1%), followed by head trauma (n=25, 32.1%). A total of 20 studies involving 35 patients with magnet migration performed skull radiography to diagnose magnet migration. Revision/exploratory surgery with surgical repositioning or replacement was the most frequent management procedure (n=46).
Conclusions: Further research on magnet pocket design and standard protocols for MRI in CI users is needed. Early diagnosis of magnet migration and instant referral to specialized CI centers is necessary for proper management and prevention of major complications. PROSPERO REG. NO. CRD: 42020204514
Cochlear implants (CIs) are effective and safe for patients with moderate and severe hearing loss. Approximately half a million patients have received CI over the last decade.1 However, with their increasing use, several complications have been shown to contribute to CI failures and revision surgeries or re-implantation. The major complications include receiver-stimulator protrusion, electrode array migration, flap necrosis, otitis media, persistent perilymph leakage, and permanent facial nerve paresis.2,3
The number of imaging studies, especially magnetic resonance imaging (MRI), for examining neural structures, including the spinal cord and joints, has considerably increased over the last decade.4 Of note, MRI scans of CI users have been reported to jeopardize the magnet by causing displacement of the magnet out of its lodging.5-7 Magnet migration can lead to difficulties with fixation of the internal part of the implant, causing discomfort as well as skin infection and necrosis.5-7 Some protective measures have been recommended by implant manufacturers, such as wearing head bandages during MRI; however, these measures may be insufficient since the reports of displacement have been increasing.8,9 Also, other many manufacturers implemented the features of a freely rotating and self-aligning magnet in CI devices in which no complication was reported with a total of 19 MRI scans.8 A recent review concluded a superior effect for rotatable magnet during MRI scans with no need for device removal or head wrap.10
Migration of the CI magnet may also occur because of head trauma, which is commonly reported in children11 and has been reported in adults.12 Of note, redness and swelling on the receiver-stimulator site were found to be associated with magnet displacement even in the absence of a clear history of trauma or MRI scan.13
If magnet displacement is suspected, confirmation of the diagnosis through radiological studies is essential, and it is usually followed by revision surgery to re-fix the implant. Since migration of the CI magnet or receiver-stimulator is considered a rare complication, no previous studies have clearly reported the prevalence of this complication, performed systematic qualitative studies of the pooled evidence, or established standard practices and management protocols for the patients. Therefore, this report aimed to systematically review the occurrence of magnet or receiver-stimulator migration after CI and conduct a full evaluation of this complication. Further, this study aimed to outline the clinical presentations, diagnostic approaches, and surgical interventions for these rare complications.
Methods
The present systematic review followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
In August 2020, the following search terms were used to search for relevant articles: (migration,displacement, or dislocation) AND (cochlear or cochlea) AND (implant or implantation). Electronic databases including PubMed, Scopus, Web of Science, Virtual Health Library (VHL), and Cochrane Library, without language or year restrictions, were used. Additionally, a manual search of potentially eligible studies was performed. Articles were collected in a single library through Endnote, and all duplicate references were omitted. Two authors blindly screened all articles based on the predetermined inclusion and exclusion criteria. Papers were deemed included if they reported original data of magnet or receiver-stimulator migration as a complication after CI. There were no restrictions on study design, country of research, or year of publication. However, we excluded (i) posters, commentaries, letters, review articles, theses, conferences, and book chapters; (ii) studies with overlapped data sets; (iii) non-English articles; and (iv) in vitro studies.
Data extraction
Two authors independently extracted data from the eventually included studies. Pilot extraction was initially performed using 5 articles to prepare a consistent extraction form to fit the data and reduce heterogeneity. The extraction form covered 3 main domains: (i) the baseline demographics of the included studies, including patients’ age, gender, and sample size, (ii) patients’ clinical presentations and device type, and (iii) patient outcomes, including the number of cases showing migration, causes of migration, investigations, and management approaches. The outcomes were classified on the basis of the cause of migration as either post-MRI, post-head trauma, or unexplained migration. All discrepancies were resolved through discussion among the authors and with a third senior author.
Quality assessment and data analysis
All included studies were evaluated by 2 separate authors using the National Institutes of Health Quality Assessment Tool for observational studies14 and the CARE checklist for case studies.15 Descriptive data analysis was performed using Microsoft Excel to calculate numbers, proportions, means, and standard deviations (SD).
Results
Our electronic search retrieved 1657 studies, of which only 972 were left after removing duplicated references. On the basis of title and abstract screening, 902 references were excluded, while 70 references were assigned for further full-text screening. Finally, 36 studies were included for qualitative synthesis in the systematic review (Figure 1).
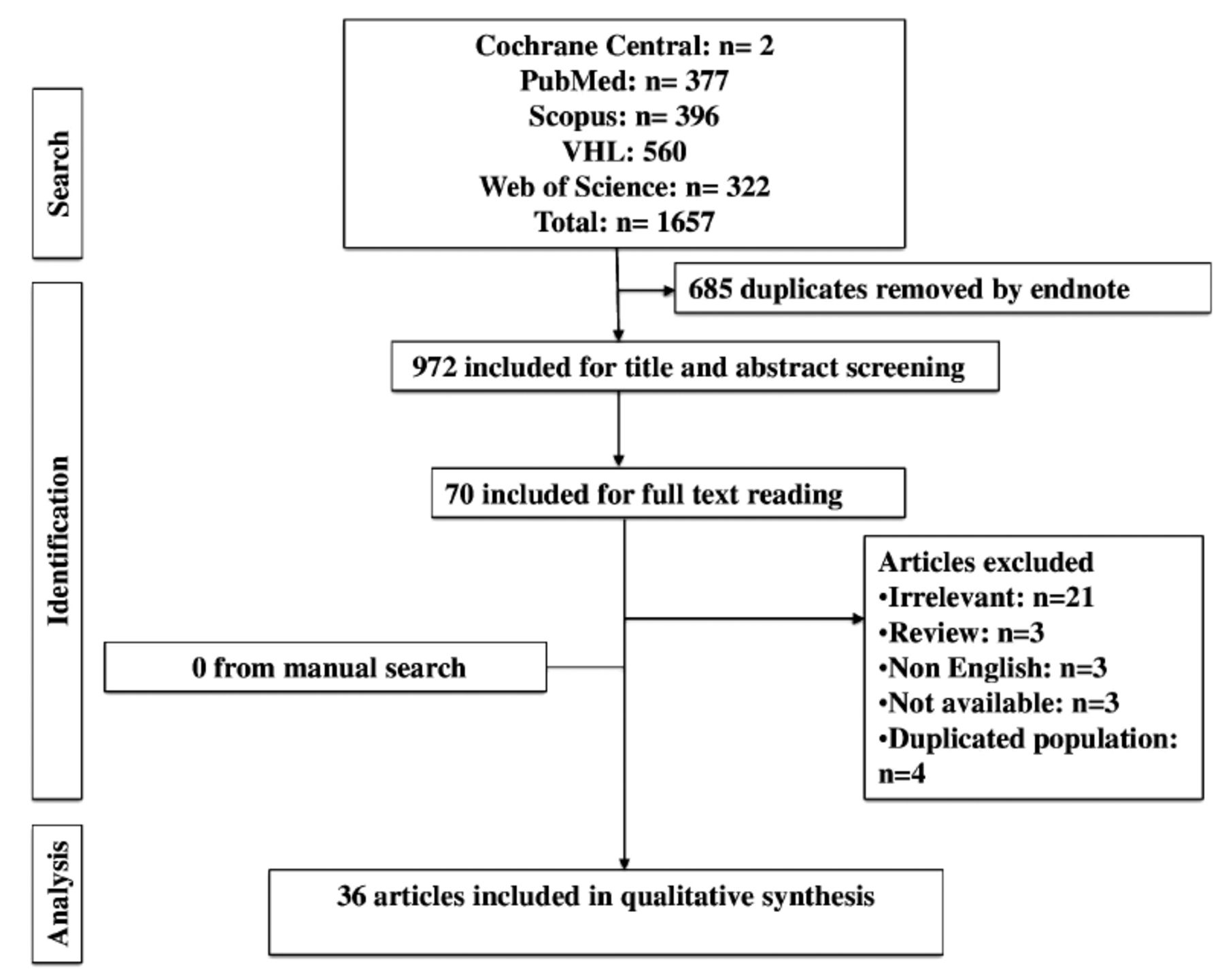
- Flow diagram of studies’ screening and inclusion. VHL: Virtual Health Library
Baseline characters of included studies
A total of 18 retrospective case reviews and 18 case studies including 6469 patients were included (34 studies on magnet displacement, one study on receiver-stimulator migration, and one study evaluating both magnet and receiver-stimulator displacement). Magnet migration was reported in 82 (1.3%) patients, while receiver/stimulator was reported in 4 (0.1%) cases. The average quality assessment score was 10 for case reports and 8 for observational studies. The basic characteristics of individual studies, including country, device type, and causes of hearing loss, are shown in Table 1.
-Basic characteristics of patients in our included studies.
Clinical characteristics of patients showing magnet displacement according to the reasons for migration
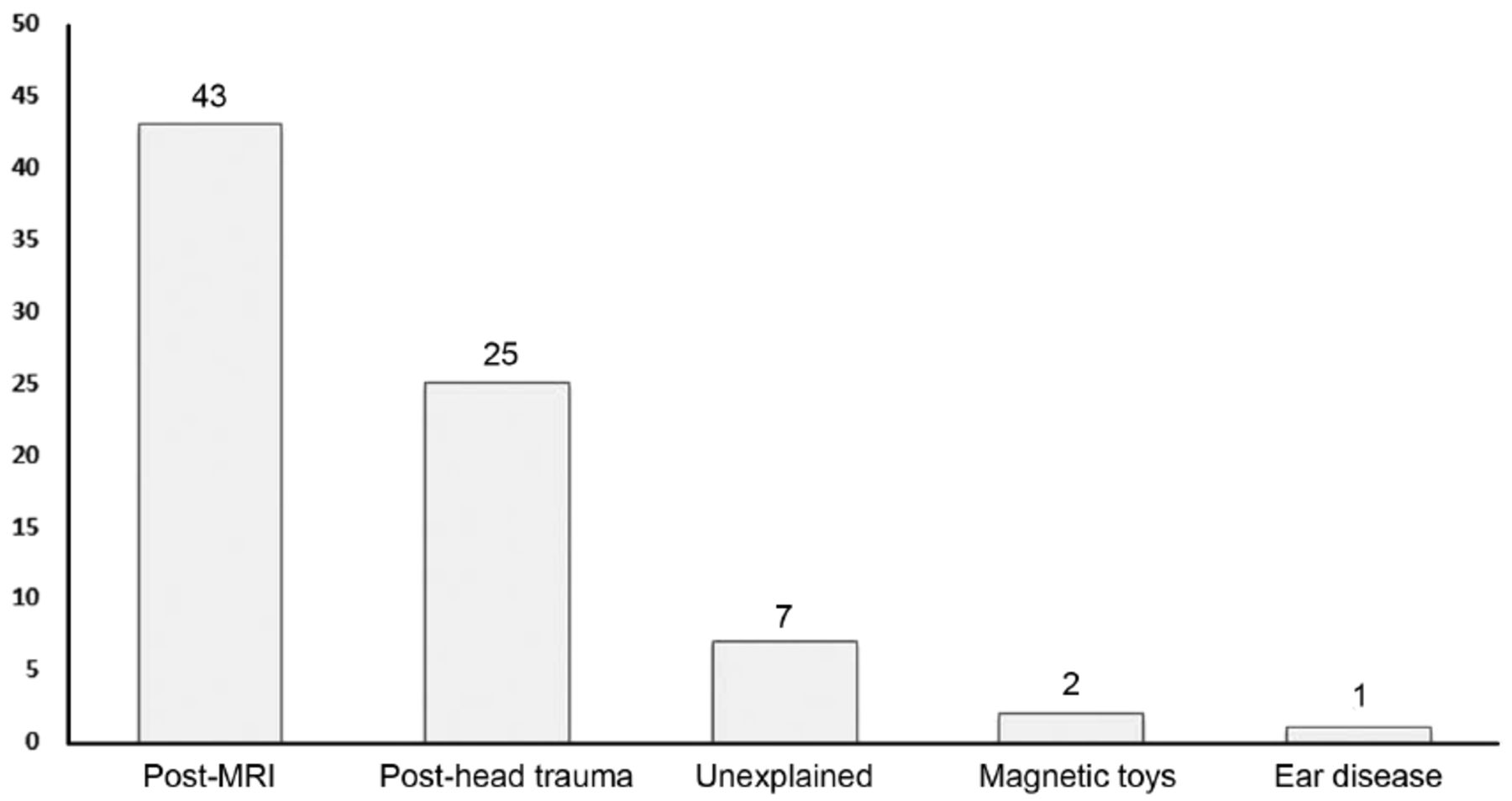
Of the 82 cases involving magnet migration, the cause of migration was identified in 78 cases. Magnetic resonance imaging examination was the most frequently reported cause (n=43, 55.1%), followed by head trauma (n=25, 32.1%). In addition, magnet migration due to unexplained reasons (no history of apparent trauma or MRI) or no apparent cause was identified in 7 cases (9%). Playing with magnetic toys was also reported in 2 cases. Chronic suppurative otitis media was associated in one case (Figure 2).
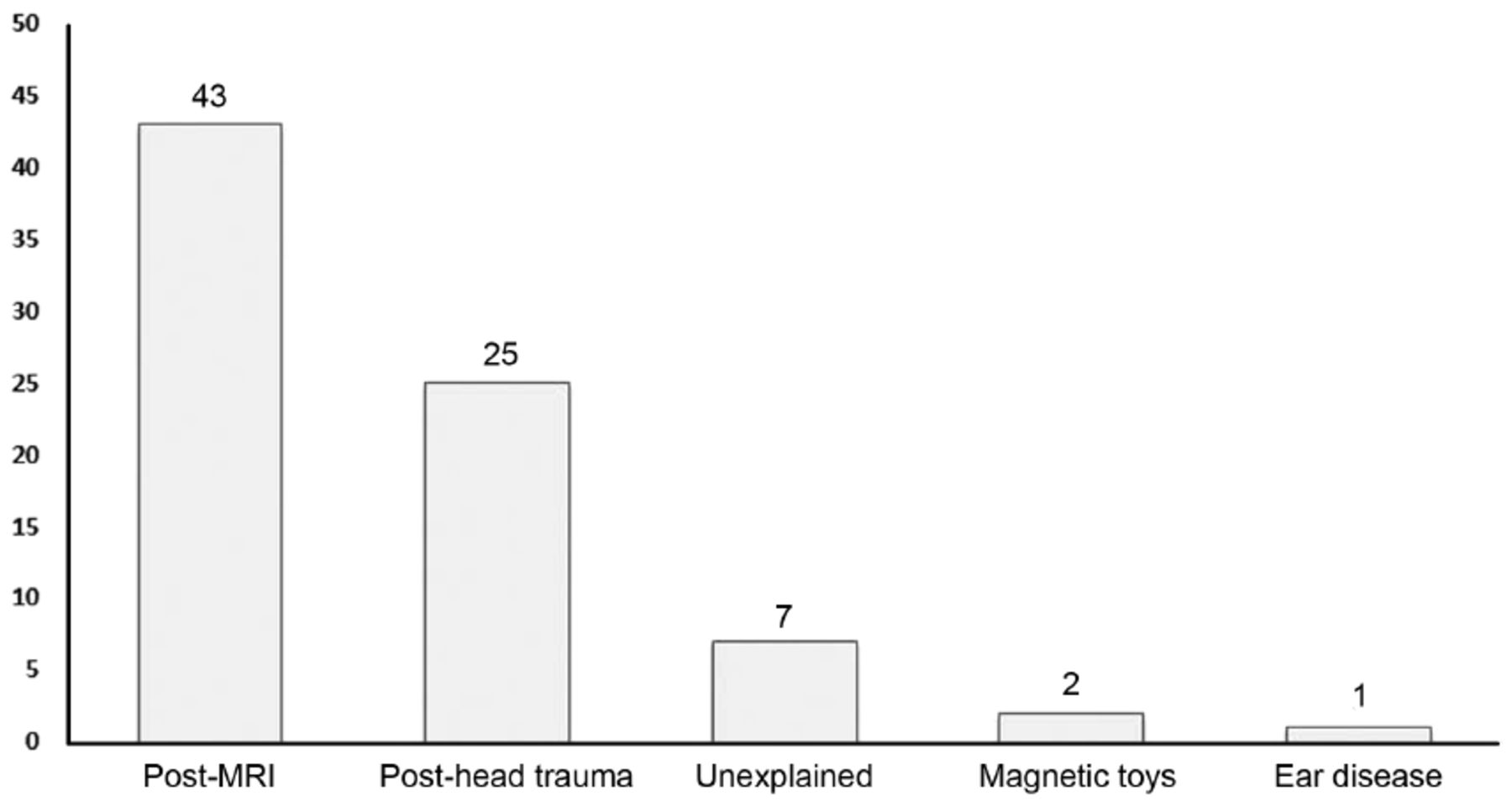
- Reasons for magnet migration in accordance with the authors’ reporting.
A total of 13 (30.2%) patients with post-MRI magnet migration experienced pain and discomfort during the MRI scan. A head bandage was applied in 14 patients during the MRI scan. All patients were exposed to 1.5 T MRI, except for one patient who was exposed to 3 T MRI. Clinical examination revealed redness, swelling, or a bulge over the magnet site; a bulge in the receiver-stimulator site was demonstrated in the majority of cases. In patients with head trauma, clinical examination relieved diffuse swelling with a visible or palpable magnet over the internal receiver-stimulator coil. However, cases without an apparent history of trauma or MRI presented with deterioration of sound and auditory skills (Table 2).
- Clinical characteristics of magnet displacement according to the reason of migration.
Management of reported cases with magnet displacement
A total of 20 studies involving 35 patients with magnet migration used skull radiographs to diagnose magnet migration, and 2 studies used both radiography and computed tomography (CT).16,17 The magnet was shown to be outside the receiver-stimulator container, outside the antenna coil, and migrated from the silicon pocket. Using a CT scan in a case report, magnet rotation was observed without total implant displacement.18 Furthermore, in one study, magnet migration was diagnosed by a poor response through neuroresponse telemetry.19 Revision/exploratory surgery with surgical repositioning or replacement was the most frequent procedure for magnet migration management (n=46). Emergency surgery was indicated in a patient who experienced pain during an MRI scan.18 Moreover, spontaneous reduction was reported in another case.20 Table 3 summarizes the radiological findings and management in cases with magnet migration.
- Investigation and management of magnet migration cases.
Discussion
Magnet or receiver/stimulator displacement following CI surgery is a rare complication; however, it is a serious event and may be underestimated. This systematic review summarizes the evidence from original studies to report the prevalence, clinical characteristics, and management of magnet or receiver-stimulator migration following CI. The current study identified that MRI scans and a history of head trauma are the main causes of magnet migration, but this condition may also occur without apparent reasons. The static and dynamic magnetic fields generated by MRI scanners can affect the magnet of the CI, leading to its displacement. The literature suggested that 1.5 T MRI is a safe and efficacious imaging method for patients with CI.21,22 Newer and better CI devices may show reduced influence of the adverse events induced by the electromagnetic field of MRI machines; however, several patients showed magnet migration following 1.5 T imaging.18,20,23 It is therefore important to consider magnet problems if patients present with tenderness or pain in the temporal region after an MRI scan.24 The data extracted in our systematic review revealed that a head bandage was applied in almost all included studies with individual data. Although the use of Cochlear® is advised while performing MRI in CI users with a compression bandage as well as a “splint” being directly placed above the magnet,25 magnet displacement has also been reported even in studies that used head bandage and followed all precautions.16,20,26 Moreover, it is difficult to quantify the success rate of head bandages in the absence of large data. Therefore, the need for an MRI scan must be carefully assessed and discussed with CI users and their families.27 More importantly, the position of the patients in the MRI machine and the imaging protocol may influence the magnet status. Previous reports have recommended that MRI scans should be performed at specialized CI centers where otorhinolaryngologists can guide the patients about proper precautionary measures and carefully monitor them after MRI imaging for possible clinical signs of magnet migration.17
The main challenge after magnet migration is to promptly perform and confirm the diagnosis. Of note, many patients presented with redness, swelling, or bulging over the magnet site bulge in the receiver-stimulator site. In addition, the majority of patients with post-MRI magnet displacement experienced pain and discomfort during the MRI procedure. However, there were no consistent presenting features. While radiological methods including radiography, CT, and cone-beam CT (CBCT) can confirm the diagnosis, radiography may be recommended because of the low radiation risks. Notably, Hassepass et al recommended performing radiography immediately after MRI scans in CI users who experienced pain or any problems during MRI without magnet removal to exclude possible magnet displacement and prevent further complications.28 Recently, the diagnostic ultrasound has been utilized as one of the diagnostic tools for identifying magnet dislocation.29
Once the diagnosis of magnet dislocation has been proven, most cases would require surgical repositioning or replacement of the magnet. A literature search revealed that the procedure can be conducted under general anesthesia or local anesthesia.17 A commonly followed incision approach is the incision of a semicircular cut around the antenna of the CI.17 A larger incision may affect the long-term wound outcomes; therefore, Leong et al recommended an endoscopic fixation technique through a smaller access.9 Leinung et al preferred an open surgical technique along with a small semicircular incision of the skin, between the magnet and the antenna parts.17 However, some cases, which can be recognized as grade one displacement in accordance with the Gubbels and McMenomey classification, can be managed through manual fixation from outside.22,30,31 Notably, patients who underwent manual repositioning should be instructed about the potential recurrence of magnet migration because of the physical impact close to the CI. In these cases, a skin incision line is recommended so that a repositioning procedure can be converted into a replacement operation.27
The significance of this study lies in the fact that it is the first systematic review to provide qualitative evidence regarding these rare complications after CI.
Study limitations
The first is the relatively small number of included participants and studies, although 5 major databases were selected for the literature search. The second limitation is that the inferences from our study relied on data from case reports and cohort analysis, and the lack of randomized trials and controlled studies may affect the generalization of study conclusions. Lastly, the included patients were of different ages, received various device types, and underwent different implantation techniques. Therefore, larger studies are needed to compare different types of CI devices, patients’ basic demographics, exact causes of migration, best diagnostic approach, and effective management.
In conclusion, magnet or receiver-stimulator displacement are critical complications of CI and may not be as rare as previously perceived. This systematic review revealed that MRI and head trauma were the most frequently responsible factors for magnet displacement. Patients may present with redness and swelling at the implant site, and skull radiography is usually performed to confirm the diagnosis. Further research is needed on magnet pocket design, and standard protocols for MRI in CI users are required to lessen magnet or receiver-stimulator migration. Therefore, the necessity of an MRI scan must be carefully assessed and discussed with CI users and their families. In addition, healthcare providers should carefully evaluate CI users after MRI scans and head trauma. Early diagnosis and instant referral to specialized CI centers for appropriate management are extremely important for the prevention of partial or complete explantation of the implant.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 17, 2021.
- Accepted June 27, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.