


Abstract
Objectives: To describe characteristics, mechanism, and factors associated with morbidity and mortality of pediatrics with burn injuries.
Methods: This cross-sectional retrospective study examined all pediatrics with burn injuries carried out at King Abdulaziz Medical City, Riyadh, Saudi Arabia, from 2015-2020. Collected data included demographics, mechanism of burn, total body surface area (TBSA) burned, body region burned, incidence of infection, renal failure, scars, and respiratory events.
Results: The study included 370 patients. Approximately 47.0% were aged ≤2 years, and 61.0% were males. The most common burn mechanism was scald burn (54%), 59.2% had a TBSA of 0-10%, and 60.3% had regional burns on the upper limbs. During follow-up, 5 patients died (incidence rate [IR]=1.60/100 patient/years [PYs]). Morbidity events included blood/sepsis infection (IR=2.87/100 PYs), urine infection (IR=8.30/100 PYs), wound infection (IR=21.72/100 PYs), renal failure (IR=0.96/100 PYs), and respiratory infections (IR=1.60/100 PYs). In a multivariate Cox regression analysis, factors independently associated with combined hazard of morbidity and mortality were female gender (hazard ratio [HR]=1.64, 95% confidence intervel [CI]: [1.01-2.67], p=0.047), TBSA (HR=3.20, 95% CI: [1.828-5.585], p<0.0001), and length of hospital stay (HR=3.14, 95% CI: [1.91-5.17], p=0.000).
Conclusion: This study identifies certain characteristics suggestive of poor outcomes of pediatric burn injuries that are relevant to clinical management and prevention programs. Larger multicenter studies are required to fully characterize pediatric patients with burn injuries and to identify factors that adversely affect their prognosis.
Burn injuries are a significant public health problem in low and middle-income countries. According to the World Health Organization (WHO), there were more than 7.1 million fire-related unintentional burns in 2018, and the incidence rate was 110 cases per 100,000 individuals per year.1 Approximately, 180,000 deaths are attributable to burn injuries annually. The incidence amounts to 187/100,000 patient-years (PYs) in the East Mediterranean Region (EMR), 19/100,000 PYs in the United States, and as high as 243/100,000 PYs in Southeast Asia. Moreover, burns are the sixth leading cause of loss of productive years (disability-adjusted life years).1
Children are predominantly susceptible to burns, and the incidence of burn deaths among those under 5 years of age in Africa is over 2 times greater among children under 5 years of age worldwide. Furthermore, boys under 5 years of age living in low- and middle-income EMR countries are almost 2 times more likely to die from burns than those living in Europe.1
Burn injury may lead to death or contribute to morbidity among children. As far as we know, there are few published studies on the epidemiology of burns among children in Saudi Arabia. During the 1990s, the rate of childhood burn deaths ranged from 5-11% according to 2 prospective cross-sectional studies (including 105 and 197 patients over 2 years old) and one retrospective study (examining medical records of 435 patients over 8 years).2-4 Most of the deaths occur among male infants and toddlers with high burn surface area caused by accidental burn injuries, which mainly lead to septicemia and heart failure.
Three recent studies identified fewer death cases among many patients (148-787 patients in each study) over one, 2, and 9 years.5-7 Severely burned patients who survived death would probably suffer from prolonged morbidity. The aim of this study is to determine factors associated with mortality and morbidity among pediatrics with burn injuries carried out at King Abdulaziz Medical City (KAMC), Riyadh, Saudi Arabia.
Methods
This cross-sectional retrospective study considered all children aged 18 years or younger who were admitted with burn injuries between January 2015 and July 2020 to KAMC in Riyadh, Saudi Arabia. King Abdulaziz Medical City is one of the many large medical cities in Riyadh and is equipped with the latest technologies to treat complex injuries. Although access to KAMC is limited to the employees of the Ministry of National Guards and their first-degree relatives, it covers a large segment of the Saudi population. The Institutional Review Board of King Abdullah International Medical Research Center reviewed and approved this study.
All consecutive cases of pediatrics with burn injuries causing damage to skin or any other part of the body as a consequence of extreme heat, flame, contact with heated objects, or chemicals admitted at KAMC from January 2015 until July 2020, were considered for inclusion into the study. Patients with incomplete data were excluded.
Data were collected from KAMC’s electronic medical records (BestCare). In addition, demographics data on mortality and comorbidities were extracted. The variables examined included the mechanism of burns (flame, scald, contact, chemical, and electrical), total body surface area (TBSA) burned, body region burned (head and neck, trunk, upper limb, lower limb, and genital area), infections (blood/sepsis, urine, and wound), renal failure, respiratory events, and length of stay at the hospital. This study adopted the definitions of extended stay (21 days) and short stay (less than 21 days) reported by Doctoroff et al.8
Statistical analysis
Descriptive statistics were used to summarize data. Continuous data were expressed as the mean (standard deviation) or median (interquartile range), and categorical data were expressed as the frequency (%). Continuous data were compared using a t-test or Mann-Whitney test, and categorical data were compared using the Chi-squared test or the Fisher exact test as appropriate. Patients were followed from initial clinic visit until date of death or last known clinic visit. Cumulative incidence rate (IR) was calculated by dividing reported cases of comorbid conditions or death occurring during follow-up period (per 100 PYs). Cox proportional hazard regression models were constructed to identify factors associated with the hazard of combined clinical outcome (mortality and comorbid conditions). Variables found significant in the univariate analysis were included in the final multivariate model. All tests were 2-sided, and a p-value of <0.05 was considered significant. Missing data were imputed using the multiple imputation technique. Collected data were entered and analyzed using Statistical Package for the Social Sciences for Windows, version 25.0 (IBM Corp., Armonk, NY, USA).
Results
From 2015-2020, a total of 370 children were identified as burn patients. Almost half (46.5%) were 0-2 years old. Most of them were Saudis (93.2%), and nearly two-thirds were males (60.8%). The most common mechanism was scald burn (54.1%), 59.2% had a TBSA of 0-10%, and 60.3% had burns on the upper-limb region. The majority (81.1%) of patients stayed less than 21 days at the hospital (Table 1).
- Baseline demographic and clinical characteristics.
During follow-up, 5 (1.35%) patients died, and the IR was 1.60 per 100 PYs, as shown in Table 2. Overall, 270 (73.0%) patients developed at least one comorbid condition (IR = 86.22/100 PYs). These conditions included urine, wound, respiratory, blood/sepsis infections, and renal failure. The most common of these was wound infections (18.4%; IR = 21.72/100 PYs). The proportion of patients with combined morbidity and mortality was significantly higher among females (p=0.002), those with TBSA >10% (p<0.0001), and those with length of hospital stay of ≥21 days (p<0.0001), as shown in Table 3.
- Morbidity and mortality events following burn injury.
- Distribution of mortality and morbidity events by gender, total body surface area, and length of stay.
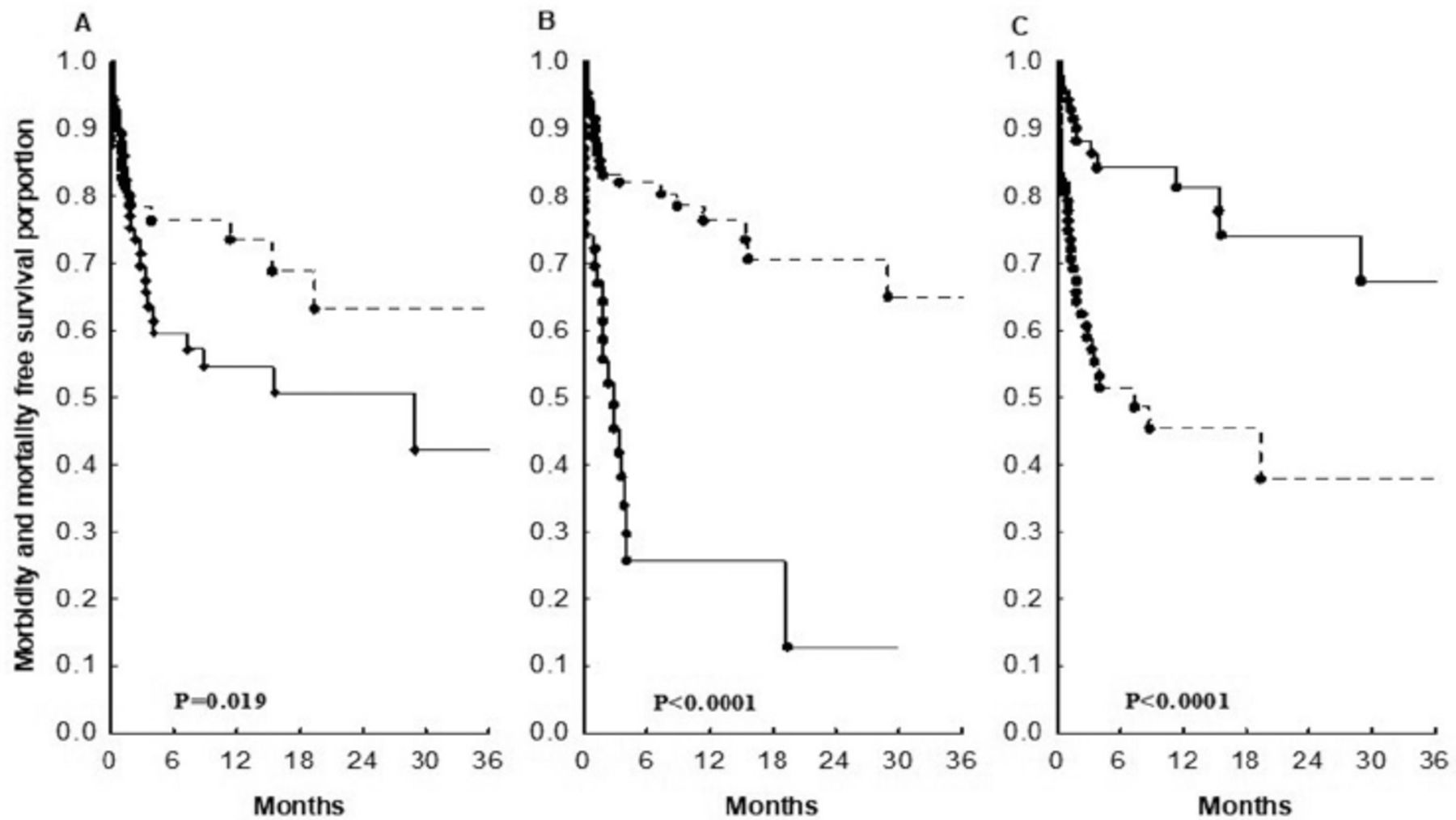
A Kaplan-Meier analysis was carried out to examine the rates of combined morbidity and mortality-free survival. The results revealed that females (log-rank test; p=0.019), those with TBSA of >10% (log-rank test; p<0.0001), and those with length of hospital stay of ≥21 days (log-rank test; p<0.0001) had significantly lower survival rates and more rapid progression to combined morbidity and mortality events, as shown in Figure 1. A Cox proportional hazards regression analysis was carried out to identify factors associated with the hazard of combined morbidity and mortality. In the univariate analysis, gender, TBSA, and length of hospital stay were significantly associated with the hazard of combined mortality and morbidity events, as shown in Table 4. The final multivariate model shows that females had a higher hazard than males (hazard ratio [HR]=1.64, 95% CI: [1.01-2.67], p=0.017). Furthermore, patients with TBSA of >10% had higher hazard than those with TBSA of 0-10% (HR=3.20, 95% CI: [1.83-5.39], p<0.0001), and those who stayed ≥21 days in the hospital had higher hazard than those who stayed <21 days (HR=3.14, 95% CI: [1.91-5.17], p<0.0001).
- Cox regression analysis for factors associated with combined morbidity and mortality events.

- MKaplan-Meier probabilities of morbidity and mortality free survival stratified by: A) gender (female: solid-line, male: dotted-line), B) length of stay (>20 days: solid-line, ≤20 days: dotted-line), and C) total body surface area (0-10%: solid-line, >10%: dotted-line).
Discussion
This study documents the spectrum of major morbid conditions and death following burn events and their association with demographic and clinical characteristics of patients with burn injuries. The study has identified certain characteristics that are suggestive of poor outcomes, such as gender, TBSA, and extended length of stay. The findings are relevant to clinical management and prevention programs for patients with burn injuries.
The findings indicated that the most of the admitted burn patients were male infants with 0-10% TBSA, which was mainly caused by scald burn. The majority of children were admitted with burns in the upper-limb area and subsequently developed wound infection. Females with TBSA more than 10%, especially in the trunk and lower-limb areas, were more likely to develop morbidity related to burn injury. In addition, the longer burn patients stayed at the hospital, the more likely they were to develop morbidity related to the burn injuries.
The mortality rate of burns admitted to KAMC, Riyadh, Saudi Arabia, from 2015-2020 was low. However, this was not the case for the morbidity rate as the rates of urine infection, wound infection, and scars were high. The factors of gender, TBSA, and LOS are possible predictors of increased hazards of mortality and morbidity related to burns injuries.
The results showed a significant gender-related difference in the occurrence of morbidity and that gender could be a predictor for mortality- and morbidity-specific survival. International studies showed that gender was a predictor for both mortality and morbidity with different burn characteristics.9-12 Interestingly, in this study, females had more risk of developing mortality and morbidity related to burn injuries. However, further studies are needed to confirm this finding. Furthermore, the results of this study revealed that TBSA and length of stay were strong predictors for morbidity. Similar results were found in several international studies where TBSA was a strong predictor for morbidity and mortality.9,13-24
In regard to mortality and morbidity rates, similar results were found in international studies. A Dutch study found that the infection rates per 1,000 patient days for 55.2% of pneumonia, 8.9% of primary bloodstream infections, 18.5% of wound infection, and 41.7% of urinary-tract infections.25 However, the mortality rate in the present study was lower than that in Europe (1.4-18.0%).26 The reason behind the low mortality rate estimated in this study remains unclear. However, it is unlikely that this could be due to under-reporting or inability to capture all death events because we employed an aggressive approach to confirm all mortality events occurring during study period. The observed difference maybe attributed to differences in severity of burn injuries; the majority (~60.0%) of patients in this cohort had <10% TBSA. Other possible reasons might be the effectiveness of government programs in decreasing mortality among children and the availability of advanced health care systems. Further studies with a larger sample size are needed to confirm this.
Study limitations
The study was based on a single healthcare setting, so the results may not be generalizable beyond the area of the institution involved. In addition, some burn characteristics were not recorded in the medical records, so they were not included in data analysis. A few observations were missing but were imputed. The sample size was relatively small, and the findings might differ in a larger cohort.
In conclusion, this study has described characteristics of patients with burns that could be used to predict progression to morbid conditions and mortality in patients with burn injuries. The findings could inform decision-makers in healthcare services about necessary preventive measures with the aim of improving the prognosis and quality of life of such patients. Such improvement in the quality and efficiency of health services could facilitate the success of health-sector transformation programs by reaching objectives according to Saudi Vision 2030.27 Nevertheless, multicenter studies with larger sample sizes are required to characterize patients with burn injuries and to identify factors that might adversely affect their prognosis.
Acknowledgment
The authors gratefully acknowledge Ms. Hazel Devera and Ms. Martites Thomas for their unwavering dedication and efforts in data acquisition. We also would like to thank American Manuscript Editors (https://americanmanuscripteditors.com/startanewproject.aspx) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 30, 2021.
- Accepted April 7, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.