


Abstract
Objectives: To assess the effectiveness of reinforcing sutures after surgery for rectal cancer and its associated impact on postoperative recovery. Anastomotic leakage (AL) is a common and serious complication after anteriorrectal resection. It is currently unclear whether laparoscopic intracorporeal reinforcingsutures can effectively reduce the incidence of AL.
Method: From inception to 2024, the literature search was conducted using a variety of databases, including PubMed, the Chinese biomedical literature database (CBM), Wanfang, EMBASE, the Cochrane Library, VIP, and China National Knowledge Infrastructure (CNKI), to identify relevant articles. Free-text forms were used to search the literature: “rectal cancer”, “rectal neoplasms”, “reinforcing sutures”, and “anastomotic leakage” or AL. The search was undertaken by 2 different reviewers, who independently evaluated the studies.
Result: Twelve retrospective studies and 4 RCTs were analyzed in all. A total of 3147 individuals were identified, with 1512 receiving reinforcing sutures and 1635 not. Patients who underwent laparoscopic surgery to get reinforcing sutures had a notably decreased occurrence of anastomotic leakage, according to our data. (OR 0.33; 95% CI 0.21-0.51, p<0.00001). It had an earlier anal exhaust time and a shorter hospitalization. The 2 different groups did not differ substantially with regard to intraoperative blood loss or the rate of postoperative intestinal obstruction. However, patients who received reinforced sutures via a laparoscopic approach cost more operative time (MD=16.77, 95% CI 11.31–22.23, p<0.00001).
Conclusion: The occurrence of AL can be greatly decreased through the use of a laparoscopic approach for anastomotic reinforcement, which may be a better option after radical surgery for rectal patients. However, more RCT studies with large sample sizes are needed.
PROSPERO: CRD42024548847
Based on the World Healthcare Organization (WHO), colorectal tumors are among the most common tumors of the gastrointestinal system. They have the world’s third highest incidence rate, accounting for almost 10% of all cancers. Additionally, they rank as the world’s fourth most widespread cause of cancer-related deaths, with a yearly rise in developing countries.1 Approximately 70% of colorectal cancers are rectal cancers and low rectal cancers are the most common subtype.2
According to recent research, laparoscopic rectal surgery represents safe and feasible.3 Compared to traditional open surgery, the advantages of laparoscopic surgery include fewer injuries, faster recuperation, and clearer surgical vision. However, laparoscopic surgery has not been demonstrated to reduce anastomotic leakage after surgery.4
Anastomotic leakage is a serious complication with rates of incidence between 3.4%-20% and mortality up to 18%.5 Numerous factors, such as male gender, smoking, obesity, large tumor, diabetes, and preoperative radiation, are connected with the incidence of AL.6 The prevention of anastomotic leakage is a common yet challenging subject in the field of colorectal surgery.
Surgeons use a variety of methods to minimise the chance of anastomotic leakage, including prophylactic ileostomy, anal tube decompression, and reinforced anastomotic sutures. The double stapling technique (DST) creates weaknesses due to crossing staple lines, known as the “dog-ear” structure.7-9 Anastomotic leakage can be reduced due to intraoperative reinforcing sutures, according to new studies.10
A meta-analysis by Zhang et al11 and Wang et al12 showed that the use of anastomotic reinforcement sutures has been demonstrated to have a notable effect on the reduction of anastomotic leakage. However, anastomotic suturing can be performed by 2 different surgical approaches, laparoscopic intracorporeal reinforcing sutures and transanal reinforcing sutures, and different surgical approaches may have different effects on the results of the study.13,14 Therefore, this study included all relevant literature on anastomotic suturing using laparoscopic sutures with the aim of evaluating whether anastomotic reinforcement suturing after radical surgery can lower the chance of anastomotic leakage and its associated impact on postoperative recovery.
Methods
Our study was completed at Rizhao Hospital of Traditional Chinese Medicine in Shandong Province, China, in 2024. A literature search of PubMed, Wanfang, the Chinese Biomedical Literature Database (CBM), EMBASE, the Cochrane Library, China National Knowledge Infrastructure (CNKI), and VIP was conducted from the establishment of the database to 2024. Free-text forms were used to search the literature included”rectal cancer”, “rectal neoplasms”, “reinforcing sutures”,”reinforcement suturing” and “anastomotic leakage” or “AL”. Two different reviewers (Wang and Song) conducted the search and independently assessed the studies.
The following were the inclusion criteria for this research: i) population: people with rectal cancer who underwent laparoscopic surgery; ii) intervention: laparoscopic intracorporeal reinforcing sutures; iii) comparison: no reinforcing sutures; iv) outcome: anastomotic leakage or other postoperative complications; and v) study design: RCTs or retrospective studies. Research was not included in this analysis. if i) there was unclear reporting of the data or results. ii) case reports (medicine), reviews, meta-analyses, and meeting records were not included, or if the study did not include a control group, iii) transanal reinforcing sutures, or iv) robotic surgery.
The search was undertaken by 2 authors (Wang and Song), who independently evaluated the studies. Disagreements were discussed. The primary outcome was anastomotic leakage. Other results were intraoperative blood loss, intestinal obstruction rate, operation time, length of hospital stay, and first anal evacuation time. The most important information that was collected from each of the selected studies is as follows: BMI, tumor location and size, TNM status, surgical approach, first author, country and year of publication, type of study, total cases included, genders, and age.
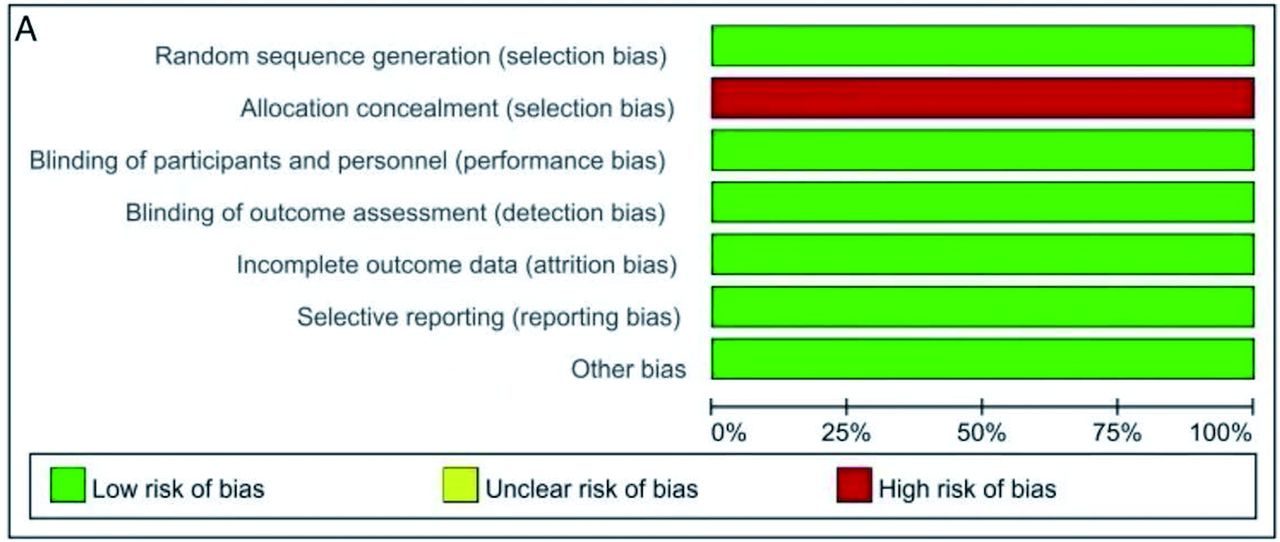
The Cochrane risk of bias tool was employed to evaluate 4 randomized controlled trials (RCTs). They were classified as “low risk,” “unclear risk,” or “high risk” according to the criteria established for 7 domains. (The risk of bias graph is seen in Figure 1A; The risk of bias summary is seen in Figure 1B).


- The Cochrane risk of bias assessment tool was used to evaluate the included articles’ quality. A) Risk of bias graph; B) Risk of bias summary.
The Newcastle-Ottawa Scale (NOS) was employed to assess the quality of 12 CCS studies (Table 1).
- Quality evaluation of the included articles (CCS) using the Newcastle-Ottawa scale.
Statistical analysis
The review was carried out using Review Manager 5.4 (RevMan, The Cochrane Collaboration, Copenhagen, Denmark). The Mantel-Haenszel method was used for the statistical analysis for operation time, anastomotic leakage, first anal evacuation time, hospital stay, and other postoperative complications, including intestinal obstruction and intraoperative blood loss. The analysis of dichotomous data was conducted using odds ratios (OR) and 95% confidence interval (95% CI). The mean difference (MD) and 95% CI of continuous data were subjected to analysis. The outcomes are shown using forest plots. The I² statistic was applied for the purpose of evaluating the presence and extent of statistical heterogeneity. A p-value of <0.05 was deemed to represent a statistically significant result.
Results
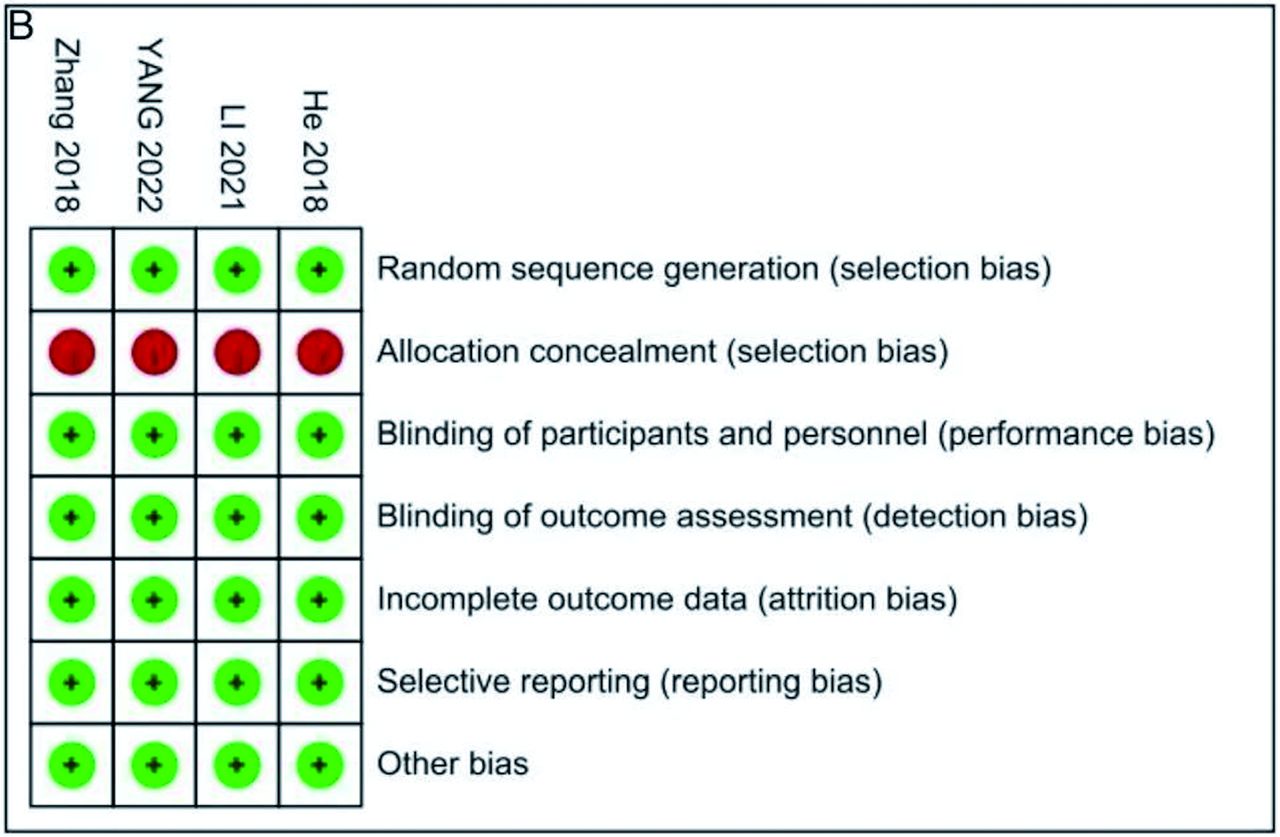
Finally, 4 randomized controlled trials and 12 retrospective studies were included.15-27 The literature screening and inclusion process is detailed in Figure 2. Anastomotic suturing was performed laparoscopically in all 16 included studies. Publications for the included studies ranged from 2015 to 2024. Total 3147 patients were identified, including 1512 patients who received laparoscopic reinforcing sutures and 1635 patients who did not (Tables 2 & 3).

- Flow diagram of study selection.
- Characteristics of all included studies.
- General information of the included studies.
Anastomotic leakage
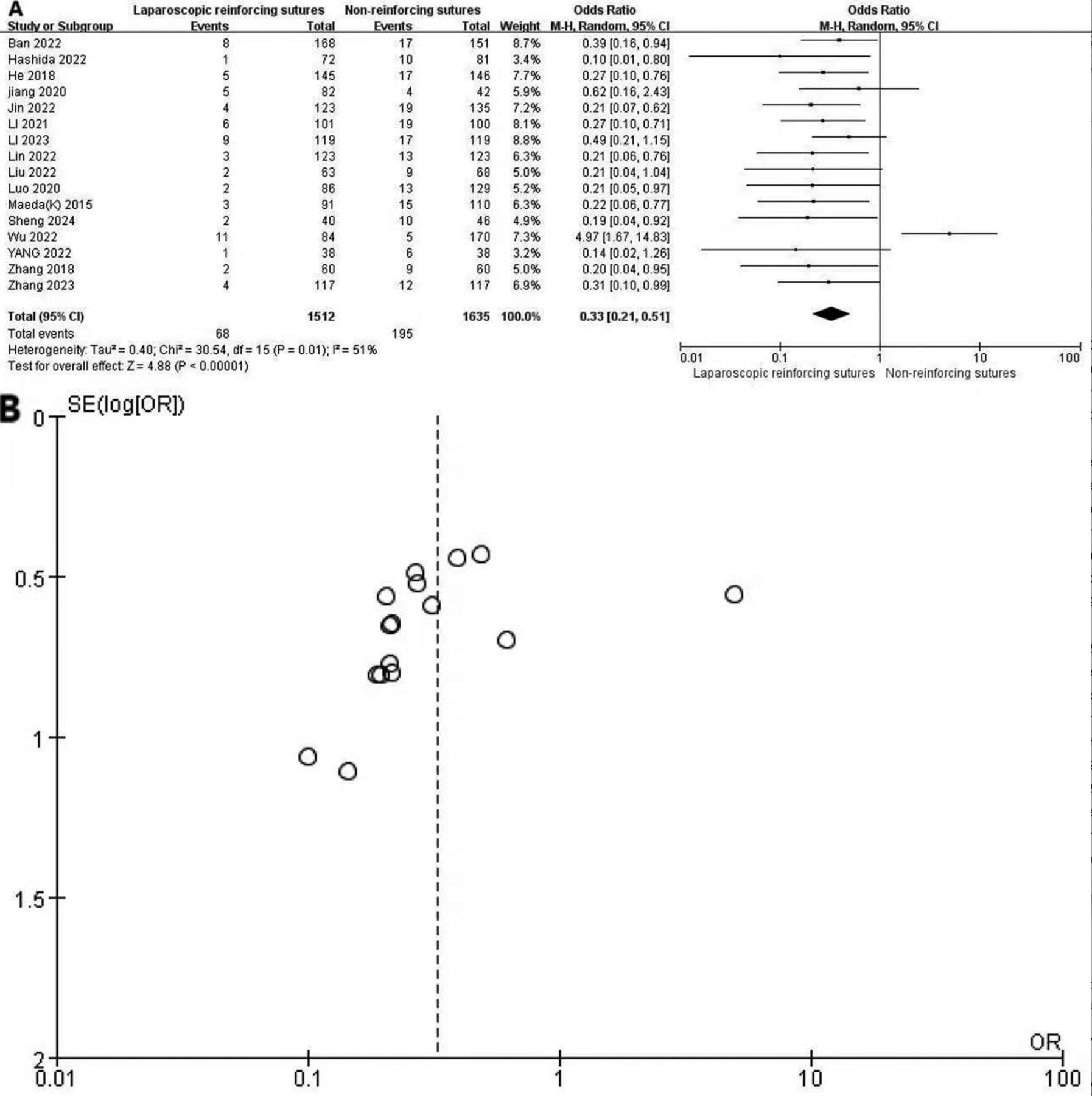
Anastomotic leakage was reported in all 16 included studies. Heterogeneity exists among articles. (I2=51%, p=0.01). According to our statistical analysis, the laparoscopic approach for anastomosis suturing was linked with a fewer occurrences of anastomotic leakage than the unreinforced suture. Anastomotic leakage was notably reduced in the group that underwent laparoscopic reinfored sutures. (In Figure 3A, OR 0.33; 95% CI: 0.21-0.51, p<0.00001, forest plots are shown).

- Comparison of anastomotic leakage between laparoscopic reinforcing sutures and non-reinforcing sutures. A) Forest plot of anastomotic leakage; B) Funnel plot of anastomotic leakage.
Exhaust time
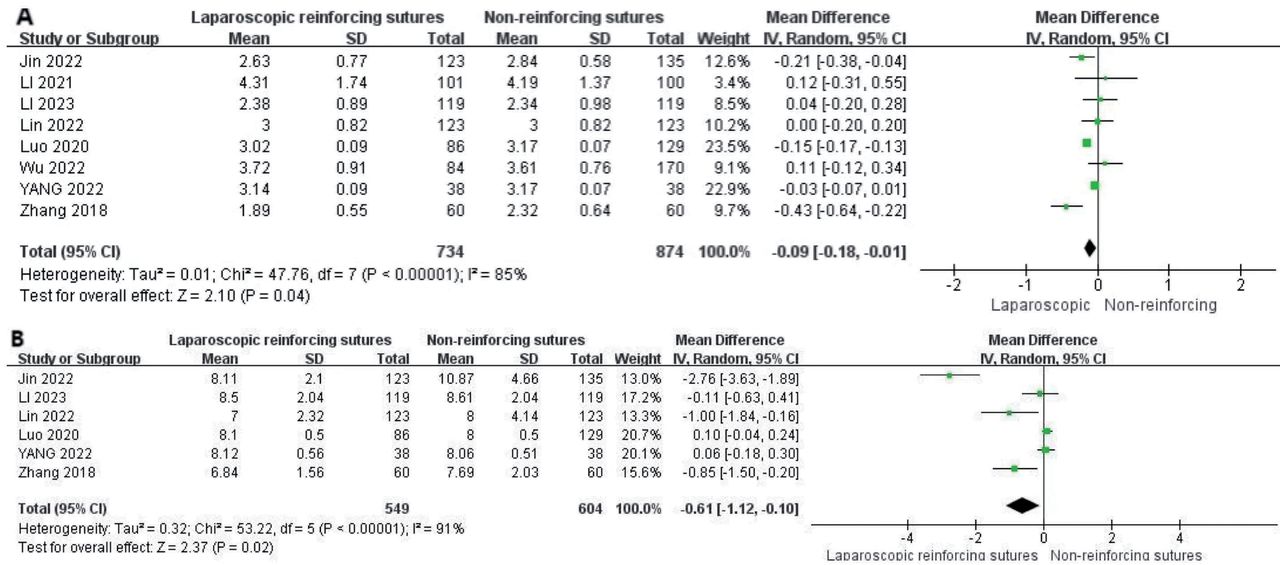
The first anal exhaust time was recorded in 8 articles. Heterogeneity exists among articles. (I2=85%, p<0.05). According to our statistical analysis, the first anal exhaust time of the anastomotic suture using a laparoscopic approach occurred earlier than that of the unreinforced suture. (In Figure 4A, MD=-0.09, 95% CI -0.18--0.01, p=0.04, forest plots are shown).

- Forest plots comparing laparoscopic reinforcing sutures to non-reinforcing sutures. A) Forest plot of the exhaust time; B) Forest plot of hospital stay.
Hospital stay
Six articles reported hospital stay. Heterogeneity exists among articles. (I2=91%, p<0.05). In comparison to the un-reinforced suture, the laparoscopic anastomotic suture resulted in a significantly shorter hospital stay, based on our data (MD=-0.61, 95% CI-1.12- -0.10; p=0.02) (Figure 4B).
Intraoperative blood loss
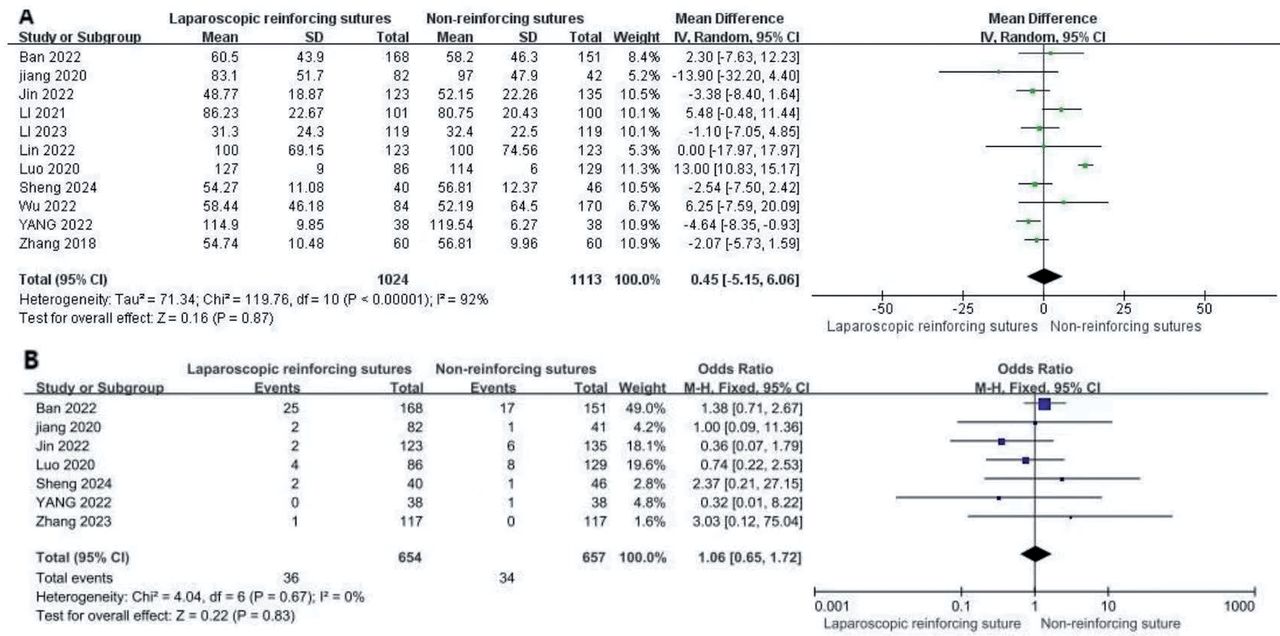
Eleven articles reported intraoperative blood loss. Heterogeneity exists among articles. (I2=92%, p<0.05). Our statistical analysis revealed that intraoperative bleeding was not significantly different between them. (MD=0.45, 95% CI-5.15-6.06, p=0.87) (Figure 5A).

- Forest plots comparing laparoscopic reinforcing sutures to non-reinforcing sutures. A) Forest plot of intraoperative blood loss; B) Forest plot of the occurrence of bowel obstruction
Intestinal obstruction
Seven studies reported the occurrence of bowel obstruction. We evaluated these 7 studies by use of the I2 statistic and found no heterogeneity (I2=0, p=0.67). The rate of intestinal obstruction did not differ significantly between the 2 groups. (OR=1.06, 95% CI=0.65-1.72; p=0.83) (Figure 5B).
Operation time
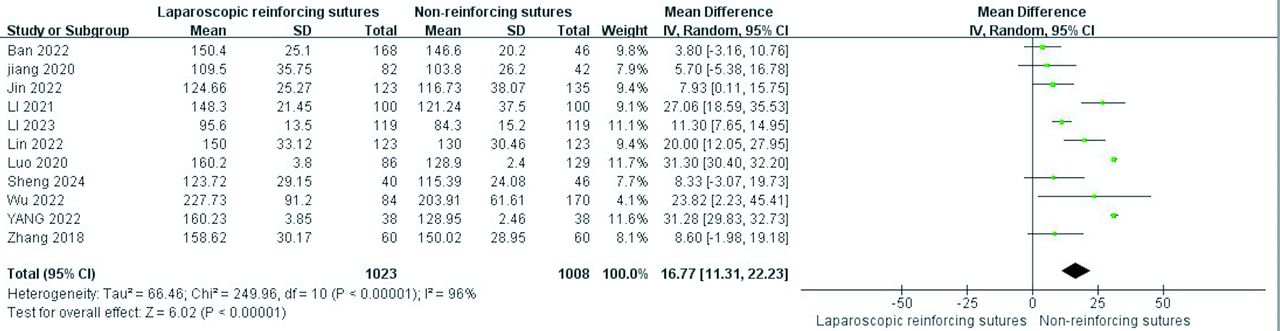
The operation time was included in eleven papers. Heterogeneity exists among articles. (I2=96%, p<0.05). According to our statistical analysis, anastomotic suturing performed by a laparoscopic approach requires a longer operating time than that for unreinforced suturing. (MD=16.77, 95% CI 11.31–22.23, p<0.00001) (Figure 6).

- Forest plot of the operation time.
Sensitivity analysis
There was obvious heterogeneity of anastomotic leakage, so We conducted a sensitivity analysis by eliminating articles one by one. We found that I2=0, heterogeneity disappeared when one study, Wu et al16 was excluded. And the heterogeneity did not change significantly when the other 15 studies were removed one at a time.
Wu et al’s16 study showed that laparoscopic reinforcement of suture anastomosis was not definitively effective in preventing postoperative anastomotic leakage occurrence, which should be the reason for the significant heterogeneity, but this study was retrospective with a small sample and some limitations.
Heterogeneity also exists in operation time, first exhaust time, hospital stay, and intraoperative blood loss. We used the same sensitivity analysis method and found no significant change in heterogeneity. This reflects the stability of the results.
Assessment of publication bias
Our study focused mainly on anastomotic leakage; thus, we used funnel plots to analyze publication bias and discovered that the scatter plots are not symmetrical on either side, which is an indication of publication bias (funnel plots are shown in Figure 3B).
Discussion
Anastomotic leakage rate may be reduced by intraoperative strengthening of the anastomosis, according to recent research.10 Nevertheless, the application of reinforcing sutures in open surgery is challenging due to the limited pelvic view field. Laparoscopic surgery offers the advantage of superior magnification visualization with endoscopy, thus it can be easier to put reinforcing sutures in laparoscopic surgery than in open procedures.28 However, laparoscopic suturing of the anastomosis requires a greater level of suturing and costs more time. Therefore, it is still debatable if laparoscopic anastomotic suture reinforcement could decrease the occurrence of postoperative anastomotic leaking.
In this research, we assessed the effectiveness of reinforcing sutures using a laparoscopic approach after radical surgery for patients diagnosed with rectal carcinoma. The occurrence of anastomotic leakage was markedly reduced by the application of reinforced sutures, as the results of this study demonstrated. The “dog-ear” area is most likely to result in anastomotic leakage because these areas are structurally weak and have poor blood supply. Sutures with anastomotic reinforcement may decrease the incidence of AL by reducing anastomotic tension, increasing blood supply, and strengthening weak areas. Reinforcing this weak point or anastomosis with barbed or absorbable sutures after reconstructing the digestive tract may lower the rate of anastomotic leakage.29
A well-healed anastomosis promotes the recovery of gastrointestinal function and allows for earlier anal exhaustion.11 According to our statistical analysis, the first anal exhaust time of the anastomotic suture using a laparoscopic approach occurred earlier than that of the unreinforced suture. The recovery of gastrointestinal function is a key indicator of rectal cancer surgery. When the gastrointestinal function of the patient is restored, a step-by-step increase in diet can be contemplated, thereby reducing the amount of intravenous fluids, reducing costs, speeding up the recovery of the patient, and thus shortening the length of hospital stay.30 Compared to the unreinforced suture, the laparoscopic anastomotic suture had a substantially shorter hospital stay based on our data.
According to our statistical analysis, between the 2 groups, there was no obvious distinction in intraoperative bleeding. The dissection of inferior mesenteric artery and inferior mesenteric vein, as well as chronic bleeding from surgical wounds, is the most likely cause of bleeding in rectal cancer surgery. With the ongoing advancement of laparoscopic surgical techniques and the wide application of ultrasonic knife and 3D laparoscopy, the surgical field is clearer, vascularization is handled more carefully, hemostasis effect is better, and the amount of intraoperative bleeding can be only a few milliliters or even less.31 Anastomotic bleeding is another serious postoperative complication, which was mentioned less in 16 articles without further analysis and will need to be confirmed by further studies.6
Laparoscopic anastomotic reinforcement suturing is controversial because some scholars believe that suturing will cause anastomotic stenosis, leading to a variety of complications such as bowel obstruction.32 Our analysis revealed that laparoscopic intracorporeal reinforcing sutures does not increase the incidence of postoperative bowel obstruction. This may be due to advances in laparoscopic suturing techniques.
The operation time for anastomotic suturing via a laparoscopic approach is longer than that for unreinforced suturing in our statistical analysis. The longer operation time is due to the additional suture step, especially in patients with a low anastomotic position. These suture steps are challenging and time consuming for many of our young surgeons because the lower the anastomosis is, the more difficult it is to expose the surgical field. This increases the difficulty of suturing, especially in patients with a narrow pelvic space.
However, by using barbed sutures, the knotting step during suturing can be reduced, resulting in an overall reduction in operative time.33 As surgical techniques evolve and surgeon skills improve, laparoscopic intracorporeal reinforcing sutures will become more proficient, and the operative time will continue to decrease. Therefore, laparoscopic intracorporeal reinforcing sutures may be a better option after surgery for rectal cancer.
Study limitation
The current study is limited by several factors, including the small number of randomized controlled trials (RCTs) included in the analysis (only 4), and there is a lack of data from other countries because all included studies were conducted in Asia. So more high-quality RCTs in different countries are needed to support these conclusions in the future. At present, there are 2 types of anastomotic sutures: interrupted sutures and continuous sutures, and different types of sutures may have different effects on the results of the study; therefore, more clinical studies are needed.
In conclusion,our meta-analysis demonstrates that the occurrence of AL can be greatly decreased through the use of a laparoscopic approach for anastomotic reinforcement, which may be a better option after radical surgery for rectal patients. However, more RCT studies with large sample sizes are needed.
Acknowledgment
We would like to thank AJE and STS for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 30, 2024.
- Accepted November 14, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.