


ABSTRACT
Objectives: To comprehensively understand the relationship between infertility medications and the risk of breast cancer (BC) in females.
Methods: Relevant literature search using different databases (PubMed, The Cochrane Library, Embase, Scopus, and Web of Sciences) following preferred reporting items for systematic reviews and meta-analyses guidelines was carried out from 2003-2023. Population-based studies comparing the incidence of BC after hormonal fertility treatment and a control group were included. In addition, random and fixed effect models were used to carry out meta-analyses.
Results: A total of 15 studies involving 92,555 women were included in this review. The pooled analysis using risk ratios (RRs) showed no evidence of increased BC risk associated with hormonal fertility medications (RR=1.00, 95% confidence interval [CI]: [0.97-1.02], p=0.83). The level of heterogeneity, as indicated by the I² statistic, was low (32%), and the Q test was not statistically significant. Sensitivity analysis using a random-effects model yielded consistent findings, suggesting no increased BC development risk with infertility medications. Among the 4 studies reporting hazard ratios (HRs), a significant protective effect on BC risk was observed (HR=0.91, 95% CI: [0.88-0.94], p<0.001). The heterogeneity was substantially high (I²=96%), and the Q test demonstrated statistical significance. Sensitivity analysis using a random-effects model showed that heterogeneity remained constant, suggesting that the heterogeneity was attributable to the methods utilized in the included studies rather than being a result of statistical heterogeneity. The overall effect, as determined by the HR, was 1.01 and was not statistically significant (p=0.94).
Conclusion: This meta-analysis found no evidence of increased risk of BC following hormonal infertility treatment. However, the results should be illustrated cautiously, given the heterogeneity between studies.
PROSPERO No. ID: CRD42024569158
Among the malignancies in the reproductive stage of women, breast cancer (BC) is considered as the most prevalent malignancy, with significant cases detected annually.1 The approximate estimate in 2022 was 2.3 million females identified with BC and 670,000 deaths also occurred worldwide.2 Breast cancer is characterized by uncontrolled growth of cancerous cells within the stroma and epithelium of the mammary glands. Over the years, considerable progress has been carriedout in BC research, leading to new insights into BC diagnosis, progression, prognosis, metastasis, and treatment. Despite advancements in the understanding of BC, it remains a major public health concern and a challenging condition for management.3
Breast cancer development is attributed to variety of factors, with the oncogenic and proliferative activities of both endo and exogenous female hormones being significant risk factors.4,5 Meanwhile, a subject of increasing interest is determination of potential relationship between the remedy of fertility and BC development.6 Given the widespread use of treatments, the investigation of the association between risk of cancer and fertility drugs is at utmost importance. Moreover, it is estimated that there are one million in vitro fertilization (IVF) cycles annually, and an unknown number of ovulation induction cycles are carried out worldwide.7,8 There are different types of medications used for the treatment of fertility (gonadotropins, clomiphene citrate, and letrozole). Gonadotropins include human chorionic gonadotropin (hCG), luteinizing hormone (LH), and follicle-stimulating hormone (FSH), and for the initiation of ovarian stimulation (OS), these gonadotropins directly bind to ovarian follicular cell receptors.9 However, controversies still exist in terms of the impact of hCG on BC risk. Furthermore, during pregnancy, placental hCG hormone is considered with antitumor effects, whereas ectopic hCG promotes progression of tumors.10 Meanwhile, clomiphene citrate plays a critical role in the inhibition of the negative feedback of gonadotropin release, leading to increased estrogen production and ovulation induction.9
Letrozole is an aromatase inhibitor, which limits estrogen production and triggers ovulation to inhibit the negative feedback of FSH and is considered the first-line remedy for hormone receptor-positive BC.9,11 However, it is still unclear that the letrozole, when combined with other fertility medications, has a risk for the development of BC. Meanwhile, female reproductive disorders, including infertility have increased, which made it a significant public health concern. Consequently, the safety of hormone-related medications, particularly OS drugs, which are mainly used medications to treat infertility.12 Therefore, this review aims to comprehensively understand the relationship between infertility medications and the risk of BC in females. The results of this study conclusively demonstrate the absence of an increased risk of BC associated with fertility treatment, which is a significant contribution to the fields of women’s health policy, clinical decision-making, cancer research, and patient education and empowerment.
Methods
Updated guidelines of preferred reporting items for systematic reviews and meta-analysis (PRISMA) and Cochrane handbook were followed for transparency and reproducibility of the studies.13,14
Literature search and data collection
The literature was searched using different electronic databases, such as PubMed, Scopus, Embase, The Cochrane Library, and Web of Sciences utilizing the following search terms: hormonal therapy, infertility, hormonal fertility treatments, and BC.
Eligibility criteria and selection of studies
For the selection of the studies, PICO guidelines were followed, P (population): the population consisted of females with fertility issues; I (intervention): the intervention involved hormonal fertility treatments; C (control/comparator): the comparator was a control group; and O (outcomes): the incidence of BC and impact of medication on fertility. In addition, randomized controlled trials (RCTs) and non-RCTs (including cross-sectional, retrospective, and cohort studies) published in peer-reviewed journals during 2003-2023 were included. Likewise, certain exclusion criteria were also considered before the selection of the studies. For instance, non-PICO studies, reviews, editorials, commentaries, letters, and studies published in non-peer-reviewed journals published before 2003 were excluded.
Duplicate studies were removed using the EndNote software. The screening process was carried out using PRISMA flowchart and initially involved reviewing the titles and abstracts, followed by full-texts, which were carried out by 2 independent authors. Any discrepancies between authors were resolved by a third senior author.
Data extraction
The data comprised the following components: I) summary characteristics, which encompassed women experiencing fertility issues and undergoing hormonal fertility treatments; II) baseline data, including the location of the study, study design, publication year, primary outcomes, and conclusions; and III) outcomes that featured the incidence of BC among females receiving hormonal fertility treatments, along with the odds ratio (OR) or risk ratio (RR) or hazard ratio (HR) and confidence interval (CI).
Data analysis
To analyze the extracted data from the included studies, RevMan software (Version 6.0) was employed along with the Generic Inverse Variance method, which is suitable for studies with varying sample sizes and standard errors across multiple studies. Most studies employed the RR or OR to gauge the impact of infertility medications on the incidence of BC (8 studies). However, 4 studies used HR as their estimation method, as they employed person-time years and carried out a time-to-event analysis. The analysis was based on 2 measures: RR and OR. As the conversion of OR to RR is relatively simple, particularly when the prevalence of the outcome is less than 10%, the 2 were analyzed together. However, the conversion of HR to RR was more complex and required information on the shape of the survival function, which was not available in the included studies. As a result, studies that used HR were analyzed separately (4 studies). A forest plot was constructed for all included studies using both random and fixed models to carry out sensitivity analysis and compare the findings. The I2 values and Chi-square statistics were used to evaluate heterogeneity at the significance level of <0.05.
Results
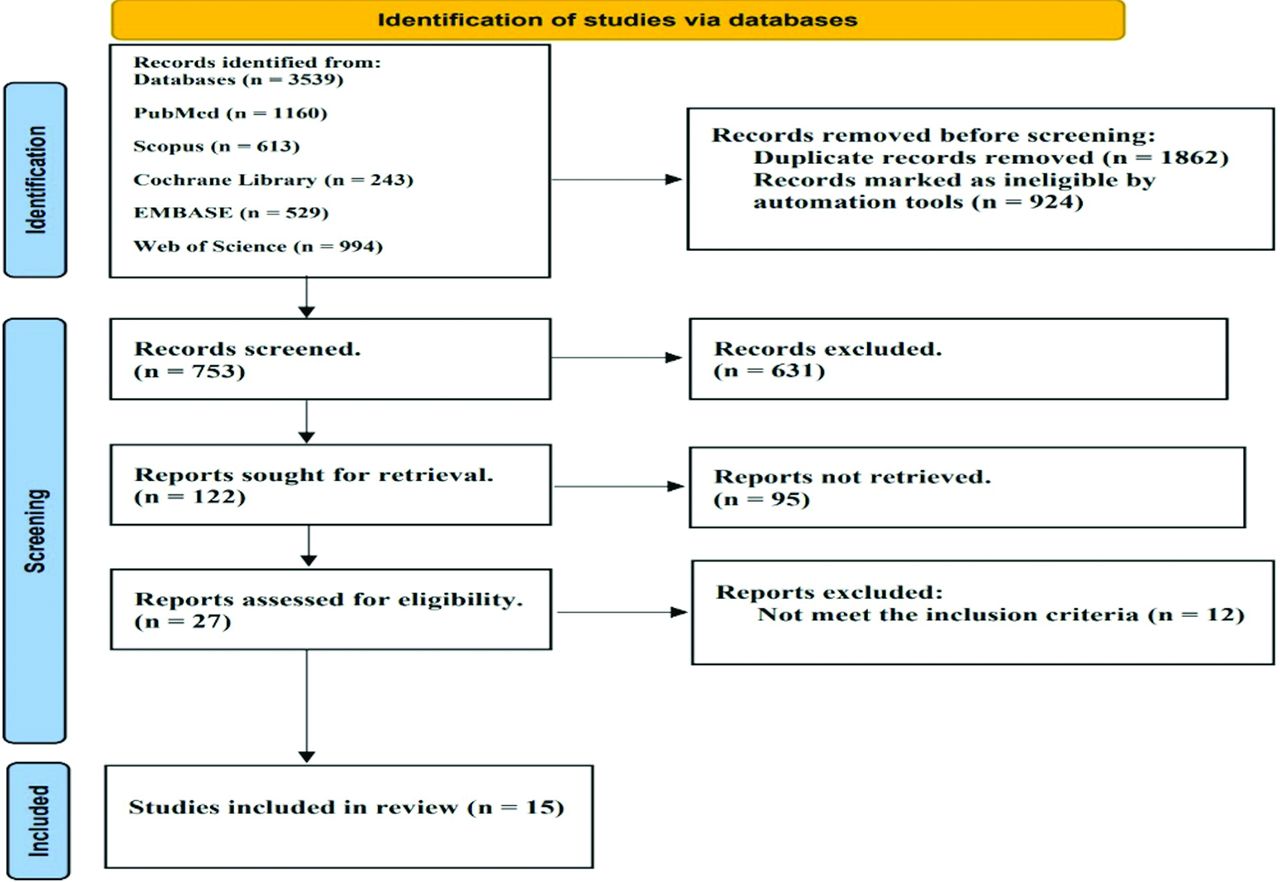
Figure 1 depicts the process of identification and selection of studies for this systematic review. Initially, 3,539 records were identified from the following databases: PubMed (n=1,160), Scopus (n=613), The Cochrane Library (n=243), EMBASE (n=529), and Web of Science (n=994). After removing duplicates (n=1,862) and 924 records were found ineligible by automation tools (n=924), 753 records were screened. Of these, 631 reports were excluded, leaving 122 records for retrieval. An additional 95 records were not retrieved, leaving 27 assessed for eligibility. After excluding 12 records that did not meet the eligibility criteria, 15 records were ultimately selected in the review for further qualitative and quantitative analysis.

- Preferred reporting items for systematic reviews and meta-analyses flow diagram. Process study selections through databases.
Summary study characteristics
Table 1 summarizes the studies, which evaluated the association between fertility treatment and BC risk in various populations across different countries. A study from Taheripanah et al15 used ovulation drugs for the treatment of infertility and observed no association with BC risk, except for a rise in risk with use exceeding 6 months. Likewise, Orgéas et al16 found no evidence for increased overall BC risk with infertility treatment, however, increased risk of BC was linked with high-dose of clomiphene citrate for nonovulatory causes. Furthermore, Calderon-Margalit et al17 observed a significant association between overall risk for cancer with ovulation induction, however, lacked understanding of treatment details. Furthermore, Lerner-Geva et al18 found no increased ovarian cancer risk with infertility treatment and attributed higher borderline ovarian tumor risk to inherent tumor traits or surveillance bias. Bildircin et al19 found no BC risk from controlled OS and advocated for anti-estrogen agents, GnRH antagonists, and awareness of lower ovarian reserves in patients with cancer.
- Study characteristics (N=15).
A study from Basudan et al20 attributed the rising BC incidence to lifestyle changes and called for preventive measures, such as addressing tobacco use and improving screening. In France, Gauthier et al21 found the effect of fertility treatment on the incidence of BC unclear, but observed a potential role played by family history. Moreover, Kotsopoulos et al22 found no increase in BC risk from fertility treatment in carriers of BRCA mutations. Likewise, Jensen et al23 found no link between fertility drug use, cycles, or years since first use and BC overall, but possibly an effect in nulliparous women. While, Reigstad et al24 demonstrated higher BC risk after assisted reproduction versus no treatment. However, Burkman et al25 suggested prolonged medication use may increase risk. Meanwhile, Terry et al26 found a lower risk of ovulatory disorders versus other infertility causes. Similarly, Stewart et al6 associated younger IVF age with a greater risk of BC. While, Doyle et al27 demonstrated that ovarian stimulation had no risk of cancer development, and Cooley28 suggested estrogen treatment had an indirect effect on BC cells (Table 1).
Meta-analysis using the risk ratio
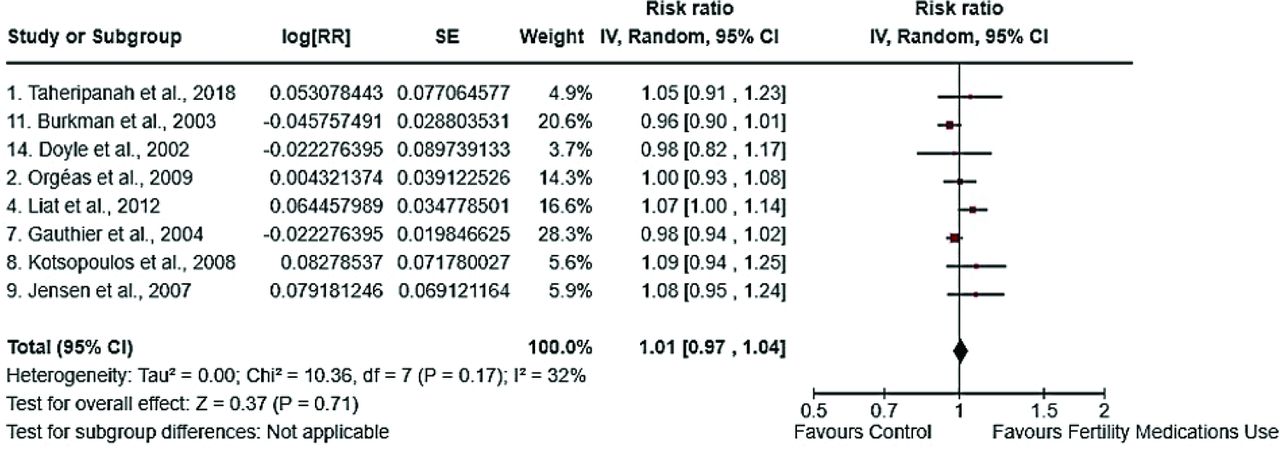
Figure 2 shows a pooled effect size of 8 studies and revealing an overall RR=1.00, p=0.83. The RR for the association between infertility medications and BC in women was (RR=1.0, 95% CI: [0.97-1.02]), according to the fixed effect model. This suggests that there is no evidence to support the notion that infertility medications increase risk of BC in women.

- The influence of infertility medications on breast cancer risk in women was assessed using a fixed effects model.
Meta-analysis (random effects model)
The level of heterogeneity, as indicated by the I2 statistic, was low (32%) and the Q test was not statistically significant. Sensitivity analysis was carried out via random-effects model for the assessment of the heterogeneity, which has an impact on our findings (Figure 3). The findings of this analysis were consistent with those of fixed-effects model, suggesting that there is currently no evidence to underpin and establish the notion that infertility medications increase the risk of BC.

- The impact of infertility treatments on a woman’s likelihood of developing breast cancer using a random effects model.
Meta-analysis using hazard ratio
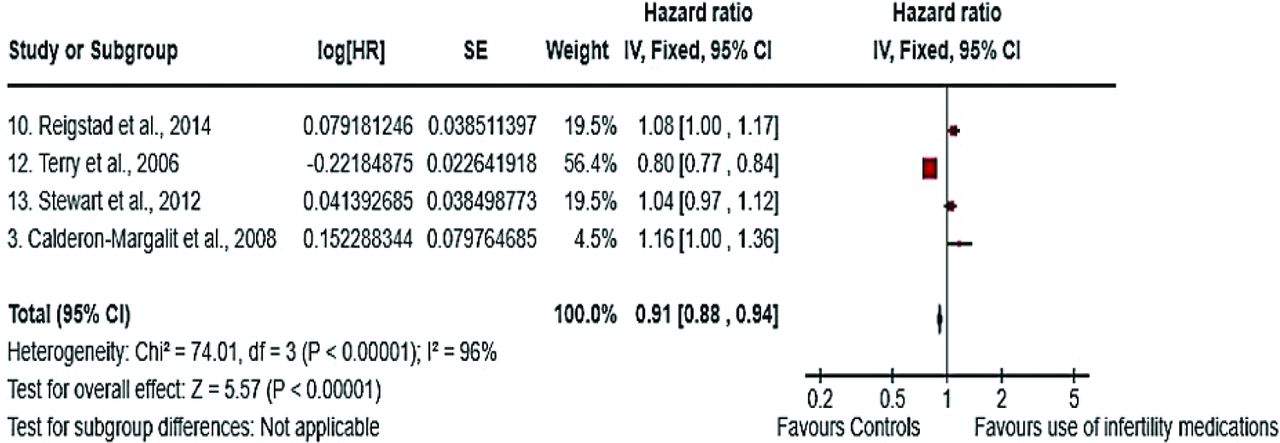
The degree of heterogeneity was substantially high, as indicated by the I2 value (96%), and the Q test demonstrated statistical significance. This suggests the presence of heterogeneity, which may be attributed to the following factors, such as differences in patient clinical characteristics or variations in statistical methodologies among the studies. A sensitivity analysis was carried out by employing either fixed- or random-effects models. Figure 4 illustrates a forest plot depicting all assessed studies utilizing the model (fixed-effects) to determine the effect size. The HR for the overall analysis is indicated by the black diamonds in the figure. The HR estimated at 0.91 (95% CI: [0.88-0.94]) revealed significant reduction in BC risk in women, who used infertility medications than those with no medications (p<0.001). This analysis employs time-to-event data, accounting for the risk among women during non-follow-up periods.

- Forest plot for hazard ratio to assess the impact of infertility treatments on women’s susceptibility to breast cancer, specifically examining the fixed effects model.
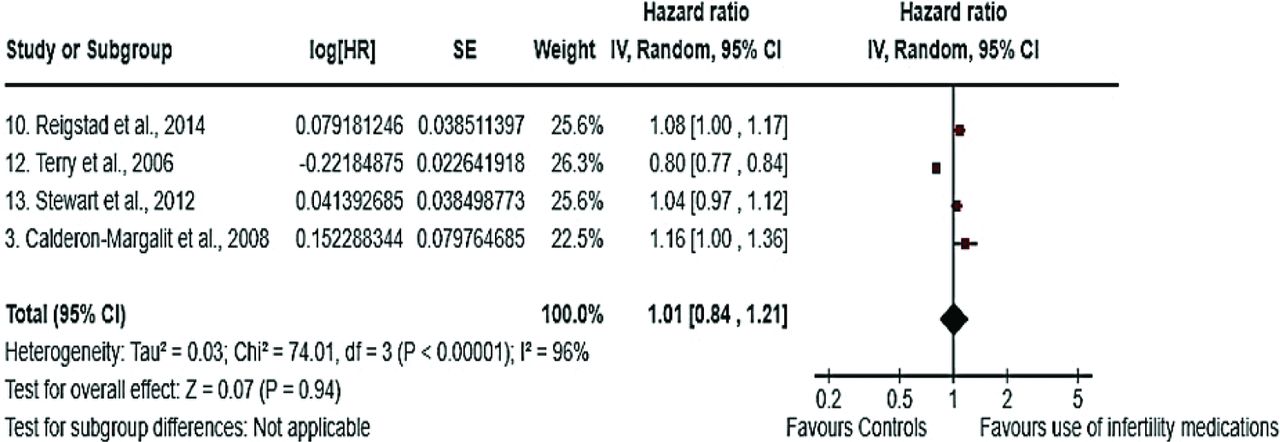
Meta-analysis using random effects model and hazard ratio
By employing the random-effects model in Figure 5, it was observed that heterogeneity remained constant, suggesting that source of heterogeneity was attributable to the methods utilized in the included studies rather than being a result of statistical heterogeneity. The overall effect, as determined by the HR, was 1.01 with non-significant difference (p=0.94). Consequently, the use of the random-effects model in this instance was not beneficial as it led to the loss of statistical significance, while the heterogeneity remained unchanged.

- The impact of infertility treatments on the likelihood of breast cancer in women can be analyzed using a random-effects model and hazard ratio.
Discussion
The incidence of BC following hormonal treatment for infertility, as with all gynecological cancers poses significant threat to the overall health of women and also considered as a leading cause of mortality among women worldwide and has serious implications for public health.30,31 Therefore, this meta-analysis aimed to compare medications used for fertility and their role on the BC development.
The safety of hormone-containing fertility treatments for OS has garnered significant attention; however, evidence supporting their safety remains limited.12 Numerous studies have explored the connection between exogenous hormones and BC; however, the association between infertility treatment and BC remains unclear. Evaluating BC risk is particularly challenging for women seeking treatment for fertility in their early age of life (20s and 30s), and in the later stage of life (3-4 decades), the peak incidence of BC occurs.32 Although the incidence of BC and its associated deaths increases with age, this association remains unclear.
One of the key difficulties in investigating the impact of the treatment for fertility on BC risk is the confounding factors, which are the underlying causes of infertility. As, infertility and nulliparity are considered as the risk factors for BC, and the effect may be unreliable when checked with the general population.33
Our results demonstrated a non-significant impact of treatments used for fertility on the increase risk of developing BC among women. Our findings are in consistent with the another meta-analysis, which was carried out in the general female population. Furthermore, fertility therapy did not significantly increase the BC incidence in genetically vulnerable women, or in women with BRCA mutations, and those with a family history of BC. In addition, lower mortality rate was observed in women assessed for infertility than the general population.12,34 Furthermore, another meta-analysis also observed similar findings and revealed non-significant risk of BC development with fertility treatment and compared with subfertility or general population as a reference group. The OR was 0.97 (95% CI: [0.90-1.04]) and even women administrated with 6 or more IVF cycles did not develop or show the risk of BC development.35 Moreover, another study also demonstrated a non-significant relationship between BC and IVF in general population with 0.91 RR (95% CI: [0.74-1.11]), while in infertile women RR was 1.02 (95% CI: [0.88-1.18]).36 Likewise, a cohort study included 25, 108 women and treated with IVF and compared with general population for the risk of development of BC. This study observed non-significant difference with 1.01 standardized incidence ration (SIR, 95% CI: [0.93-1.09]) for general population and for non-IVF group HR was 1.01 (95% CI: [0.86-1.19]).37 In contrast, research has demonstrated that women who undergo assisted reproductive technology (ART) have a 20% higher risk of developing BC.24 Meanwhile, a question can arise that how these fertility medications cause BC and the possible explanation can be that with the fertility medications stimulate ovarian activity, leading to elevated levels of progesterone and estrogen hormones, which play an important role in breast tissue proliferation.38 In addition, prolonged or repeated exposure to high level of these hormones can enhance and increase cell division in breast tissue, potentially heightening the risk of tumor formation.39 Overall, this study highlights the non-significant impact of fertility treatment on the risk of development of BC. However, clinically the outcomes of the present study should be used with caution as it is also established that with high dose or duration of these treatments can increase risk of BC.
Future studies should focus on large scale, long-term cohort studies with robust design for better comparison and further elucidate the association between fertility treatment and risk of BC. In addition, studies should incorporate treatment type, dose, cycles, and duration and most importantly confounding factors, such as age, lifestyle factors, genetic predisposition, and history.
Study limitations
This review was characterized by several robust features and limitations. The studies included in our review were primarily observational and retrospective, and cohort studies were retrieved from national databases. These databases are prone to information and recall bias, which may affect the accuracy of the collected data. Additionally, the data often lacked key variables, such as HRT exposure, BMI, family history for cancer or BC, smoking, alcohol consumption, and age at menarche, which are considered utmost and significant risk factors and potential confounders for developing BC.
In conclusion, this review did not provide concrete evidence to support a connection between the hormonal medications use for infertility treatment and an BC development risk in women. Although this systematic review indicates that fertility medications did not appear to increase the risk of BC, however, it is challenging to definitively prove the absence of any association because of the variety of existing studies and the need for thorough, long-term registry studies that account for confounding factors. Therefore, the results of this study are useful for guiding clinical practice and patient counseling. However, further research is necessary to monitor BC incidence after infertility treatment.
Acknowledgment
The authors gratefully acknowledge Research Medics (https://researchmedics.com/) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 1, 2024.
- Accepted March 12, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.