


ABSTRACT
Objectives: To compare the efficacy and safety between 2 endoscopic surgical approaches for early gastric cancer: pocket creation method of endoscopic submucosal dissection (PCM-ESD) and conventional ESD (CM-ESD).
Methods: A comprehensive literature search was carried out in PubMed, China National Knowledge Infrastructure, and the Cochrane Library from their inception to July 2024 using medical subject headings and free-text terms, which were “pocket-creation method”, “gastric cancer”, “gastric neoplasms”, and “endoscopic submucosal dissection” or “ESD”. Two independent reviewers carried out the search, screened studies, and extracted data.
Results: A total of 578 cases were included in our study, which sourced from 2 randomized controlled trials and 5 retrospective cohort studies. Among them, 258 cases were in the intervention group that received PCM-ESD, and 320 cases were in the control group that received CM-ESD. The PCM-ESD demonstrated a significantly faster dissection speed (mean difference=5.57 mm²/min; 95% confidence interval: [4.24-6.91]; p<0.00001) and shorter procedure time compared to CM-ESD. The incidence of intraoperative perforation in the PCM-ESD group was notably lower than that in the CM-ESD group. In terms of complete resection, R0 resection, or delayed bleeding, the 2 groups had no significant differences.
Conclusion: For endoscopists, the use of PCM in early gastric cancer seems to be superior to CM-ESD in terms of dissection speed and the procedure time, and got a lower incidence of perforation. Moreover, there was no discernible difference between the 2 groups’ rates of en bloc and R0 resection, and the use of PCM-ESD did not increase the chance of delayed bleeding.
PROSPERO No. ID: CRD42024564118
Gastric carcinoma is a malignancy, which originating from the gastric mucosa, currently ranking fourth in global incidence and second in mortality worldwide.1 The early symptoms of stomach cancer may not be obvious, and most of the patients have already entered the progressive stage when they are diagnosed. Benefiting from the popularity of digestive endoscopy, the chances of detecting early gastric cancer are increasing year by year.
Recently, endoscopic submucosal dissection (ESD) has been widely used for early superficial gastrointestinal tumors, becoming one of the standard endoscopic surgical techniques.2 Compared to surgery, ESD demonstrates distinct advantages: its minimally invasive results in reduced tissue trauma, accelerated postoperative recovery, and preservation of gastric function. This endoscopic approach not only significantly enhances patients’ postoperative quality of life but also substantially decreases healthcare costs associated with hospitalization.3 However, the wide lumen and complex structure of the stomach make it sometimes difficult to carry out ESD operations on the gastric, especially in special areas such as the gastric angle and the pyloric ring.4 Various methods, including traction-assiste, double-channel endoscopic, and the pocket creation method, have been reported to be used during ESD to conquer these obstacles and produce some profitable results.5,6
The pocket creation method of endoscopic submucosal dissection (PCM-ESD), which was first introduced by Yamamoto’s group in 2014, was developed for the resection of superficial colorectal neoplasms.7 The core feature of the PCM-ESD technique is that it uses a tiny incision to construct a large-scale submucosal tunnel for operation, avoiding the circumferential incision procedure in traditional ESD. Several studies in colorectal lesions have demonstrated superior en bloc and R0 resection outcomes with PCM-ESD compared to conventional ESD (CM-ESD), as well as reduced adverse events.8,9 Research carried out by Pei et al’s10 team has demonstrated that PCM-ESD exhibits statistically significant advantages over CM-ESD in both clinical efficacy and safety metrics. There have also been recent studies aimed at evaluating the usefulness of PCM for ESD of superficial gastric tumors.11 But the cases in the literature are relatively few. This meta-analysis evaluates the comparative effectiveness and safety of PCM-ESD versus CM-ESD, aiming to consolidate current evidence and inform clinical practice.
Methods
This meta-analysis was carried out at the Rizhao People’s Hospital in 2024. A systematic literature search was carried out from July 2024, across China National Knowledge Infrastructure, PubMed, and Cochrane Library databases, covering publications from their inception to 2024. The literature was searched using the medical subject headings and keywords such as “pocket-creation method,” “gastric cancers,” “gastric neoplasms,” and “endoscopic submucosal dissection” or “ESD”. Two independent reviewers (Wang and Song) screened and evaluated studies to minimize selection bias.
This study strictly followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) reporting guidelines.12
Inclusion criterion
I) population: patients diagnosed with early gastric cancers and undergoing ESD; II) intervention: PCM-ESD; III) comparison: CM-ESD; IV) outcome measure: the R0 resection rate, en bloc resection rate, dissection speed, procedure time, and perforation and delayed bleeding; and V) study design: all types of studies.
Exclusion criterion
Studies that I) did not provide clear results or enough data for analysis; II) used non-primary research forms (such as case reports, reviews, or conference abstracts); or III) did not have a control group for comparison were excluded.
Data extraction
Song and Wang systematically screened the database, followed by a rigorous quality assessment of the eligible studies. Disagreements were discussed. From each of the chosen studies, the following key data were taken out: first author, study period, country, year of publication, kind of study, gender, age, number of patients, tumor location and size, and macroscopic type (Table 1). The outcomes are detailed in Table 2.
- Characteristics of the included studies.
- Characteristics of the included studies (continuation).
- Outcomes of clinical observation indicators in the included studies.
Risk of bias analysis in the analyzed trials
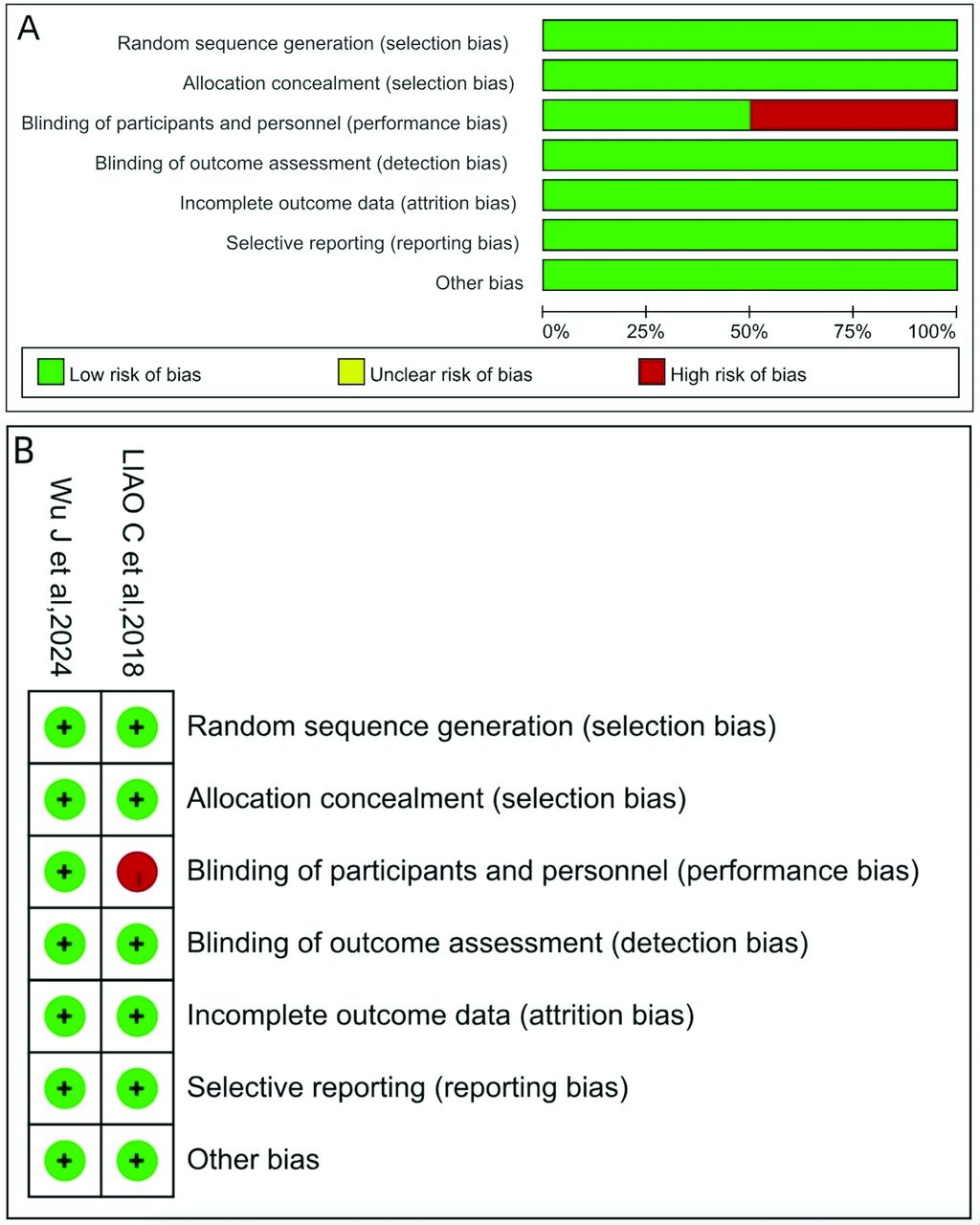
The 2 randomised controlled trials (RCTs) were assessed by us using the criteria of the Cochrane risk of bias assessment tool.13 A total of 7 domains were assessed, resulting in bias risk classifications of low, uncertain, or high. The results are presented in Figure 1. There was a high risk of bias in one of the RCT because the endoscopy was not blinded to the ESD procedure. However, the other risks were all classified as low. Another RCT was considered low risk. A total of 5 retrospective studies were assessed using the Newcastle Ottawa scale, which includes research object selection, intergroup comparability, and outcome indicators (Table 3). All 5 retrospective studies received a score of >7 in a quality assessment based on the Newcastle-Ottawa scale and were classified as high-quality studies.

- The Cochrane risk of bias assessment tool was used to evaluate the included articles’quality. A) Risk of bias graph; B) risk of bias summary.
- Quality evaluation of the included articles using the Newcastle-Ottawa scale.
Statistical analysis
The analysis was carried out using Review Manager 5.4 software, which was developed by The Cochrane Collaboration, Copenhagen, Denmark, for 6 outcomes. The Mantel-Haenszel approach was applied for data synthesis. Dichotomous variables (namely, the R0 resection rate, adverse events) were expressed as odds ratios (OR) with 95% confidence intervals (CI), whereas continuous variables (namely, dissection speed, procedure time) were reported as mean differences (MD) with 95% CI. The results were displayed using forest plots, and heterogeneity was evaluated via the I² statistic. A p-value was defined as statistically significant if <0.05.
Results
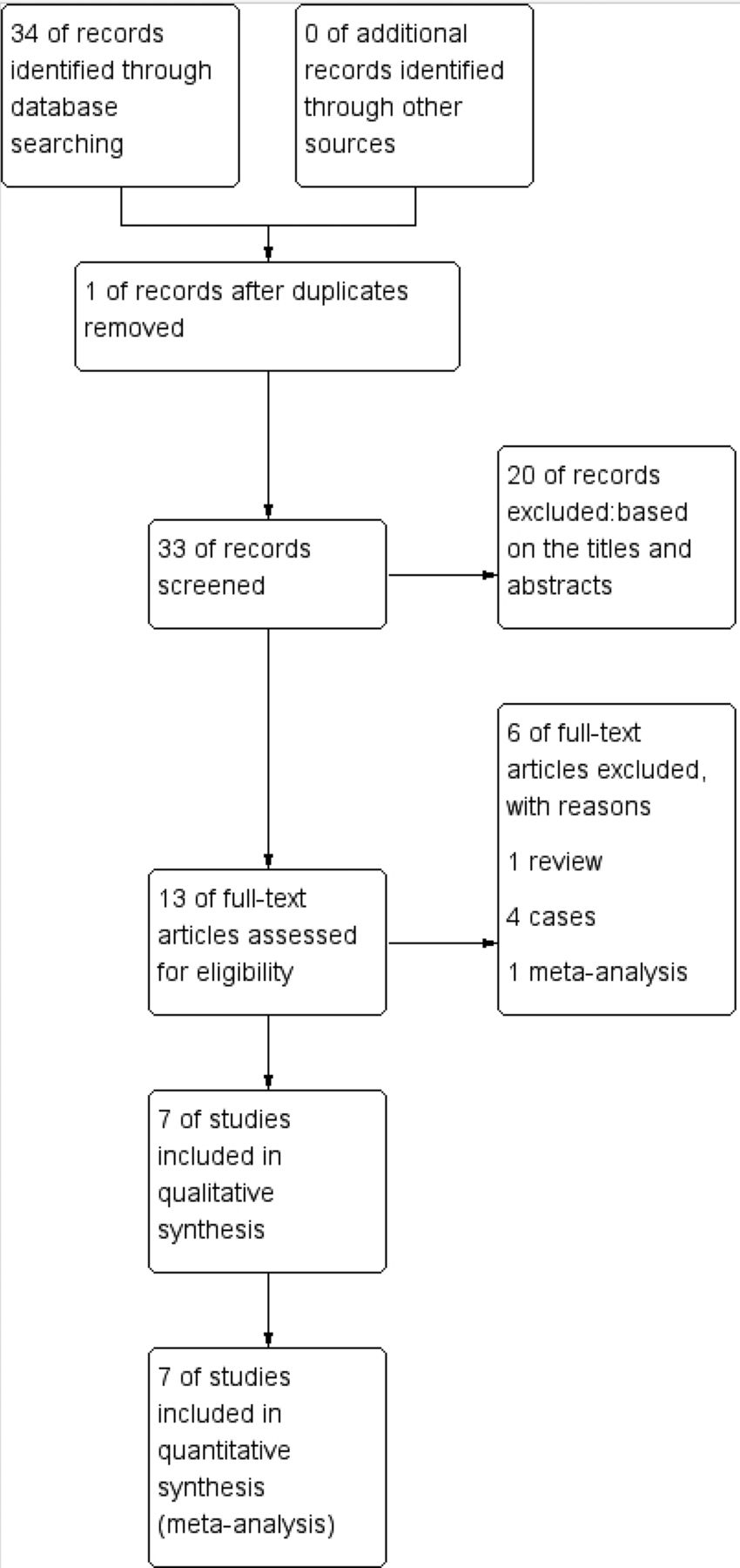
This review included 2 RCTs and 5 retrospective analyses.14-20 The publication dates of the studies were between the years 2018-2024. The literature screening and inclusion process is illustrated in Figure 2. Which comprised 578 participants, with 258 undergoing PCM-ESD and 320 receiving CM-ESD.

- Flow diagram of study selection.
The R0 resection rate
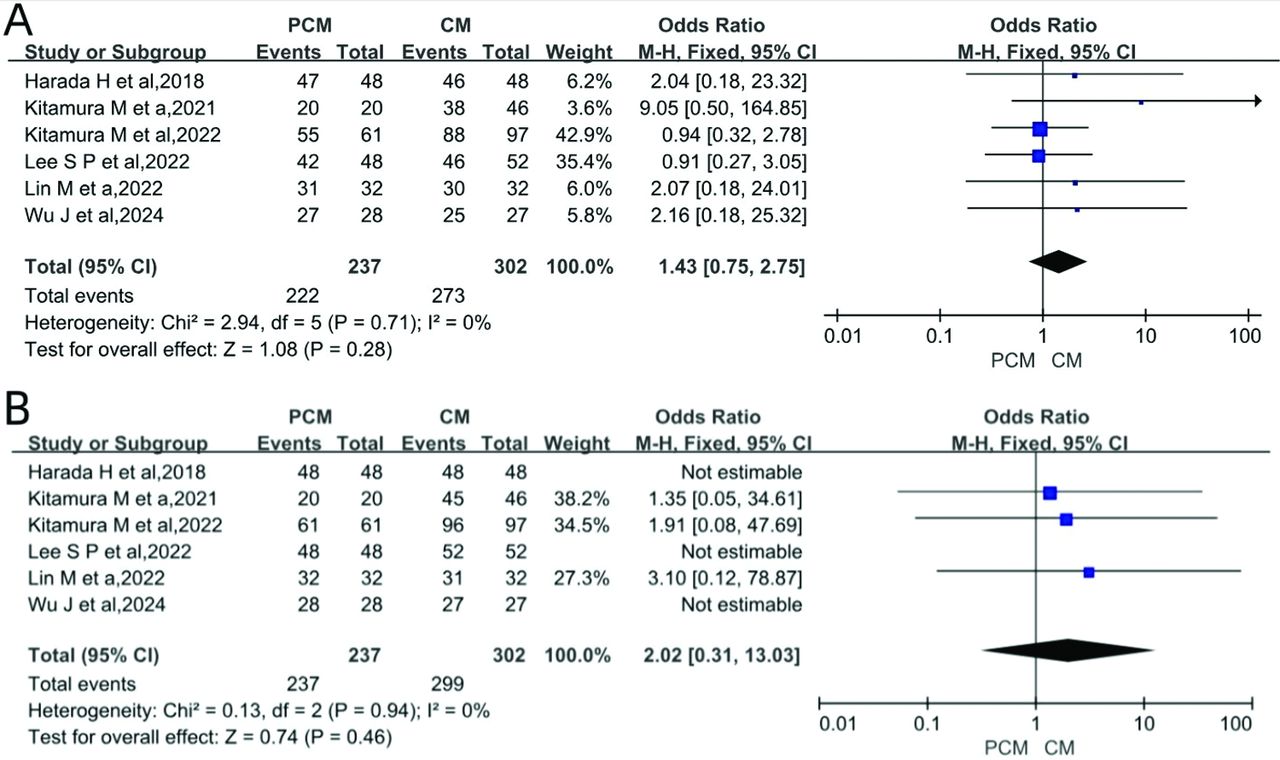
The rate of R0 resection was reported in 6 articles. Using the I2 statistic, we assessed these 6 trials and discovered no heterogeneity (I2=0, p=0.71). The study found no statistically significant gap in R0 resection outcomes (p=0.28, Figure 3A displays forest plots).

- Forest plots comparing PCM-ESD to CM-ESD. A) Forest plot of the R0 resection rate; B) forest plot of the en bloc resection.
The rate of en bloc resection
A total of 6 studies reported en bloc resection rates. No heterogeneity exists (I²=0%, p=0.94). The study found no statistically significant gap in en bloc resection rates (OR=2.02; 95% CI: [0.31-13.03]; p=0.46), as depicted in the forest plots Figure 3B.
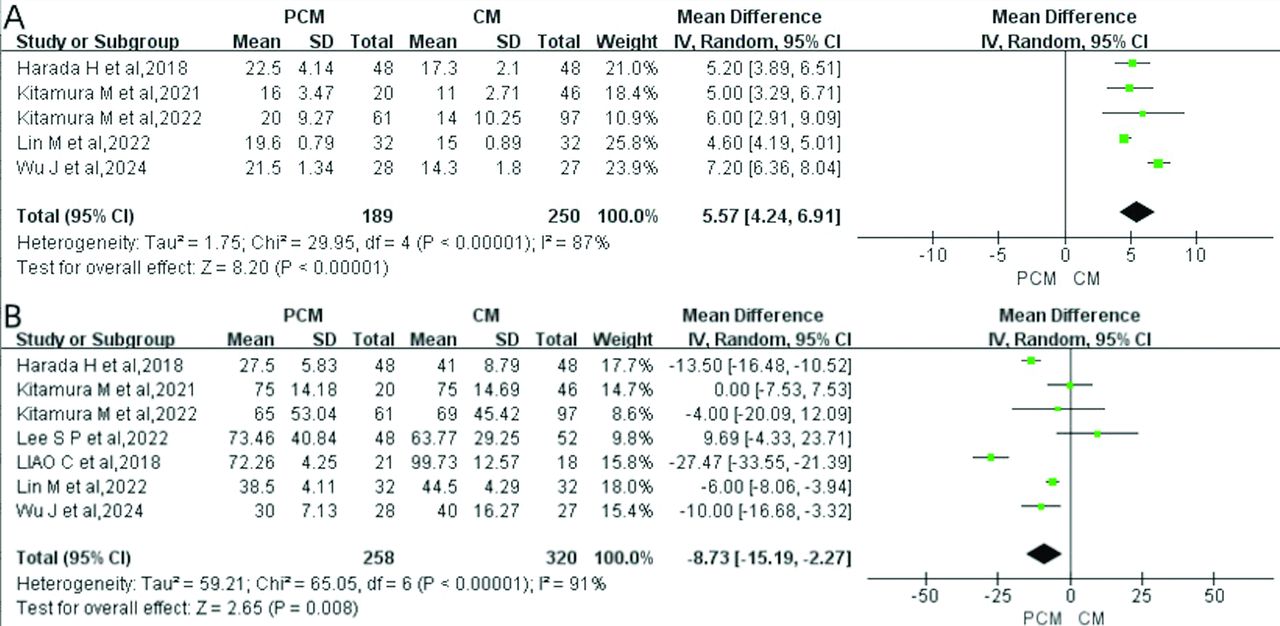
Dissection speed
A total of 5 studies evaluating dissection speed revealed significant heterogeneity across the articles (I²=87%, p<0.05). The pooled results demonstrated a statistically significant increase in dissection speed (mm²/min) with PCM-ESD (MD=5.57; 95% CI: [4.24-6.91], p<0.00001). Forest plots illustrating these findings are presented in Figure 4A.

- Forest plots comparing PCM-ESD to CM-ESD. A) Forest plot of dissection speed; B) forest plot of procedure time.
Procedure time
All 7 included studies reported procedure time, with significant heterogeneity detected across the studies (I²=91%, p<0.05). Furthermore, procedure time is also one of the most important indicators of ESD. In this respect, CM-ESD has a significant disadvantage by comparison with PCM-ESD in terms of procedure time, with a mean difference of -8.73 (95% CI: [-15.19 to -2.27]; p=0.008), as shown in the forest plots Figure 4B.
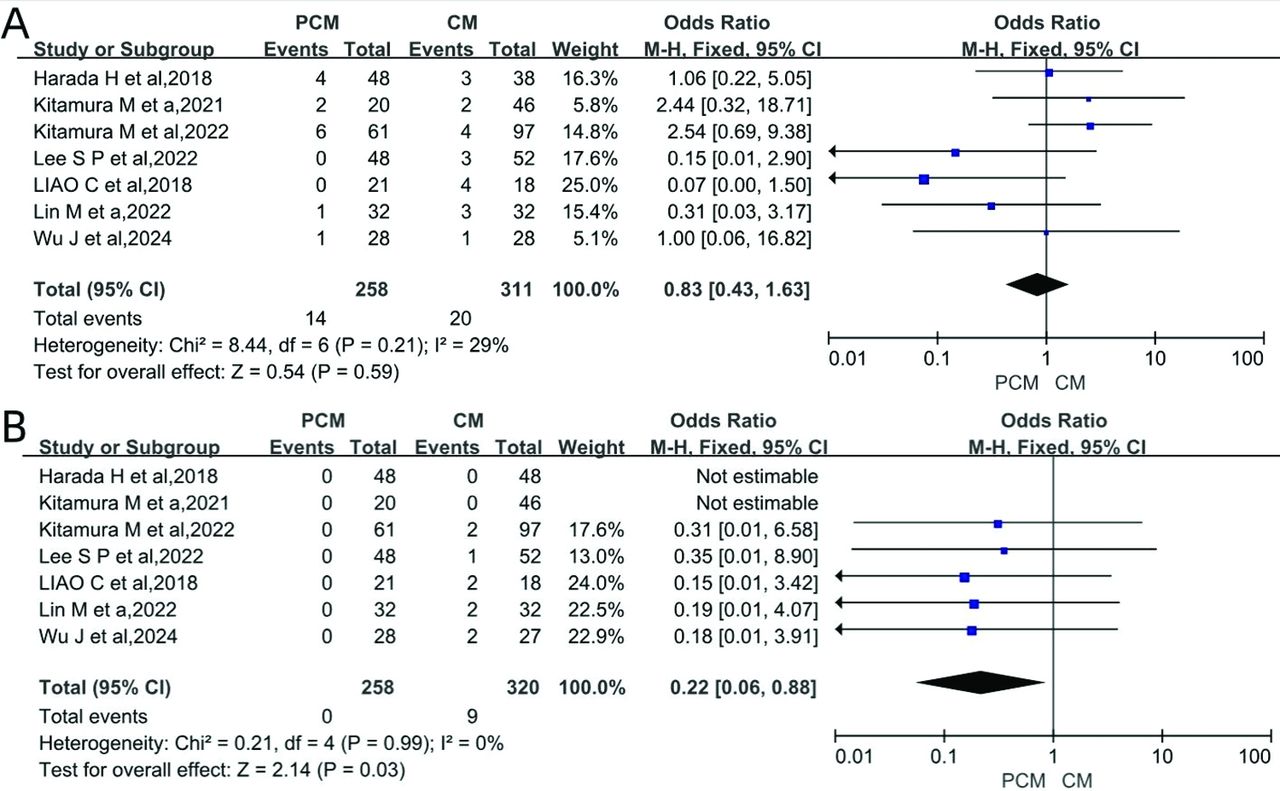
Delayed bleeding
All 7 articles included in the analysis reported data on the incidence of delayed bleeding. Forest plots (Figure 5A) showed that there was no substantial gap in rates of delayed bleed (OR=0.83; 95% CI: [0.43-1.63], p=0.59).

- Forest plots comparing PCM-ESD to CM-ESD. A) Forest plot of delayed bleeding; B) forest plot of perforation.
Perforation
All 7 articles articles reported the incidence of perforation. No heterogeneity exists (I2=0, p=0.99). In our statistical analysis, among the 578 patients, PCM-ESD had a significantly lower perforation rate (OR=0.22; 95% CI: [0.06-0.88], p=0.03, forest plots shown in Figure 5B).
Sensitivity analysis
We carried out a sensitivity analysis by eliminating articles one by one, as there was obvious heterogeneity in terms of dissection speed and procedure time, and there was no significant change in heterogeneity. This was a reflection of the stability of the results.
Publication bias
We analyzed publication bias using funnel plots and found that the scatter plot was symmetrical on both sides, which suggests that there is no publication bias.
Discussion
Japanese endoscopists at Jichi Medical University developed a novel endoscopic technique called the PCM-ESD.7 The main procedure is to first cut the mucosa on one side of the lesion to create the pocket opening, peel along the opening pocket under the submucosa to the other side of the tumor, and then incise the mucosa on the remaining 2 sides of the lesion to remove it completely.
The small caliber tip transparent (ST) hood contributes enormously to the effectiveness as well as safety of PCM-ESD.7 It is an essential tool in PCM to facilitate entry and provide adequate traction and countertraction in the pocket. By pressing on the tissue, it promotes countertraction, generating tension that promotes submucosal dissection and lessens accidental damage to the muscle tissue. The ST hood is crucial in PCM-ESD to accomplish en bloc excision of lesions while putting patient safety first since it overcomes visualization and access issues, unlike bulkier hoods.
As one of the newer methods of ESD treatment, PCM-ESD provides a self-traction effect generated by mucosal flaps. The PCM offers 4 major advantages: I) a small inlet prevents leakage of the injected solution, avoiding unnecessary repeat injections; II) both traction and countertraction are obtained when inciseing the mucosa; III) can switch between a vertical and tangential approach to the muscularis, ensuring complete peeling of the vertical and horizontal margins of the lesion, and a high-quality pathology specimen is obtained; and IV) the effect of cardiopulmonary movement is diminished as a result of the synchronization of the endoscope and the pocket.21 These advantages minimize the technical difficulties involved in ESD for early gastric cancer. Previous studies have shown that PCM-ESD can effectively eliminate lesions without requiring specialized technical knowledge or expertise.8
A meta-analysis of PCM-ESD in colorectal cancer suggests that PCM takes less time to carry out and is faster to dissect, fully demonstrating the superiority of the pocket method.10 Early-stage gastric cancer has also seen extensive use of PCM-ESD.
According to a single-center retrospective study, PCM-ESD outperformed CM-ESD in terms of dissection speed for early gastric cancer. It has been demonstrated that PCM-ESD exhibits a superior dissection speed in comparison to CM-ESD, according to our statistical study. Faster dissection speed saves surgical time. All 7 articles reported the procedure time. According to our statistical analysis, the procedure time via PCM-ESD is shorter than CM-ESD. Despite the reduction in operative time, there was significant heterogeneity (I2=91%). The reasons for this may include differences in the experience of the operators. Procedural success and complication rates are strongly influenced by operator expertise, experienced operators may be more effective and have fewer adverse events than novices, which is an important factor that may account for the observed differences in outcomes, particularly dissection speed and procedure time. PCM-ESD requires advanced skills, and experience may have an impact on the results.
The requirement to obtain en bloc resection is another important consideration in the choice of endoscopic resection method.22 En bloc resection and R0 resection are 2 important assessment indicators of early gastric cancer recurrence. In endoscopic mucosal resection (EMR), a treatment modality in which endoscopic resection is accomplished by segmentation rather than en-bloc is called endoscopic piecemeal mucosal resection (EPMR). The disadvantage of piecemeal resection is that it increases the difficulty of pathological evaluation compared to en-bloc resection. The more segments there are, the more difficult it is to assess whether complete resection of the margins of the lesion has been achieved, making it difficult to assess whether curative resection has been achieved and whether additional follow-up is required, thus delaying the timing of treatment.23
The 6 included studies did not show a notable difference in en bloc resection between the 2 groups. An R0 resection is essential for curative resection, and the 2 groups did not differ significantly in the R0 resection either.
The safety of ESD is especially important, perforating and bleeding are the major adverse events associated with ESD.24,25 Delayed bleeding is an adverse event that typically happens within 24 hours of ESD and is characterized by clinical signs including blood in the vomit and black stools along with a drop in hemoglobin, with an incidence of approximately 5-8%.26 Perforation is a serious adverse event that occurs after ESD with symptoms such as fever and abdominal pain and usually requires re-surgical treatment.27 Imaging studies, such as CT scans, can reveal the presence of fluid accumulation and abnormal air in the gastrointestinal tract.28 All 7 studies included in the analysis documented perforation incidence, and our statistical analysis of the 578 patients showed that, in contrast to CM-ESD, PCM-ESD was linked to a decreased perforation rate. The PCM provides an optimal submucosal view, which circumvents the necessity for deep peeling and, as a consequence, markedly diminishes the probability of perforation. Delayed bleeding increases the cost of hospitalization. All 7 of the articles included in the analysis reported cases of delayed bleeding, but there was no statistically significant difference in the incidence between them.
Our meta-analysis has several advantages. First, all 7 of the included studies were of high quality. Only one RCT was found to have high blinding bias, but this is unavoidable. Following a rigorous evaluation, the 5 cohort studies were deemed to be of a high standard. based on subject selection, comparability between groups, and outcome indicators. Second, most of the results showed very little heterogeneity, with the exception of process time and dissection speed.
Study limitations
Due to heterogeneity in terms of dissection speed and procedure time, we were unable to obtain sufficient data in the included studies for subgroup analysis or meta-regression. With the exception of the 2 papers by Kitamura et al,17,18 which were carried out at the same institution, the other studies may have differed in methodology, such as Harada et al,19 who used water-pocket endoscopic submucosal dissection. And the ST hood is not used in PCM in the study of Lin et al.15 This variability could contribute to heterogeneity in outcomes.
In addition, endoscopist experience was not consistently available across studies, which is a limitation of the current evidence base and may affect the generalisability of our findings, highlighting the need for standardised reporting in future studies. We recommend that future studies explicitly report endoscopist experience to better contextualise results. The study has several limitations, including the small number of RCTs (only 2) and the absence of data from countries outside Asia, as all included studies were carried out in Asian regions. These gaps highlight the need for additional good quality RCTs in different regions to support these findings in future research.
In conclusion, for endoscopists, the use of PCM in early gastric cancer seems to be superior to CM-ESD in terms of dissection speed, the procedure time, and got a lower incidence of perforation. The 2 groups demonstrated comparable outcomes in both en bloc resection and R0 resection rates, with no statistically discernible differences observed. Additionally, the PCM-ESD group showed no elevated risk of bleeding compared to the control group.
Acknowledgment
The authors gratefully acknowledge Bullet Edits Limited for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 12, 2025.
- Accepted March 23, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.