


ABSTRACT
Objectives: To describe the role of infection control measures in controlling human parainfluenza virus type 3 (HPIV-3) outbreaks in the neonatal intensive care unit of a tertiary military hospital in Riyadh, Saudi Arabia.
Methods: This single center, retrospective study collected clinical and diagnostic data from date to date. We collected nasopharyngeal swabs from symptomatic patients and processed using multiplex real-time polymerase chain reaction assays to detect HPIV-3.
Results: The HPIV-3 outbreak occurred between December 2022 and January 2023, and affected 22 patients (mean age: 13 months), among whom 18 had underlying chronic medical conditions. Most patients (n=18) presented with lower respiratory tract infections, 16 of whom required oxygen therapy. Almost all cases improved clinically except for one baby who died of holoprosencephaly. Among the symptomatic healthcare workers (n=21), only one nurse tested positive for HPIV-3. Early screening for HPIV-3, proper cohorting under isolation precautions, and the restriction of admissions and visitors, along with additional infection control measures, have been progressively implemented during the outbreak period.
Conclusion: Strict implementation of infection control approaches can contribute to limiting the spread of HPIV-3.
Human parainfluenza virus (HPIV) is an enveloped RNA paramyxovirus with types 1, 2, 3, and 4.1 The HPIV-3 is a significant cause of lower respiratory tract infections (LRTIs), accounting for over 30% of cases in young children, second only to respiratory syncytial virus (RSV).2 Outbreaks are more common in older infants, as newborns benefit from passive maternal antibodies.3 The virus spreads through direct contact, large droplets, or contaminated surfaces, with an incubation period of 3-6 days.4
Due to low clinical suspicion, viral respiratory infections are often undiagnosed or detected late.5 Current bacterial-focused diagnostic methods have low sensitivity for viral detection. The advent of multiplex reverse transcription-polymerase chain reaction (RT-PCR) has improved virus identification.6-8
In December 2022, the first HPIV-3-positive patient at Prince Sultan Military Medical City, Riyadh, Saudi Arabia, neonatal intensive care unit (NICU) presented with fever and respiratory symptoms. Initial Xpert Xpress Cov-2/Flu/RSV plus kit screening was negative, but respiratory panel testing confirmed HPIV-3. No cases had been detected in the previous 12 months. Infection control measures were implemented, but cases increased, prompting outbreak management activation. This study describes the infection control response to the largest HPIV-3 outbreak in the NICU.
Methods
The NICU has a 96-bed capacity, divided into the NICU, high dependency unit 1 (HDU 1), and high dependency unit 2 (HDU 2). The HDU 1 manages patients requiring respiratory support or post-surgical care, while HDU 2 provides level 2 care for patients with chronic diseases or those nearing discharge. One airborne isolation room (AIIR) is in HDU 2, and each room accommodates 3-4 incubators or cribs. The nurse-to-patient ratio was 1:1-1:2 in the NICU, 1:2-1:3 in HDU 1, and 1:4 in HDU 2.
We retrospectively collected data from electronic medical records (EMR), laboratory reports, and NICU team inputs. Confirmed cases were diagnosed using HPIV-3-positive RT-PCR, while suspected cases included those exposed to an HPIV-3-positive patient or presenting respiratory symptoms despite a negative RT-PCR result. Clearance required 48 hours of clinical stability on room air without antipyretic/antiviral medications and at least 10 days from the respiratory test. Extended isolation was applied for immunocompromised cases and those needing oxygen support. Suspected cases were de-isolated 10 days after exposure if asymptomatic.
Prince Sultan Military Medical City’s virology lab offers 2 respiratory tests: the Xpert Xpress Cov-2/Flu/RSV plus kit (Cepheid GeneXpert) for detecting SARS-CoV-2, Influenza A/B, and RSV, and the respiratory panel 2.1 plus (BIOFIRE FilmArray Torch) for detecting 15 viruses and 4 bacteria. Due to cost constraints, the respiratory panel 2.1 plus was only used if the Xpert Xpress test was negative.
Nasopharyngeal swabs from symptomatic patients were tested using the respiratory panel 2.1 plus via multiplex RT-PCR. However, during the outbreak, kit shortages led to most symptomatic NICU staff being screened with the Xpert Xpress test. Regardless of the results, symptomatic staff were restricted from work until symptoms resolved, per the employee health clinic’s policy.
Statistical analysis
Patient demographics, clinical data, and outcomes were analyzed using Excel 2016. The attack rate (%) was calculated by dividing the number of HPIV-3-positive cases by total exposed patients during the outbreak period and multiplying by 100. An epidemic curve was constructed to illustrate case frequency and outbreak duration. Clinical presentations were classified based on EMR and validated by NICU physicians to differentiate between upper and lower respiratory tract infections.
Results
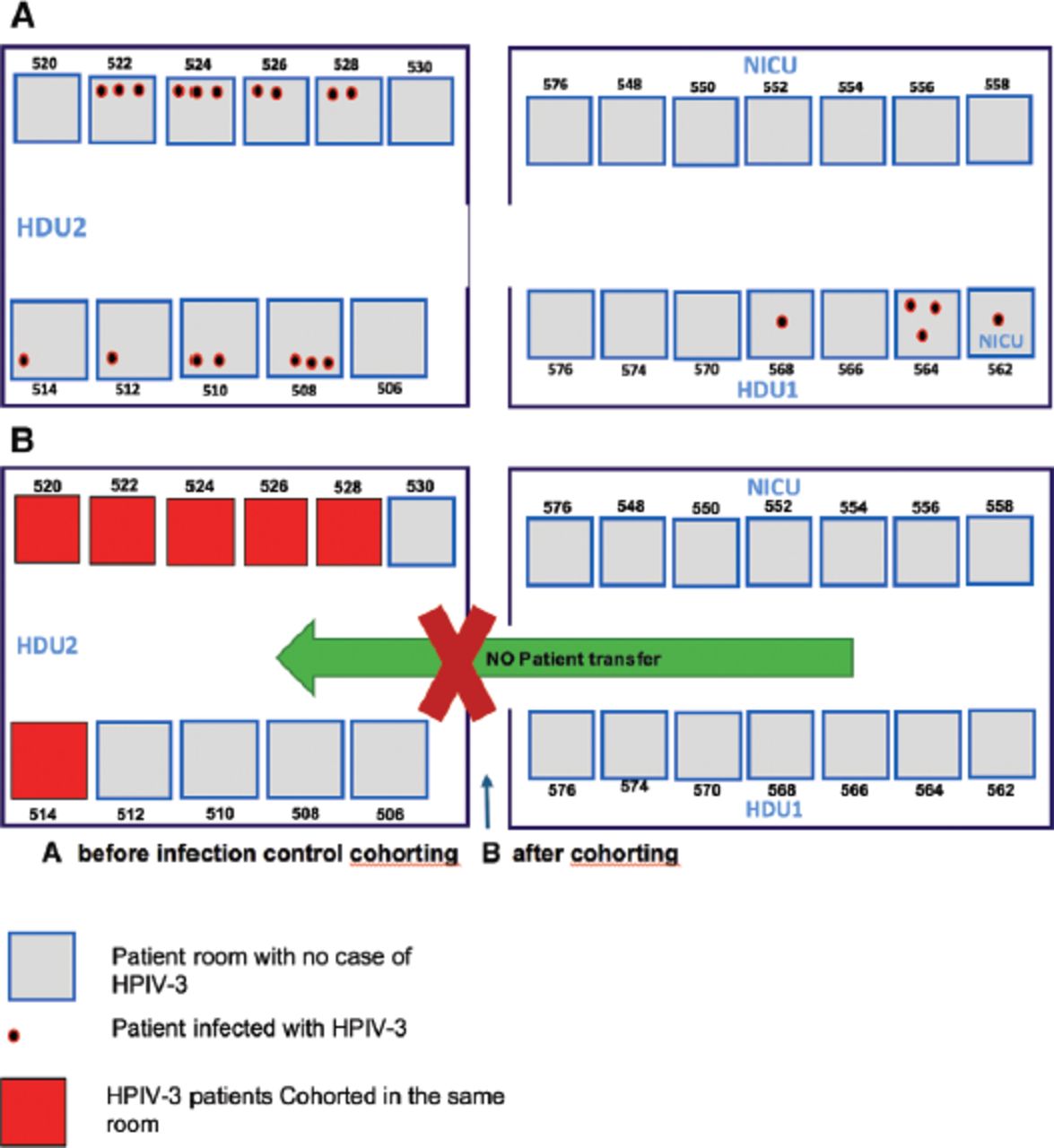
Between December 2022 and January 2023, the NICU was at full capacity (96 patients), including 26 awaiting transfers to long-term pediatric care. A total of 22 patients acquired HPIV-3, with 17 (77.3%) cases occurring in HDU 2 (Figures 1 & 2). The overall attack rate was 23%.

- Neonatal intensive care unit setting and geographic distribution of human immunodeficiency virus type 3 cases. HDU: high dependency unit, NICU: neonatal intensive care unit, HPIV-3: human parainfluenza virus type 3

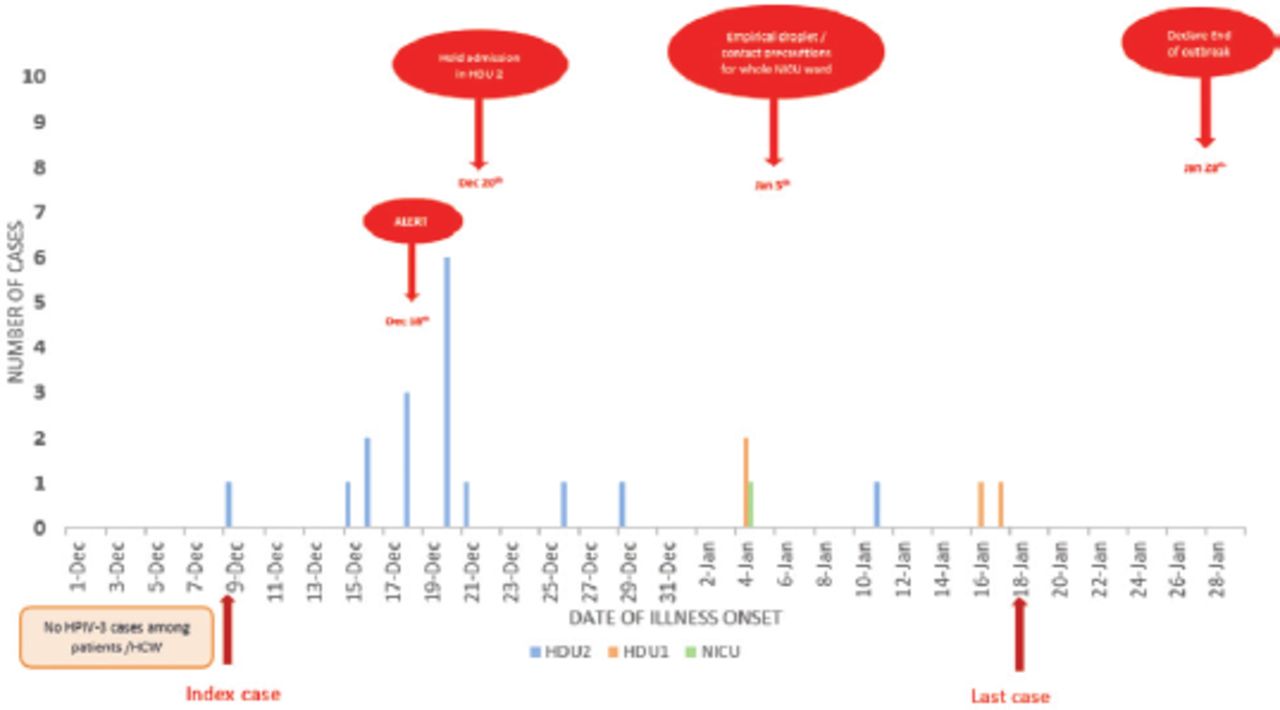
- Epidemic curve of human parainfluenza virus type 3 outbreak in neonatal intensive care unit. HDU: high dependency unit, NICU: neonatal intensive care unit, HPIV-3: human parainfluenza virus type 3, HCW: healthcare worker
The index case was a 9-month-old with chronic lung disease who underwent diaphragmatic hernia repair. Presenting with fever, cough, and copious secretions, the patient was immediately isolated in the AIIR due to oxygen support needs. Recovery occurred after 11 days, and the patient was discharged in December 2022.
Table 1 summarizes the clinical characteristics of infected patients. Ages ranged from 3 weeks to 3 years (mean: 13 months). One full-term neonate (3 weeks old) was affected, while half of the cases were >1 year, occupied cribs, and could not be placed in incubators. Many had underlying conditions: 9 had neurological disorders, 2 had cardiac diseases, and 4 preterm infants had chronic lung disease (mean age at symptom onset: 3 months).
- Demographic and clinical characteristics of patients with human parainfluenza virus type 3.
No coinfections with other respiratory viruses were observed. Fever and cough were predominant symptoms, with illness lasting >17 days in 11 (50%) cases. Lower respiratory tract infections occurred in 18 (81.8%) cases, with 16 requiring oxygen therapy. Four received continuous positive airway pressure (CPAP), 2 required high-flow nasal cannula, and 2 were ventilated. Supportive care, including bronchodilators, was provided, but no antiviral medications were prescribed. All cases improved except for one patient who had holoprosencephaly and died.
Among symptomatic healthcare workers (20 nurses, one physician), 3 were tested with the respiratory panel 2.1 plus, and one tested positive for HPIV-3.
Following the first case, infection control measures included isolation, strict hand hygiene, testing symptomatic patients using RT-PCR, and requiring surgical masks for healthcare workers and visitors.
A week later, 6 additional cases emerged, prompting the outbreak management team to escalate measures: I) dedicating HDU 2 to confirmed and suspected cases, halting new admissions; II) cohorting stable positive cases under contact/droplet precautions, with airborne isolation for oxygen-dependent patients; III) keeping asymptomatic exposed patients in place under empirical precautions, restricting transfers; IV) install 2-3 portable high efficiency particle arresting filters per affected room and close patient room doors; V) assigning dedicated staff and equipment, prohibiting personnel movement between HDU 2 and other areas; VI) implementing respiratory logbooks for all personnel/visitors, daily symptom monitoring, and work restrictions for symptomatic staff; VII) restricting visitors except when medically necessary (namely, breastfeeding); VIII) medical team visits are limited to 2 per specialty; and IX) enhancing environmental cleaning with hospital-approved disinfectants.
Despite these measures, new cases emerged in the NICU and HDU 1, affecting preterm and critical patients. Consequently, empirical droplet/contact precautions were extended hospital-wide. Elective NICU admissions from obstetric wards and regional hospitals were halted, and infection control audits intensified. Respiratory triage was mandated at NICU entrances, and surgical mask use became obligatory throughout the ward, including corridors and staff areas.
The outbreak lasted 51 days, officially ending in January 2023, 10 days after the last reported case.
Discussion
Despite the prevalence of common pathogens responsible for LRTI in pediatric patients, HPIV-3 outbreaks in NICUs are rare, partly due to the high reported frequency of passive immunity to HPIV during the neonatal period.8 The attack rate in our study was 23%, which is relatively high, as the mean age of affected patients was 13 months. Except for one case aged 3 weeks, all infected babies were older than 28 days. These findings align with those of Moisiuk et al,9 who reported a nosocomial HPIV-3 outbreak in a nursery where the mean age of infected infants was 42 days, compared with 11 days for non-infected infants. This suggests maternal neutralizing antibodies may no longer protect older convalescing infants.5
We identified the index case as the first detected patient, as no suspected cases were recorded among patients or healthcare workers in the previous 2 weeks. However, transmission from asymptomatic individuals (healthcare workers or visitors) or those with mild symptoms might have occurred.10,11 Many of our patients were in open cribs due to their larger size, increasing exposure risk through coughing and sneezing. The HPIV transmission occurs via direct personal contact and inhalation of infected droplets.4 The virus can survive for several hours on environmental surfaces and may be transferred by hospital personnel, contributing to its spread.12 The nurse-to-patient ratio was 1:4 (reaching 1:5 in rooms with full NICU capacity) potentially impacting infection control compliance.
The HPIV outbreaks in NICUs commonly affect infants with severe comorbidities requiring invasive ventilation and can result in high mortality rates, particularly among highly premature neonates and immunocompromised children.2,5 Currently, no effective antiviral treatment exists, and management remains supportive. In our study, all HPIV-3-infected patients showed clinical improvement except one baby with alobar holoprosencephaly, who was on compassionate care and passed away.
The morbidity associated with HPIV-3 in our study appeared lower than that reported in a tertiary neonatal unit in Singapore.9 Only 2 infants required invasive ventilation (one of whom was already ventilated). Three patients required CPAP, and 2 needed high-flow nasal cannula support. Differences in demographics and clinical features between patient populations may explain this variance.
The HPIV-3 nosocomial infections generally prolong hospitalization. In our study, symptom duration ranged from 8-39 days, with an average of 17.5 days, consistent with Teo et al’s report (19.3 days).3 Infants’ underlying chronic conditions likely influence the duration of their illness. The HPIV-3 infection in preterm infants often presents with nonspecific symptoms and should be considered an important differential diagnosis.
Enhanced infection prevention measures were promptly implemented and adjusted as the outbreak evolved. Positive and suspected cases were isolated in a single NICU wing (HDU 2), and the entire unit was placed under empirical contact and droplet precautions, with mandatory universal masking for all individuals. Universal surgical mask use by those in direct patient contact, regardless of symptoms or season, has been associated with significant reductions in respiratory viral infections, particularly HPIV-3.13 Visitor restrictions and limiting medical teams to 2 per specialty likely reduced viral spread. Visitor restrictions have been employed in hospitals since the early 1800s to control infection transmission and minimize stress for patients and families.14,15 The healthcare-associated viral respiratory infection (VRI) transmission index (number of HA VRIs per 100 inpatient community-associated VRIs) was found to be 59% lower during months with visitor restrictions.15
All referrals from other hospitals were suspended; however, the labor ward remained operational due to our hospital’s 11,000-patient delivery volume. Transferring patients to alternative hospitals proved challenging, impacting NICU bed capacity and infection control compliance.
Study limitations
First, molecular sequencing was not carried out, preventing us from determining whether patients were infected with the same HPIV-3 strain. Second, due to limited stock during the outbreak, most exposed and symptomatic healthcare workers were not tested using the respiratory panel 2.1 plus kit. Consequently, testing was prioritized for symptomatic patients, and clearance relied on clinical improvement rather than repeat testing. The exact duration of viral shedding remains unknown. Additionally, discharge delays for approximately 33% of non-infected babies from HDU 2, due to a lack of long-stay pediatric care and home care options, affected bed capacity and may have contributed to the virus.
Despite these limitations, our study provides valuable insights into HPIV-3 outbreak management in NICUs. Our findings underscore the importance of early detection, strict infection control measures, and adaptive strategies to minimize transmission. Future studies with molecular sequencing and broader screening of healthcare workers could provide a further understanding of transmission dynamics and improve outbreak management protocols.
In conclusion, HPIV-3 infection is underdiagnosed in the NICU. Although its incidence is relatively low, and outbreaks are rare, HPIV-3 infection may cause significant mortality and morbidity in premature and immunocompromised neonates. Early detection is necessary to limit the spread of the infection and avoid unnecessary investigations and an extra length of hospital stay. This study spotlighted the value of infection control measures, medical personnel’s awareness of these preventive measures, and increased awareness among nurses. It also emphasized the need for teamwork to identify and implement appropriate actions. Moreover, this event highlighted the need to discharge chronic patients into long-term care facilities and home respiratory care as soon as possible.
Acknowledgment
The authors gratefully acknowledge Editage for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 5, 2024.
- Accepted March 26, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.