


Abstract
Objectives: To examine the influence of socioeconomic factors, anxiety, depression, and personality traits on the decision to undergo breast reconstruction (BR) post mastectomy.
Methods: In this cross-sectional study, adult female breast cancer (BC) patients who had undergone a mastectomy between January 2017 and 2019 were interviewed using a 46-item questionnaire at King Abdulaziz University Hospital, Jeddah, Saudi Arabia. The questionnaire was divided into 5 sections: demographic data, personality traits, the Narcissism Index (NI), and the Hospital Anxiety and Depression Scale (HADS).
Results: The sample (N=196; mean age: 48.44 [± 9.87] years, opted for BR: 60.2%, with chronic diseases: 36.7%, Saudi nationals: 43.9%) obtained means of 4.17 (± 2.81) on NI score, 7.72 (± 4.88) on anxiety score, and 5.78 (± 4.65) on depression score. Group differences in age, depression, lymph node involvement, and 2 personality traits emerged.
Conclusion: Age and depression significantly influenced the decision to undergo BR. Women who had opted for BR tended to be younger, be less depressed, and be characterized by lesser nodal involvement. Personality traits also influenced the decision to undergo BR. Diagnosing and treating depressed patients is an important component. A patient’s age should not deter physicians from counselling them about BR.
Breast cancer is the most commonly occurring cancer among females, and it affects 2.1 million women worldwide each year.1 Among Saudi women, it is the most common cancer.2 The incidence of breast cancer in the United States (US) is 124 per 100000 women.3 In many cases of breast cancer, a mastectomy is indicated. Mastectomy significantly deprives women of their sense of femininity and makes them feel less attractive, and this in turn adversely influences their quality of life (QOL).4-7 Postmastectomy breast reconstruction (BR) improves QOL.8,9 There are primarily 2 types of BR, namely, implant and autologous (flap) reconstruction, and each of these can be implemented through various approaches. For example, implants include saline and silicone. A flap of the latissimus dorsi or transverse rectus abdominis (TRAM) is used for autologous BR. The latissimus dorsi flap is swung from the back. It provides less fullness than TRAM, thus an implant or a fat graft is often used coupled with it.10 A TRAM flap is performed by rotating the rectus abdominis muscle or by removing a smaller part of the muscle with its skin (free flap). Free TRAM flaps provide more flexibility and lower risk of tissue necrosis when compared to pedicle TRAM flaps.11 It has been shown that autologous BR yields superior outcomes, when compared to implant BR.12-14 Nowadays, most BRs involve implants; in the late twentieth century, autologous implants were more popular.15 This change is partially attributable to surgeons’ efforts to provide the option of reconstruction to the high-risk postmastectomy population (namely, patients with other comorbidities and/or those older than 60 years).16
Breast cancer patients experience psychological morbidities, primarily mood disorders, after receiving and when living with the diagnosis. The untreated anxiety and depression are important factors that render the QOL of these patients low, not merely the physical aspect of the patients’ presentation.17,18 These morbidities in women with breast cancer are often overlooked and left untreated because they can have unclear presentations.17
According to the findings of a Polish study, deciding to undergo BR after breast removal is correlated with personality traits among women. Specifically, introverts rarely opted to undergo BR.19 Another important personality type is the narcissistic personality. Specifically, narcissists tend to demand perfectionism as it is a sentinel feature of their personality type; hence, they seek to have an extremely attractive body.20-22
Despite recommendations to undergo BR, the rates at which the procedure is performed are low, ranging from 11% to less than 40% (in some tertiary care centers in the US).23,24 The decision to undergo BR is complicated by a variety of procedures.12 Women are asked to choose from an array of procedures, and the problem has become more strenuous with the development of the perforator flap technique, which minimizes the risk of hernia albeit requires longer operation time.12 Additionally, the burden that the surgical procedure places on the patient and her relatives makes the decision-making process even more difficult.25 Two studies that were conducted in Europe found that the patient’s age influences her decision to undergo BR and the possession of information about the procedure.26,27
Only a small proportion of treated breast cancer patients decide to undergo BR.15,28 Therefore, it is important to examine which mood states and social aspects influence this decision-making process. In this study, we aimed to examine the influence of socioeconomic factors, anxiety, depression, and personality traits on the decision to undergo BR after a mastectomy in one center in Jeddah, Saudi Arabia.
Methods
This cross-sectional study was conducted between March and July 2019, using an interview-based questionnaire. This interview was conducted among female patients who were diagnosed with breast cancer at King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia.
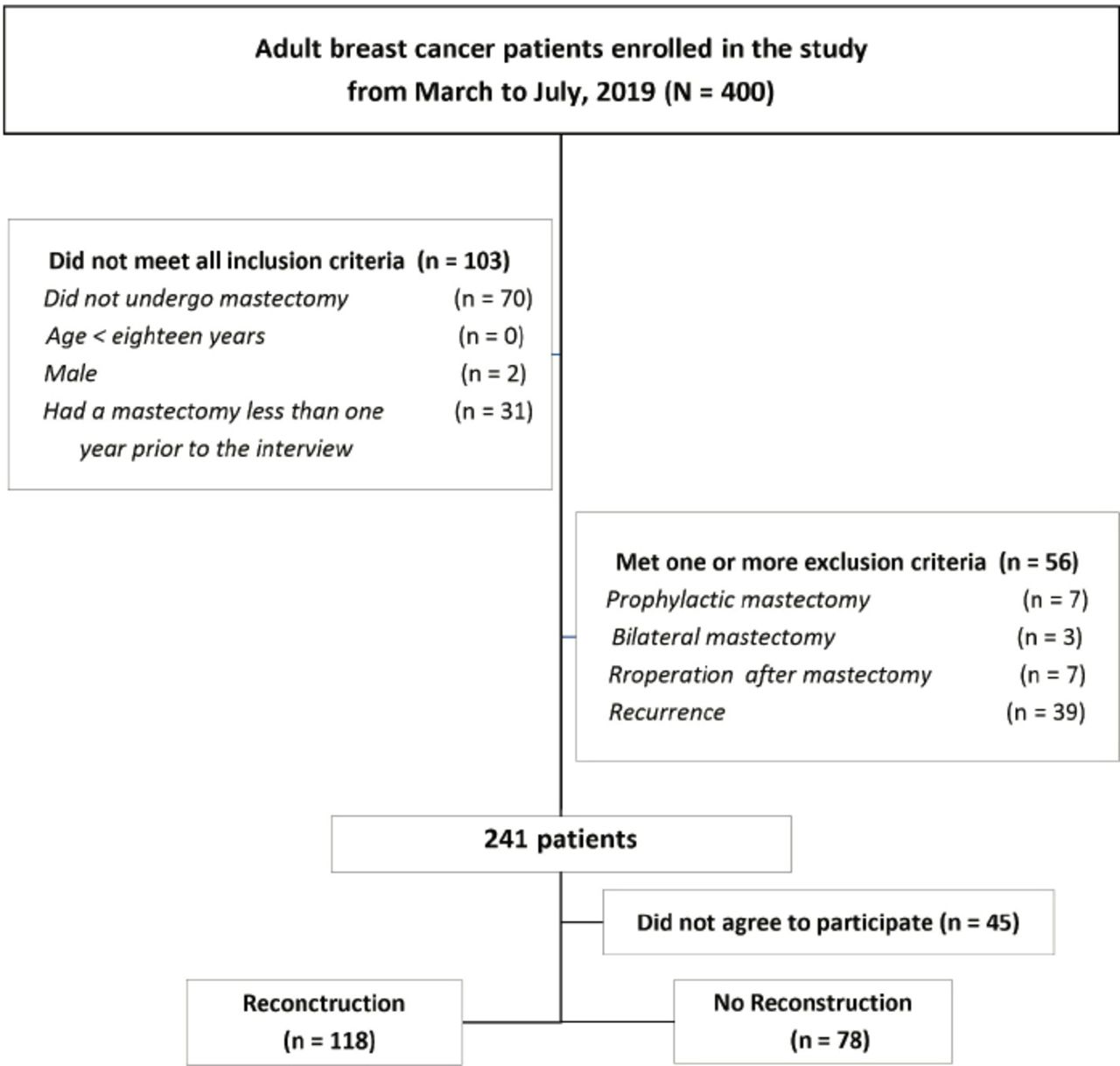
Women aged 18 years and older who had undergone mastectomy for breast cancer between January 2017 and 2019 were included. The exclusion criteria were as follows: a) undergone bilateral mastectomy, contralateral mastectomy for prophylactic purposes, or a reoperation and b) breast cancer recurrence. All contributors were knowledgeable before participation, and those who agreed to contribute were registered. Approximately 400 randomly chosen patients were identified from the hospital records, and 241 of them who met the study’s inclusion criteria were contacted; only 196 patients agreed to participate (Figure 1). Patients were divided into 2 subgroups: Group A, which consisted of women who had opted for BR and Group B, which consisted of women who chose to not undergo BR.
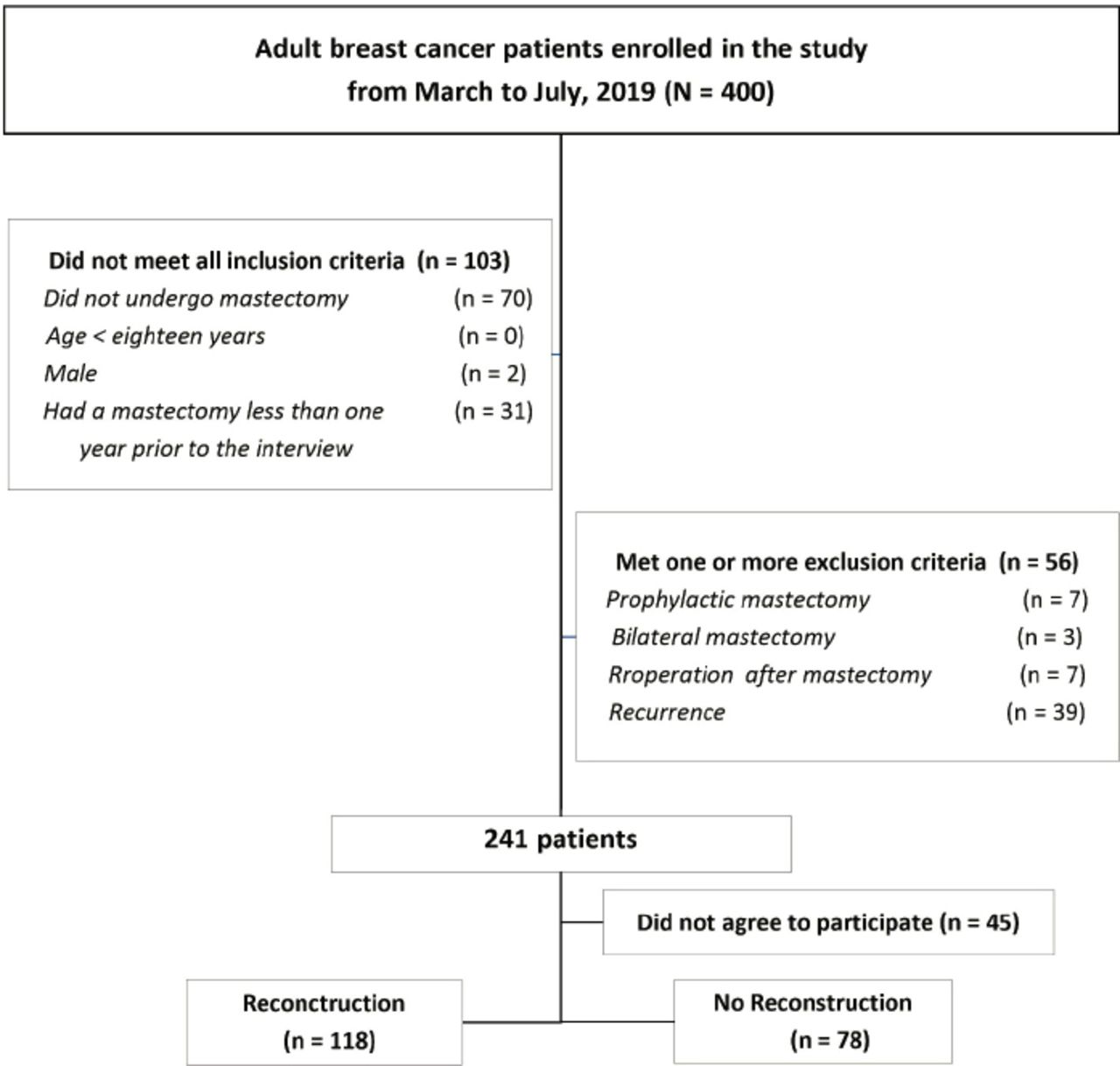
Flowchart depicting the inclusion and exclusion of the study participants.
Study variables
We reviewed the literature and developed a valid questionnaire based on the findings of several published studies.19,29-32 The questionnaire consisted of 46 questions that were divided into 5 sections: demographic data, personality traits,19 the Narcissism Index (NI),29,30 and the Hospital Anxiety and Depression Scale (HADS).31,32 The NI is a reliable tool for predicting the degree of narcissism.29,30 The reliability and validity of HADS on similar populations (breast cancer patients) has been studied, and it has been shown to have a good predictive value. Furthermore, the Arabic translation used in this study has been shown to be both valid and reliable.31-33 The study was conducted after ethical approval was granted by the Research Ethics Committee at the King Abdulaziz University Hospital. Patients participated in this study on an entirely voluntary basis.
Statistical analysis
Data were checked for completeness, and errors were corrected. The normality of the distributions of continuous variables were checked by conducting the Shapiro-Wilk and Kolmogorov Smirnov tests. Their results indicated that all variables were none normally distributed. The sociodemographic variables and clinicopathological features (namely, tumor size, lymph node involvement, and metastasis-TNM) of the 2 participant groups were compared using the Chi-squared test. Respondents’ scores on the NI and HADS were calculated by counting the responses. The mean scores of the 2 participant groups were compared using the Mann-Whitney U test. The relationship between TNM and anxiety and depression scores were examined using the Kruskal-Wallis test. The extroversion/introversion personality continuum of the 2 participant groups were compared using Chi-squared and fisher exact tests. Binary logistic regression analysis was conducted to identify the predictors of the decision to undergo BR. The results have been presented using tables and figures.
All analyses were conducted using the Statistical Package for Social Sciences version 23.0 (IBM, Armonk, NY, USA), and 95% confidence intervals were computed to interpret the results.
Results
A total of 196 patients were interviewed, and 118 (60.2%) of them had opted for BR; the remaining 78 (39.8%) patients had not opted for BR. The mean age of the participants was 48.44 (± 9.87) years. Further, 86 (43.9%) patients were Saudi, the monthly income of 118 (60.2%) patients was <5000 Saudi Riyals (SR). One hundred and thirty (66.3%) patients were unemployed/housewives, 72 (36.7%) patients had chronic illnesses, and 76 (38.8%) patients had a family history of breast cancer (BC). Out of the 76 participants with a family history of BC, 71.1% had a relative who had BC and had undergone BR. The sociodemographic characteristics for each participant group are presented in Table 1.
-Sociodemographic characteristics and clinicopathological features of the respondents split by participant group.
The group of women who had opted for BR tended to have younger women (mean difference between the 2 groups was 7.53 years, p<0.001), fewer nonsmokers (p=0.015), and more women without chronic illnesses (p<0.001). Unemployed participants were less likely to have opted for BR (p=0.041). With regard to the TNM classification, a lymph node involvement was less prominent among those who had opted for BR (p=0.13) (Table 1).
Personality traits and mood status
The mean depression score for all participants was 5.78 (± 4.65), anxiety score 7.72 (± 4.88), and NI 4.17 (± 2.81). Table 2 shows that anxiety (9.67 ± 5.07 versus 6.44 ± 4.31, p<0.001) and depression scores (7.74 ± 4.90 versus 4.49 ± 3.97, p<0.001) were significantly higher among participant who had opted to not undergo BR. However, scores on the NI were higher among those who had opted for BR (p=0.030) (Table 2).
Distribution of respondents’ mean NI score, anxiety score and depression score split by participant group.
The responses that the 2 participant groups provided to the extroversion/introversion personality questions (total: 5 questions) are summarized in Table 3. Group comparisons revealed that there was a statistically significant difference in the responses that were provided to questions 4 (p=0.0002) and 5 (p<0.001) (Table 3).
Extroversion/introversion personality continuum in the 2 study groups.
Disease stage and mood status
There was no statistically significant relationship between TNM classification and anxiety and depression scores (p>0.050).
Binary logistic regression
Binary logistic regression analysis was used to identify the predictors of the decision to undergo BR. Anxiety and depression scores, sociodemographic variables, TNM classification, and adjuvant treatment were included in the regression analysis. The results revealed that depression scores, age, and lymph node involvement were statistically significant predictors of BR decision. Other included variables were not statistically significant (p>0.050) (Table 4).
Logistic regression of the predictors of the decision to undergo breast reconstruction postmastectomy.
Discussion
Among breast cancer patients, undergoing mastectomy frequently has a negative impact on the QOL and psychological well-being. Undoubtedly, this body part entails important psychological implications. Consequently, patients who have undergone a mastectomy perceive a decline their sense of femininity and confidence levels. A mastectomy without BR can alter the mood and behaviors of patients in their workspaces.34 Further, it can strongly impact their roles as a family member. Therefore, BR after breast removal can tremendously improve QOL and perceived body image. Accordingly, we aimed to examine the relationship that the decision to undergo BR shares with different personality traits, depression, anxiety and sociodemographic variables among breast cancer patients.
The existing literature suggests that age is a very important determinant on BR.24,26,27 A similar result emerged in this study. This finding is attributable to surgeons’ fear of postoperative complications, especially in a patient with other chronic illnesses.27 There was a significant difference in BR status between Saudis and non-Saudis. This finding may be attributable to group differences in access to healthcare or the relatively higher mean depression (6.47 ± 4.96 versus 4.91 ± 4.04, p=0.035) and anxiety scores (8.93 ± 5.18 versus 6.19 ± 4.00, p<0.001) that non-Saudi participants obtained (the regression analysis presented in Table 4 yielded no significant predictor).
Another interesting finding was that the patients who were willing to undergo BR were healthier and did not have any chronic illnesses or comorbidities, when compared to the other group. Being healthy is closely related to happiness, and deciding to undergo such a procedure can tremendously improves a patient’s QOL.4-7,35 This is similar to the findings of 2 studies that were conducted in the US36 and Australia,37 whereby patients with fewer comorbidities were found to be more likely to undergo BR.
Past findings suggest that patients with early-stage BC are more likely to undergo BR. Similarly, in the present study, the percentage of node negative patients was higher in the BR group. It is noteworthy that many of these early stage BC patients do not require postmastectomy chemotherapy and radiotherapy.24
It is noteworthy that, in the present study, patients with a family member who had undergone BR were more likely to have opted for BR than their counterparts. This may be the case because BC survivors prefer to receive information about BR from their friends and peers. Further, they feel less isolated after they receive such information from patients who have undergone BR.38
In this study, the HADS was used to assess the affective states of the participants. The Center for Epidemiological Studies Depression (CES-D) Scale was not used owing to 2 primary reasons: a) it does not screen for anxiety and b) its performance and reliability has been examined primarily mostly on young population.39,40 In comparison, the HADS is a simpler assessment, and its reliability has been examined across different contexts (including among BC patients and cancer patients in general) and age groups.31-33 Our results suggest that women with depression and anxiety are not prepared to undergo another nonvital procedure as most of the focus is on monitoring BC recurrence with anxiety and depression being vaguely present.17 Satisfactory doctor-patient communication regarding patient concerns and the provision of crucial information to the patient are important factors that can improve the detection of psychological problems and mitigate depressive symptoms and anxiety among BC patients.18
The responses that the 2 groups provided to the 5 personality questions, which were adapted from the assessment that was used in a Polish study, were compared using Chi-squared and fisher exact tests (Table 3). Interestingly, 2 questions for which significant group differences had emerged in the original study had also evidenced significant group differences in the current study.19 In both the studies, patients who had opted for BR were more likely to be extroverted, as extrovert individuals are mainly outgoing and like to be with others. In the present study, the NI scores were higher among those who had opted for BR.
Study limitations
Although our sample size was moderate, and the study’s objectives were addressed, the study has a few limitations. First, our article was cross-sectional in nature and covered a short time period. Therefore, the participants may not have been representative of the entire population of Saudi Arabia. Second, this study was conducted in a single center, thereby limiting the generalizability of the results. Third, the reliability of the 5 personality questions has not been studied. In the future, studies must include a larger number of hospitals that represent different regions within the country. This study offers insights into the prevalence of depression and anxiety among breast cancer patients after mastectomy. It also uncovers the variability in personality traits within this population. More importantly, it indicates that depression single handedly plays a significant role in the decision to not undergo BR, after potential confounds are controlled for. It is important to screen and detect undiagnosed depression and anxiety among patients who have undergone a mastectomy. This is necessary to effectively treat these conditions through prompt referral to a psychiatrist, improve their QOL, restore at least a moderate level of functioning, and provide assistance during this difficult postmastectomy decision-making period. Patients of all ages should receive counseling about BR after a mastectomy.
In conclusion, undergoing BR is a difficult, yet important decision for a woman who survived BC to make. Age and depression significantly influenced this decision among our study participants. Women who opted to undergo BR tend to be younger, report lower levels of depression, and were characterized by less nodal involvement. Certain personality traits can also influence the decision to undergo BR. Diagnosing and treating depressed patients is an important aspect of caring for BC patients. A patient’s age should not deter physicians from counseling patients about BR.
Acknowledgment
The authors would like to thank Randa Abushanab and Renad Alnemari for their help in data collection. Also, we would like to acknowledge www.Editage.com for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 1, 2019.
- Accepted January 16, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.