


Abstract
Objectives: To correlate the clinical severity of laryngomalacia (LM) with endoscopic findings, swallowing evaluations and polysomnography in a cohort of patients .
Methods: We conducted a retrospective analysis between 2017-2018 on a cohort of patients diagnosed with upper airway obstruction (UAO), stridor, noisy breathing or laryngomalacia. This study took place at the Pediatric Pulmonology Department, Riley Children’s Hospital, Indianapolis, United States of America.
Results: There were 157 patients with laryngomalacia included in the study. Patients with severe LM were significantly younger than those with mild LM (p=0.0214) and moderate LM (p=0.0220). Subjects with type I of LM were significantly older than type III (p=0.0051).When associations were tested between polysomnogram (PSG) variables and clinical severity, there were significant associations with age at PSG. The overall apnea-hypopnea index (AHI) in mild (p=0.0103) and moderate (p=0.0242) were significantly lower than the severe group. The rapid eye movement (REM) AHI was significantly lower in moderate cases than severe (p=0.0134). The end-tidal carbon dioxide (EtCO2) peak was significantly lower in mild cases than severe (p=0.0141).The total sleep time (TST) peripheral capillary oxygen saturation (SpO2) 90% occurs in both mild (p=0.0197) and moderate (p=0.0498)) were significantly lower than the severe group.
Conclusions: The severity of the clinical manifestations of LM did not correlate with the different endoscopic types in our study. The presence of cyanosis was associated with type III LM. Rapid eye movement AHI and EtCO2 in polysomnogram were remained significantly associated with clinical severity.
Laryngomalacia (LM) is defined as collapse of upper larynx during inhalation.1 It is the most common cause of stridor in newborns2-4 affecting 45-75% of all infants with congenital stridor.5 The range of disease presentation, progression, and outcomes varies.5 Symptoms usually appear within the first 10 days of life. Signs of disease severity are apnea, cyanosis , failure to thrive, episodes of respiratory distress, obstructive sleep apnea, and feeding difficulties.1,6 In most cases, LM presents as a mild disease, and the symptoms resolve spontaneously by 12-18 months of age.3,7 Up to 20% of patients have severe LM and may require surgical intervention.8 Rigid or direct micro laryngoscopy (MLB) is the standard study for airway abnormalities.9 Flexible fiber optic laryngoscopy (FFLT) is a safe and effective diagnostic tool for pediatric cases.10 Detection and characterization of dynamic airway lesions is better attain by FFLT than MLB.11 In a small cohort, studying the findings of FFLT correlated epiglottic prolapse with clinical severity of LM and cuneiform prolapse with feeding difficulties.12 Previous studies showed a concurrence between gastroesophageal reflux (GER) and LM, but the evidence for a causal association is sparse.13,14 In patients with LM, GER was significantly associated with severe symptoms and complicated clinical course.13 Laryngomalacia may link significantly to obstructive sleep apnea syndrome (OSAS) in some children.15 Polysomnography may be useful in infants with LM to diagnose obstructive sleep apnea and/ or to objectively evaluate clinical outcomes as studies suggest.16,17 Supraglottoplasty may be an effective and safe surgical alternative to improve moderate to severe OSA in infants with LM.8,18 A recent study19 found a faster improvement in the quality of life of caregivers of infants with LM who were surgically managed.
Our goal was to correlate the clinical severity of LM with endoscopic findings, swallowing evaluations, and polysomnography using the International Pediatric ORL Group (IPOG) LM consensus recommendations20 and the Groningen LM classification system.21 That will help to find any significant trends of presentation of LM and endoscopic findings in larger cohort of patient
Methods
Study was conducted at the Pediatric Pulmonology Department, Riley Children’s Hospital, Indianapolis, United States of America (USA). After Institutional Review Board approval, we conducted a retrospective cohort study of pediatric patients under 2 years of age with diagnoses of upper airway obstruction (UAO), stridor, noisy breathing, or LM between January and December 2012.
The inclusion criteria were as follows: patients born at ≥ 37 weeks of gestation who underwent a comprehensive evaluation in outpatient or inpatient settings with airway endoscopy and polysomnography. We excluded patients born <37 weeks of gestation or those older than 2 years of age. We also excluded patients with known genetic disorders/chromosomal abnormalities, cardiac disease, neurologic disease, chronic respiratory disease, and craniofacial dysmorphisms. Formal evaluation of each patient was performed using the International Pediatric ORL Group (IPOG) LM consensus recommendations20 to help classifying the clinical severity of LM and the Groningen LM classification system21 to classify different types of LM. The clinical severity of LM was divided into 3 categories based on the clinical presentation and IPOG LM consensus recommendations: mild LM (inspiratory stridor with no other symptoms or radiological findings suggesting secondary airway lesions); moderate LM (cough, choking, regurgitation, and feeding difficulties); and severe LM (apnea, cyanosis, failure to thrive, pulmonary hypertension, and cor pulmonale). Groningen classification used the characteristics of laryngeal dynamic abnormalities as shown during flexible laryngoscopic evaluation. Type I had inward, antero-caudal collapse of the arytenoid cartilage into the glottis. Type II had medial displacement of the aryepiglottic folds during inspiration with or without epiglottic curling, and Type III had postero-caudal suction of the epiglottis to the posterior pharyngeal wall.
Patients were identified by screening for the international classification of disease (ICD) codes for UAO, stridor, noisy breathing, and LM (ICD-9 codes 519.8, 786.1, 748.3, 478). One author (RAA) reviewed the electronic medical records for each patient as well as endoscopic video collected by a board-certified pediatric pulmonologist. We collected demographic data, polysomnogram results, feeding evaluations/VFSS, endoscopic evaluation, and the age at each study. The following data were collected from the polysomnogram (PSG): apnea-hypopnea index (AHI), rapid eye movement (REM) AHI, arousal index, end-tidal carbon dioxide (EtCO2), percentage of total sleep time with O2 saturations <90%, and need for supplemental oxygen. Video fluoroscopic swallow studies (VFS) were conducted by a radiologist and speech therapist working together. The VFS data could evaluate the presence of penetration/aspiration of different food consistencies appropriate to the patient’s age. The PSG studies were manually scored by a registered polysomnogram technician; the raw data were subsequently reviewed and interpreted by a board-certified sleep physician following the American Academy of Sleep Medicine Guidelines.
Obstructive sleep apnea (OSA) was classified as mild, moderate, and severe based on the AHI and was defined as the total number of obstructive apnea and hypopnea events per hour of sleep. The PSG outcome variables of interest for determining the severity of OSA were the AHI/REM AHI (AHI/REM AHI events per hour were reported as 1-5=mild, 5.1-10=moderated, or >10=severe obstructive sleep apnea), arousal index (normal <12/hour), EtCO2 peak (normal ≤45 mm Hg), and total sleep time with oxygen saturations <90% (normal <5 minutes).22
At the Riley Hospital for Children, we evaluate more than 1000 pediatric patients/year for stridor and noisy breathing with concern for upper airway obstruction. Laryngomalacia has historically been found to be the most common diagnosis in these children. At our institution, pediatric pulmonologists primarily evaluate children with stridor or concern of upper airway obstruction via flexible bronchoscopy. Flexible laryngoscopy or rigid bronchoscopic evaluation is occasionally performed by otolaryngologists.
Statistics analysis
Analyses were performed to determine if significant associations existed between the clinical severity of LM and endoscopic type. Laryngomalacia was determined based on symptoms, presence of sleep-related disease seen in PSG, and the presence of feeding difficulties diagnosed by VFSS. Basic demographic analyses were performed using Fisher’s exact tests due to small frequencies and analysis of variance (ANOVA) models. Analyses with the PSG variables also used ANOVA methods for unadjusted models and with analysis of covariance (ANCOVA) models to adjust for age. Post-hoc pairwise comparisons were Bonferroni adjusted to control for inflated type I error. All analytic assumptions were verified in that observations were normally distributed within each group and that groups had a common variance. Log-transformations were performed on those variables that were skewed and thus non-linear so that the assumptions could be met. Analyses were also performed on the sub-sample of participants who had a follow-up PSG to determine if a significant change occurred in the PSG variables for those who did not have an intervention. This analysis was performed using a paired t-test with the null hypothesis that the change was zero. All analyses were performed using SAS v9.4 (SAS Institute, Cary, NC). Significance level of p-value is p<0.05.
Results
Between January and December 2012, we evaluated 617 patients for stridor, noisy breathing, or possible upper airway obstruction at our institution (Riley Children’s Hospital, Indianapolis, USA). Of these, 157 patients met the inclusion criteria. The demographics are described in Table 1.
Demographics characteristics of study participants.
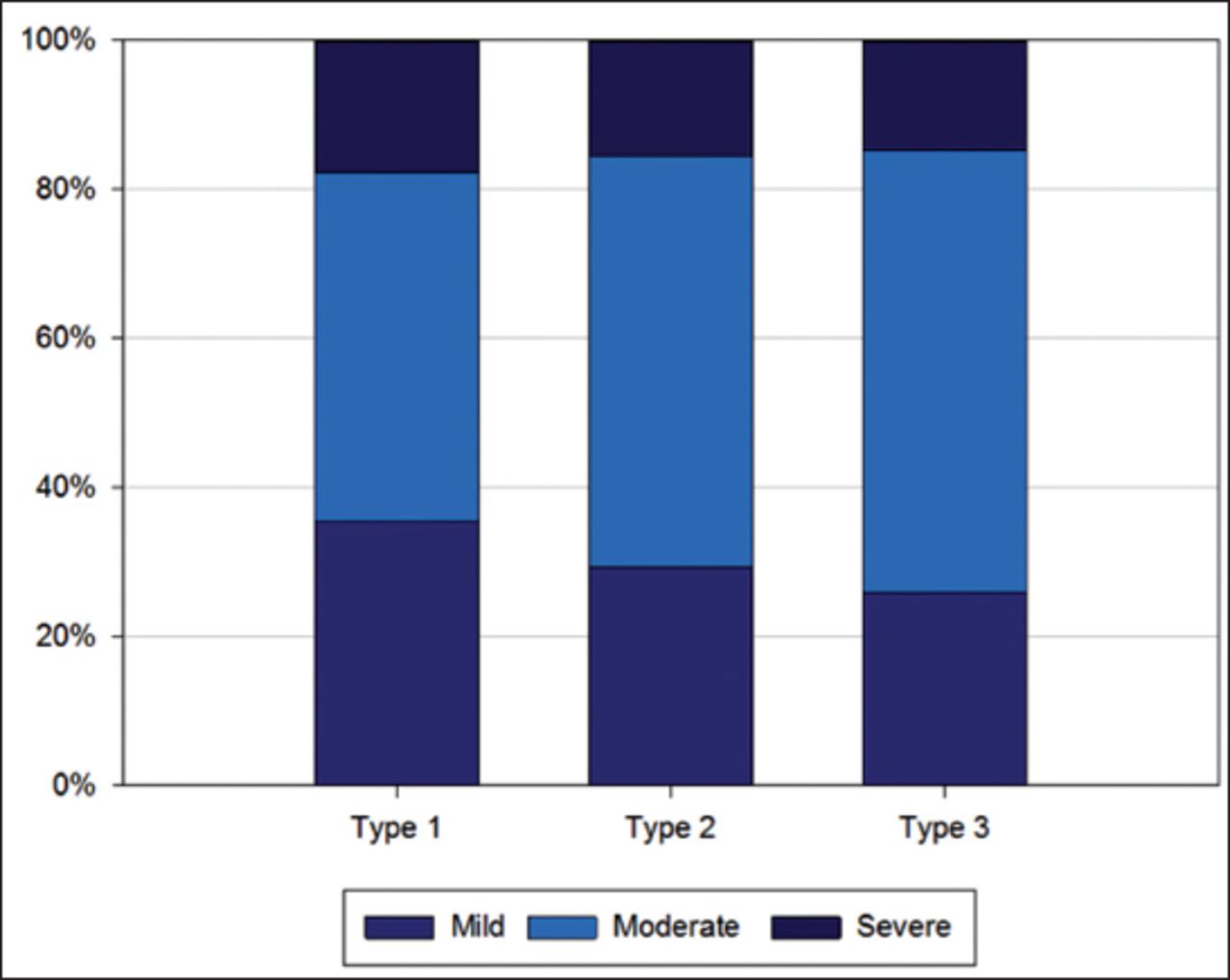
Based on the IPOG LM consensus clinical classification of LM, 50 patients had mild, 82 patients had moderate, and 25 patients had severe LM. All patients underwent endoscopic evaluation by flexible bronchoscopy (n=146; 95.4%) or by rigid bronchoscopy (n=7; 4.6%): 45 patients were classified as type I, 51 patients as type II, and 54 patients as type III LM. The severity of the clinical manifestations of LM did not correlate with the different endoscopic types (Figure 1).

There was no significant association between ordinal categories (Chi-square test p=0.8017, ordinal concordance test: p=0.6217).
The most common symptom of LM was inspiratory stridor with no symptoms or radiographic finding suggesting secondary airway lesions (n=157, 100%) followed by feeding difficulties (n=146, 93%) and cough (n=27, 17.2%). Nine patients (5.7%) presented with cyanosis.
The only significant association between demographics and clinical severity was age. The median age of mild LM group was 2.79 months, moderate LM group was 2.04 months, and severe LM group was 1.55 months (p=0.0409). After Bonferroni correction for pairwise comparisons, patients with severe LM were significantly younger than those with mild LM (p=0.0214) and moderate LM (p=0.0220) (Table 2).
Different demographic groups and the clinical severity of laryngomalacia.
Patients with type I LM by endoscopic evaluation were significantly older than those with type III (p=0.0051) after Bonferroni adjustment. More Caucasian patients had type II LM than type I or type III (p=0.0169; Table 3). A VFS was more likely to be performed in subjects with a higher clinical severity of LM (N=40 studies): mild LM (n=1, 2%); moderate LM (n=28, 34.2%), severe LM (n=11, 44%), p<0.0001. Of these, 33 were abnormal with 14 (42.4%) revealing aspiration and 19 (57.6%) revealing penetration.
Different demographic groups and the endoscopic types of laryngomalacia.
Of the 125 (80.1%) patients who underwent PSG, 31 had mild LM, 70 had moderate LM, and 24 had severe LM. The PSG variables of interest are age at the study, overall AHI, REM AHI, arousal index, EtCO2 peak, and TST <SpO2 <90%. Table 4 describes the associations between PSG variables and clinical severity (IPOG) LM consensus clinical classification of LM. After Bonferroni adjustment of all variables, the overall AHI remained significantly lower for patients with mild (p=0.0103) and moderate (p=0.0242) than patients with severe LM. Similarly, the REM AHI remained significantly lower for patients with moderate LM than those with severe LM (p=0.0134). The EtCO2 peak remained significantly lower for patients with mild LM than those with severe LM (p=0.0141). The TST <SpO2 90% remained significantly lower for patients with mild LM (p=0.0197) and moderate LM (p=0.0498) than those with severe LM after Bonferroni adjustment. However, the association between age at PSG and clinical severity of LM were not significant after Bonferroni adjustment. When adjusting for age, the association between clinical severity of LM with overall AHI was attenuated, but the other variables remained significant.
PSG variables and the clinical severity of laryngomalacia.
Table 5 describes the association between the PSG variables with endoscopic types of LM. The age at PSG was significantly associated with endoscopic type: patients with type I LM were significantly older than patients with type III LM (p=0.0051) after Bonferroni adjustment.
Polysomnogram variables and the endoscopic types of laryngomalacia.
The clinical outcomes showed that 82 (52.2%) patients had no clinical intervention; 65 (41.4%) patients were started on antacid treatment, and only 10 (6.4%) had a surgical intervention (i.e. supraglottoplasty). There were 59 (37.6%) patients who had a follow up sleep study: 48 (82.8%) showed improvement versus the initial PSG. The 33 participants who had no intervention had a follow-up PSG. The overall AHI decreased significantly on the repeat PSG with an average AHI decrease of 6.4 events per hour (p=0.0018). The REM AHI decreased by an average of 11.4 events per hour (p=0.0074), and the arousal index decreased by an average of 5.6 arousals per hour (p=0.0004). The peak ETCO2 and TST <SpO2 90% did not significantly change.
Discussion
We correlate the clinical severity of LM using the International Pediatric ORL Group Consensus Clinical Classification and Groningen system endoscopic types and to relate these to diagnostic parameters of VFSs and PSGs for more objective measures and outcomes. These data can improve patient-centered care in patients with LM. In 2012, our institute had a large cohort of patients (n=617) who presented with stridor/noisy breathing secondary to suspected LM. Of this group, 157 met our inclusion criteria. We excluded patients with significant comorbidities because those may contribute to the severity of LM and affect surgical outcome for patients requiring surgical intervention per literature review. In our practice, most patients with suspected LM underwent comprehensive evaluation to rule out significant comorbidities (aspiration, GER, and sleep-disordered breathing) that might influence disease severity. Endoscopic evaluation was performed in all patients with LM. The VFSs were completed to assess feeding difficulties when clinical history suggested potential dysphagia. Polysomnograms were performed in the vast majority of patients. Follow-up testing was performed in subsets of patients to objectively monitor their improvements after appropriate intervention.
We used the Groningen LM classification system published in 2015 as part of our correlation between the LM clinical severity and types.21 We reviewed the endoscopic images/video for every patient with stridor to identify the type of LM. We then evaluated the association between the LM clinical severity classification and endoscopic types of LM. We could not predict the endoscopic type based on the clinical presentation of LM, this might be due to the overlap between the different endoscopic types that could be seen during the endoscopic evaluation. Patients may have 2 different endoscopic types during the same evaluation (namely arytenoid prolapse and epiglottic prolapse). Here, the reported type was either the more severe type of LM observed or the type that was associated with stridor at the time of endoscopic evaluation.
While the severity of the clinical manifestation of LM did not correlate with the different endoscopic types, having cyanosis is one of the presenting symptoms of LM (under severe LM classification). This was associated with type III LM (epiglottic prolapse) and was shown to be similar to a prior small study where epiglottic prolapse correlated with the clinical severity of LM.12
Our study confirmed the coexistence between feeding difficulties and LM as well as a complicated clinical course. The improvements in LM symptoms on anti-reflux therapy were reported as previously shown in multiple case series and reports.13,14
Most patients in this study with moderate and severe LM and more than half of the patients with mild LM had PSG completed (80.1%). Previous small studies showed a contribution of LM to OSAS, and PSG may be useful in the evaluation of patients with LM to identify OSA.15-17 Polysomnogram can also objectively monitor outcomes especially after surgical intervention in those with severe LM. This is the largest cohort patients with LM with PSG completed. No prior studies included PSG data in patients with mild LM. Obstructive sleep apnea syndrome with sleep-related ventilation and oxygenation issues were significantly associated with the clinical severity of LM. The significant association between the overall AHI and clinical severity could be related to age at PSG more than the clinical severity. This is because most patients with severe LM present earlier, and those patients may have other maturity issues that can interfere with the severity of OSA, especially when no significant sleep-related oxygenation/ventilation issues are noted. Clinical management of patients with LM varies based on the clinical severities of LM with observation/monitoring in mild cases starting with anti-reflux medications for moderate cases of LM with feeding difficulties and surgical intervention. Surgery is reserved for subjects with severe cases associated with apnea, failure to thrive, and respiratory distress.
We have confirmed what was suggested in prior studies regarding the clinical course and management of LM.3,7 The vast majority of patients did not need medical or surgical therapy and could simply be observed clinically. A high percentage were started on anti-acid therapy with improved symptoms. Nearly half of the patients with severe LM underwent supraglottoplasty (<10% of the total cohort of patients).
The range of the time to resolution of LM symptoms varied as seen in prior studies, but all patients in this cohort had improved stridor, respiratory, feeding, and sleep-related behavior regardless of the type of intervention in less than 12 months. There were faster improvements in subjects with a supraglottoplasty performed and objectively monitored by follow up sleep study and VFSs. Prior studies have only looked into follow-up PSGs that were completed only post supraglottoplasty that showed significant improvement in AHI. Our study had follow-up PSGs performed on patients where no intervention was performed. The results showed significant improvements indicating the natural progression of the disease for these patients suggesting spontaneous improvements over time.
Study limitations
First it is retrospective. Second, at our institution, these patients are seen by pediatric pulmonologists or otolaryngologists (or both) based on individual patient health needs. Decisions about clinical management are based on the clinical discretion of the pulmonologist or otolaryngologist. We also included patients from 2012; this year had the largest group of patients with LM who underwent endoscopic evaluation along with PSG and VFSS. Finally, this is the experience of a single center, and practices may vary between centers. Evaluation by PSG may not be the standard of care in other institutions. Our goal here was to share our experience with LM evaluation and to determine if more testing can better identify subjects at high risk.
In conclusion, we found that the severity of the clinical manifestations of LM did not correlate with the different endoscopic types. The presence of cyanosis, one of the presenting symptoms in severe LM classification based on IPOG LM consensus, was associated with type III LM based on the Groningen classification. Rapid eye movement AHI and EtCO2 in PSG was significantly associated with clinical severity even after adjusting for age but not with different endoscopic types. In a small subset of patients, repeat sleep studies showed improvements in AHI/REM, AHI, and AI even if no intervention was performed. These findings indicate that the natural history of LM improves with time. This pilot study warrants a larger, prospective, and controlled study to validate these findings.
Acknowledgment
We would like to thank American Manuscript Editors (americanmanuscripteditors.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 3, 2019.
- Accepted February 20, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.