


Abstract
Objectives: To systematically review the literature and to summarize all evidence related to the diagnosis and management of patulous eustachian tube.
Methods: The present study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Results: Overall, 59 articles were retrieved and included in the analysis. Studies investigating treatments enrolled 1279 patients collectively, with follow-up duration varying from few days and up to 2 years. Eight studies reported medical treatments with intranasal saline instillation as the most frequently studied option. Other studies reported various surgical treatments varying from simple tympanostomy to invasive procedures targeting the orifice of the ET or the anatomical features surrounding it. In addition, 10 studies including 367 subjects investigated different diagnostic methods.
Conclusion: Currently, there is a wide spectrum of diagnostic and therapeutic interventions with minimal clinical efficacy, a persistent lack of systematic guidelines, and several gaps in previous research endeavours.
PROSPERO REG. NO. CRD: 1644000
Patulous eustachian tube (PET), a benign, largely idiopathic, condition, was first described in 1867. It has adverse effects that can markedly affect quality of life such as abnormal autophony, breathing, or hearing.1 Several factors have been reported to be causative, including pregnancy, neurological disorders, weight loss and radiotherapy, and some medications including oral contraceptives and diuretics.2 In terms of pathophysiology, all stressors that distort normal closure of the eustachian tube (ET) during the resting state can result in PET. This includes conditions affecting the elasticity, surface tension, and opening pressure of the ET.2
According to experts, there is currently a lack of universal consensus regarding symptom scores, tests, and guidelines to diagnose PET. Meanwhile, the diagnostic approach relies primarily on clinical assessment of the presenting symptoms.3 This non-systematic approach makes the identification of these cases challenging. Symptoms that should raise suspicion include aural fullness, popping, and discomfort or pain, in addition to autophony of breathing or voice. Signs include tympanic membrane retraction and signs of negative middle ear pressure.3,4 Further studies have been recommended to enhance the diagnostic approach to this condition.
Despite the modest rarity of PET and the hurdles to diagnose, it also represents a challenging condition for patients and clinicians due to limited therapeutic options.5 Current approaches vary depending on the severity of symptoms and range from informative reassurance to invasive interventions. Some cases may need combined or surgical treatment such as those with no clinical improvement and persistent movement of the tympanic membrane.6 To date, there have been limited research papers with variable outcome measures and no definite recommendations that outline a precise evidence-based, patient-centered therapeutic guideline.3,5
Given the insufficient diagnostic and therapeutic guidelines, we aim to systematically review the literature and to summarize all evidence related to the diagnosis and management of PET.
Methods
This study has followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.7 The study protocol was applied for recording in PROSPERO. Provided the nature of the present study (example, systematic review), requirements for ethics review were waived.
Any primary study that reported or investigated diagnostic approaches or management options for PET were included. There were no restrictions regarding different populations, race, origin, age, ethnicity, language, or publication date. However, letters, editorial comments, theses, book chapters, non-human and experimental studies, and articles with no available full text were excluded. Studies with no extractable data were also excluded.
A computerized systematic search was performed for potentially eligible articles published up to December 2019 using the PubMed, Scopus, ISI Web of Science, Embase, Virtual Health Library (VHL), and Cochrane Central Register of Controlled Trials databases. The search term “patulous eustachian tube” was used to retrieve all relevant articles within the scope of the present study. A manual inspection of the reference section of all competent reports was also considered to recognize any further articles. Search results were retrieved and duplicates were removed using EndNote X7.4 (EndNote, USA) for Windows (Microsoft Corporation, Redmond, WA, USA). Two independent reviewers screened potentially relevant articles and included all reports that met the research criteria. Initial screening of titles and abstracts was followed by full-text review. Disagreements were resolved by discussion and consensus between reviewers and among senior researchers.
Three authors independently collected the target outcomes from the eligible articles and filled it into blind Excel sheets. Any discrepancy was resolved by discussion to reach consensus. The extraction form was established using a pilot extraction of a few blindly selected studies. Extracted outcomes comprised demographic informations of the enrolled subjects. In addition, different types of therapeutic and diagnostic approaches, and follow-up period were analyzed. Complete, partial, and non-resolution rates were also compared. Descriptive statistics was carried out and the data were presented as numbers and proportions.
Results
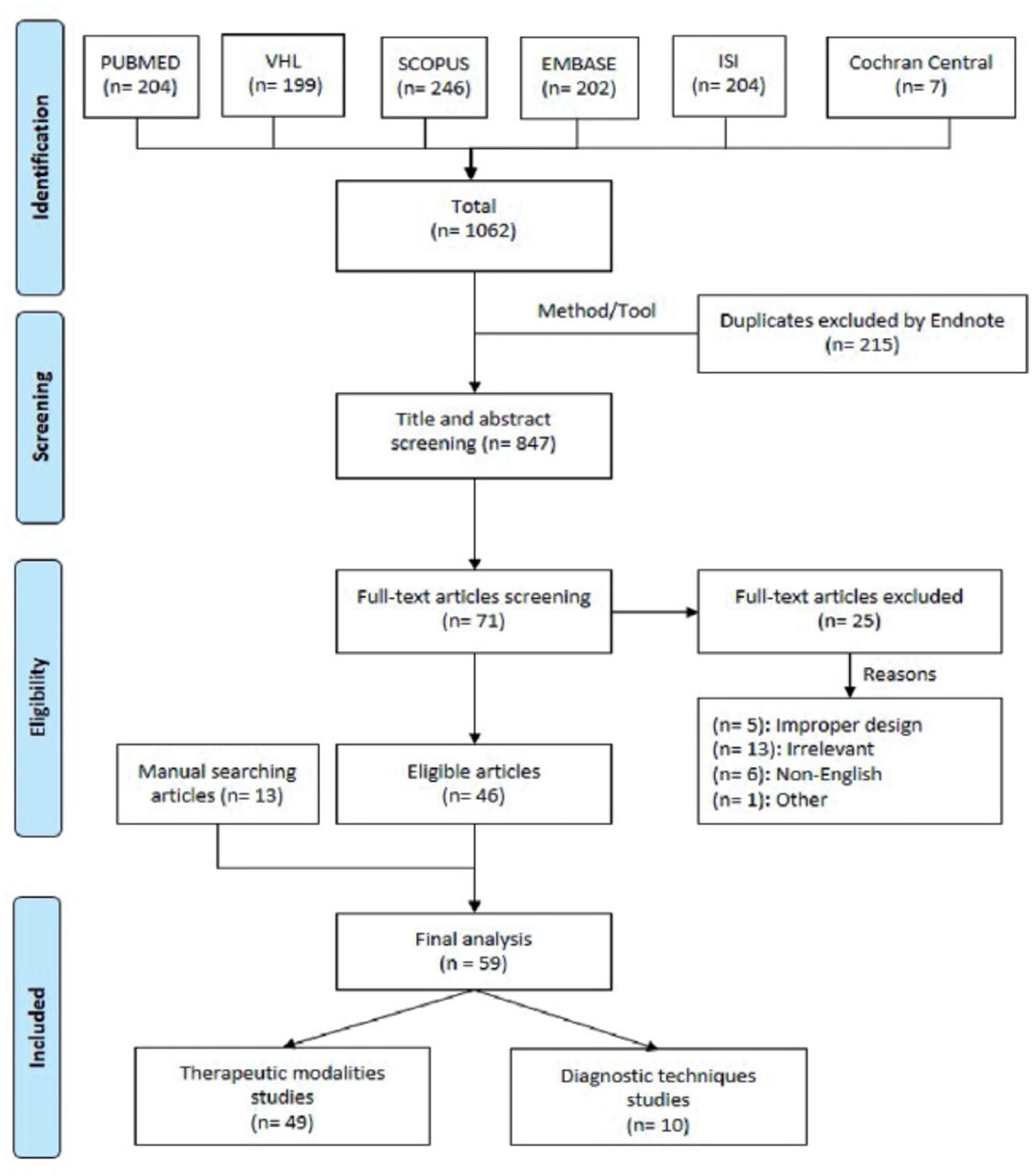
The search of the medical literature retrieved 1062 titles (PubMed [n = 204]; VHL [n = 199]; Scopus [n=246], Embase [n=202], ISI Web of Science [n=204], Cochrane Central Register of Controlled Trials [n=7]). After removing 215 duplicates, 847 titles and abstracts were pooled for initial screening (Figure 1). Three reviewers working independently selected 71 articles for full-text screening. After discussion, 25 articles were excluded for irrelevance or improper design, among other reasons (Figure 1). Ultimately, 46 articles were eligible by screening and 13 were identified through the manual search, resulting in 59 articles included for data extraction and analysis.

PRISMA flowchart of studies selection and screening. ISI: Web of Science, VHL: virtual health library
Of the 59 included studies, 49 investigated treatment options, while 10 described diagnostic approaches.8-54 The studies investigating treatments collectively enrolled 1279 patients (1442 ears), with follow-up intervals varying from 2 weeks to 2 years. Baseline demographics of the enrolled articles are summarized in Table 1.
Baseline characters of 49 studies reporting treatment of patulous eustachian tube.
Medical treatment approach
Eight articles described several non-surgical, intranasal or intratubal treatments (Table 2). Treatment options included guidance to stop sniffing and nasal saline instillation, irrigation using normal saline, potassium iodide, diluted hydrochloric acid, beta chlorobutanol, benzyl alcohol, atropine, 1:4 salicylic acid powder, boric acid powder. The latter was reported in 3 studies enrolling 40 patients, which led to a 100% resolution of PET symptoms.48,53,54 Irritation was the only side effect reported. More recent studies favored the use of topical normal saline with high efficacy (65.7% experienced complete resolution in the study by Ikeda9) and safety (example, no adverse events were reported with the use of saline drops).
Outcomes from 8 studies reporting treatment of patulous eustachian tube through medical approach.
Tympanic membrane mass loading approach
Several techniques were used to increase the mass of the tympanic membrane, which is aimed at decreasing its movement and, therefore, potentially improving PET symptoms. In the review, 10 studies reported different means to load the tympanic membrane, which are summarized in Table 3. These techniques included paper patching, loading with ventilation tubes, cartilage chip insertion, myringoplasty, potassium-titanyl-phosphate (KTP) laser, and loading with blue tack. Complete resolution was more frequently reported with the use of blue tack (78.6%) in a sample size of 11 subjects, and paper patching (65.2-76.2%) in 44 patients (56 ears). The side effects of paper patching were limited to mild to moderate discomfort.
Outcomes from 10 studies reporting treatment of patulous eustachian tube through tympanic membrane mass loading approach.
Eustachian tube occlusion approach
Ten studies investigated ET occlusion using several modalities including plugging (example, silicon plug, catheter with bone wax, and orifice suturing), cautery, and injections. The outcomes of these reports are elaborated in Table 4. The largest sample size was reported by Kikuchi et al,14 in which 252 ears were occluded using Kobayashi plug, with a complete resolution rate (CRR) of 64.7% and several reported side effects including tympanic membrane perforation (17.5%) and plug dropping toward the pharyngeal tube (22.6%). Cauterization was reported in 3 case series including 22 patients. Several techniques and resolution rates are summarized, with otitis media as the only reported side effect. Various types of injectable elements used for inducing ET occlusion are also summarized in Table 4. Those with the largest sample sizes included autologous cartilage injection (33 ears [CRR 27.3%]), soft-tissue bulking agent (26 ears [CRR, 35%]), calcium hydroxyapatite (23 ears [CRR 57-63%]), absorbable gelatin sponge solution (22 ears [CRR 100%]), and Teflon (26 ears [CRR 73.1%]). Otitis media with effusion, epistaxis, tinnitus, and temporomandibular joint discomfort were reported as adverse events post-injection.
Outcomes from 10 studies reporting treatment of patulous eustachian tube through eustachian tube occlusion.
Muscular techniques
Modulating the tone of the tensor veli palatine muscle can change the patency of the ET and was investigated as a potential therapeutic approach to PET. Appendix 1 summarizes relevant evidence. The most commonly investigated technique was tensor veli palatine transection or transposition with pterygoid hamulotomy, which was reported by Virtanen (44) on 16 ears, with a CRR of 56.2%.
Diagnostic approaches
Ten studies including 367 subjects investigated various diagnostic methods.55-64 The various diagnostic options summarized in this review (Table 5) include the 678 Hz acoustic immittance probe tone of GSI TympStar Middle Ear Analyzer (Grason-Stadler, Eden Prairie, MN, USA), patient-reported outcome measure (PROM), sonotubometry acoustic click stimulus, nasal-noise masking audiometry (NNMA), computed tomography in the sitting position, and sonotubometry.
Summary of 10 studies reporting different applied diagnostic methods of patulous eustachian tube.
Discussion
Patulous eustachian tube is a modestly prevalent condition that impacts the quality of life of affected individuals. The recognition of and approach to this condition is usually challenging due to the highly subjective nature of the disease and various management options that fail to be consistent in terms of clinical efficacy.3 The present systematic review summarized therapeutic and diagnostic options published in the literature, updated previous work in this field, and included more studies and approaches compared with previous reviews. Although the diagnosis of PET is mainly clinical, several approaches have been proposed to confirm the diagnosis.3 This is significant because symptoms can be nonspecific or misleading in some instances, especially autophony, which is often incorrectly regarded as a pathognomonic sign of PET, while several other conditions may precipitate it, such as external ear canal occlusion, superior canal dehiscence, and foreign bodies such as hair or wax.1,65 These approaches are also important for persistent treatment-resistant cases and for research purposes.66 Thus, having a consistent diagnostic approach is important for clinical studies that investigate various management options, and for synthesizing comparative evidence. Meanwhile, there is still no gold standard for diagnosing PET. The most commonly reported approach is computed tomography in the sitting position with or without the Valsalva maneuver, which is used to detect any anatomical patency and measure open tubal distance.60,61 It remains; however, costly, and not readily available in all healthcare centers. Sonotubometry, tympanometry, and audiometry, along with other approaches, that may or may not need special equipment, were summarized in this review to emphasize the need for a tailored, case-specific approach that combines clinical assessment with diagnostic tests to detect PET. Given the results and nature of the included studies, this appears to be better than standard tests. More research is, nevertheless, needed to inform and develop future guidelines.
In terms of therapeutic approaches, several medical and surgical interventions were suggested, none of which, however, proved to be consistently effective.67 Our review highlights the lack of randomized controlled trials and the need for more interventional studies. Non-surgical interventions mainly include the intratympanic or intranasal administration of different agents. Most recent studies have focused on the role of saline instillation for symptom relief in those with PET.28,32 Intranasal saline was suggested as the initial step in the management plan due to its moderate to high efficacy and clean safety profile.32 However, confounders such as instructing patients to stop sniffing were reported, especially in those with PET and habitual sniffing, which need to be accounted for in future studies. Similar to previous systematic reviews, we failed to find any evidence supporting the use of nasal estrogen cream to treat PET.67
Patients with no clinical improvement and persistent movement of the tympanic membrane may be candidates for combination therapies or surgical treatment.6 The wide spectrum of surgical interventions mainly targets the tympanic membrane, ET orifice or the surrounding anatomical features, and range from simple to invasive procedures. Again, surgical approaches are limited by the lack of consistency of clinical efficacy, scant descriptions of the details of some procedures, and the primitive evidence that we still have in this area. For example, the outcome of “partial resolution” was not consistently defined among the studies.
Our results highlight several additional challenges that impede a more informed approach to PET. Some of these challenges are specific to the nature of the condition, such as the scarcity of objective outcomes and that symptoms can be self-limited, which is an important confounder in research studies. Other challenges leave room for improvement through further research and interventions. They include small sample sizes, high risk of bias, unmatched confounders, poorly defined follow-up periods, and poorly described intervention(s), in addition to the lack of clinical trials and guidelines for diagnosing and managing PET. The present systematic review was limited by the lack of quantitative meta-analysis and the exclusion of non-English articles due to a lack of native speakers.
In conclusion, the present systematic review is the most recent comprehensive investigation of diagnostic and therapeutic approaches to PET to date. It revealed a highly variable spectrum of choices, with a lack of systematic guidelines and several gaps in current research endeavours. As such, a case-specific, step-wise approach is recommended.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 25, 2020.
- Accepted April 9, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.