


Abstract
Objectives: To report the epidemiology of chronic kidney disease (CKD) in neonates at a single tertiary center and the outcomes of renal replacement therapy (RRT) in these patients and discuss ethical considerations regarding RRT in this population.
Methods: In this retrospective study, we reviewed clinical data from all neonates with evidence of CKD who were followed up at King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia between 2005 and 2015. Follow-up serum creatinine levels were recorded every 6 months.
Results: A total of 181 neonates presented with CKD. Their mean age at the time of presentation was 11.1 days (95% confidence interval [CI]: 9.5-12.8) and the mean creatinine level was 106.5 µmol/ (95% CI: 91.3-121.7). Congenital anomalies of the kidneys and urinary tract (CAKUT) were the underlying causes of CKD in 84.5% of the neonates. Mortality was high, particularly in the first 6 months (10%), and reached 16% by 4 years of follow-up. At the time of the last follow-up, 42 (41%) neonates had hypertension and 27 (26.5%) had significant proteinuria. Five patients received dialysis in the neonatal period and another 6 were commenced on dialysis later.
Conclusion: Congenital anomalies of the kidneys and urinary tract is the most common etiology in neonates with CKD. Chronic kidney disease in neonates is associated with high morbidity and mortality rates.
Information about the epidemiology of chronic kidney disease (CKD) in neonates and infants is limited worldwide.1,2 These patients require special attention, as the characteristic features of CKD in these patients differ from those of children older than 2 years. Furthermore, the need for dialysis among neonates with severe CKD should be considered carefully from medical and ethical points of view.2 Congenital anomalies of the kidneys and urinary tract (CAKUT), particularly obstructive anomalies and renal dysplasia, are the most frequent underlying causes of CKD during the neonatal period.3,4 Chronic kidney disease in neonates requiring renal replacement therapy (RRT) is very rare. In a survey, conducted between 2000 and 2011, of patients on chronic dialysis in 32 countries, only 264 neonates had received RRT.4 Delivery of RRT is influenced by the uncertain outcomes of chronic dialysis in neonates.4 As a result, there is significant variation in the attitudes of pediatric nephrologists caring for infants with end-stage kidney disease (ESKD).5 In addition, the economic impact of RRT leads to major regional variation in its use globally. For example, more neonates with ESKD receive RRT in countries with a higher gross national income than those in countries with a lower gross national income,5 which is likely influenced by the high cost of providing RRT to young children.6,7 The challenges faced by pediatric nephrologists in developing countries are even greater due to limited facilities and cultural issues. However, there is a paucity of studies about CKD in neonates in these countries.
In this study, we reported the epidemiology of neonatal CKD and outcomes of RRT in these patients at our institution. We also discussed cultural and ethical issues regarding the provision, or lack thereof, of life-sustaining RRT treatment for neonates.
Methods
Compliance with ethical standards
The Ethics Research Committee at the Faculty of Medicine of King Abdulaziz University (KAU), Jeddah, Kingdom of Saudi Arabia provided us permission to perform this study. The need to obtain consent from the participants was waived, as we studied anonymous subjects retrospectively and we did not perform any interventions. The study was performed according to the ethical principles of the Declaration of Helsinki.
Study population and data collection
Data of all fullterm neonates, either born at or referred to King Abdulaziz University Hospital, with evidence of CKD between January 2005 and December 2015 were evaluated. Low-birth-weight neonates (premature and small for gestational age) or neonates with acute kidney injury that had resolved were excluded.
Data were collected retrospectively from the patients’ medical records and included age at the time of presentation, gender, neonate length at presentation, etiology of CKD, associated comorbidities, blood pressure (BP), serial serum creatinine level, hemoglobin level, urine protein level, and mortality.
For subjects with stage 5 CKD (ESKD), we recorded details about RRT, including reasons for it not being performed in neonates who did not receive RRT.
Subjects aged 1-28 days were considered to have been born in the neonatal period. Hypertension was defined as an elevation in systolic blood pressure ≥95th percentile for gestational and post-conception age and the birth weight, measured on 3 separate occasions.8,9 Babies with normal BP readings on antihypertensive were considered hypertensive.
We defined neonatal CKD as an abnormality in renal structure or function that manifested in the neonatal period and was long term or expected to last for more than 3 months. Significant proteinuria was defined as an early morning urine protein level of 30 mg/dL or greater.10
We determined the estimated glomerular filtration rate (eGFR) using Schwartz’s11 formula for infants. The related studies, which have been referred to throughout our study were obtained from a variety of reliable online databases such as WebMD and PubMed.
Statistical analysis
We used STATA software (StataCorp. 2011: Release 12. College Station, TX: StaCorp LLC) for all analyses. The proportion and mean for dichotomous and continuous variables, respectively, were measured to describe the patients’ characteristics. The 4-year survival was estimated using a Kaplan-Meier curve. The impact of the severity of disease and RRT on the 4-year mortality was estimated using a Cox proportional hazards regression model. A multivariate regression analysis was performed to control for potential confounding factors, including baseline age, gender, and hypertension, which were determined based on an a priori theoretical assumption using directed acyclic graphs. All patients, including censored patients, with a determined follow-up duration were included in the survival analysis. Statistical significance was determined with a p-value of 0.05, and data are presented as 95% confidence intervals (CIs).
Results
One hundred eighty-one neonates fulfilled our inclusion criteria and were included in the study. They represented 14.25% of our pediatric CKD population (1,270 children with CKD). Their baseline demographic and disease characteristics are summarized in Table 1. There was a predominance of male patients, and obstructive uropathy was the main underlying etiology of CKD. Data on consanguinity were available for 77 children, of whom 53 (69%) had a history of consanguinity between parents.
Baseline demographic and disease characteristics of the study participants.
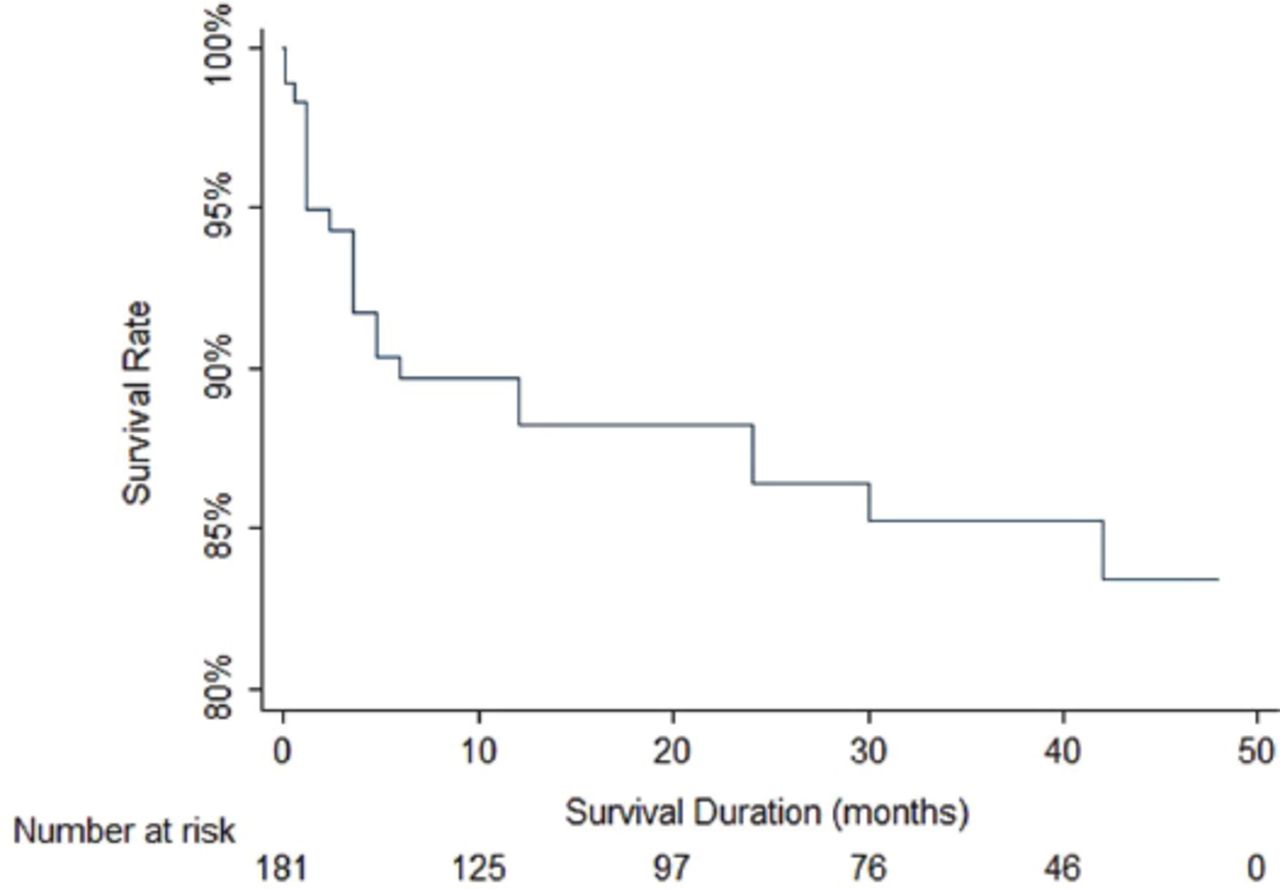
Figure 1 demonstrates patient survival over the course of 4 years, with considerable mortality within the first 6 months of life (10%).

Patient survival over the course of 4 years, with considerable mortality within the first 6 months of life (10%).
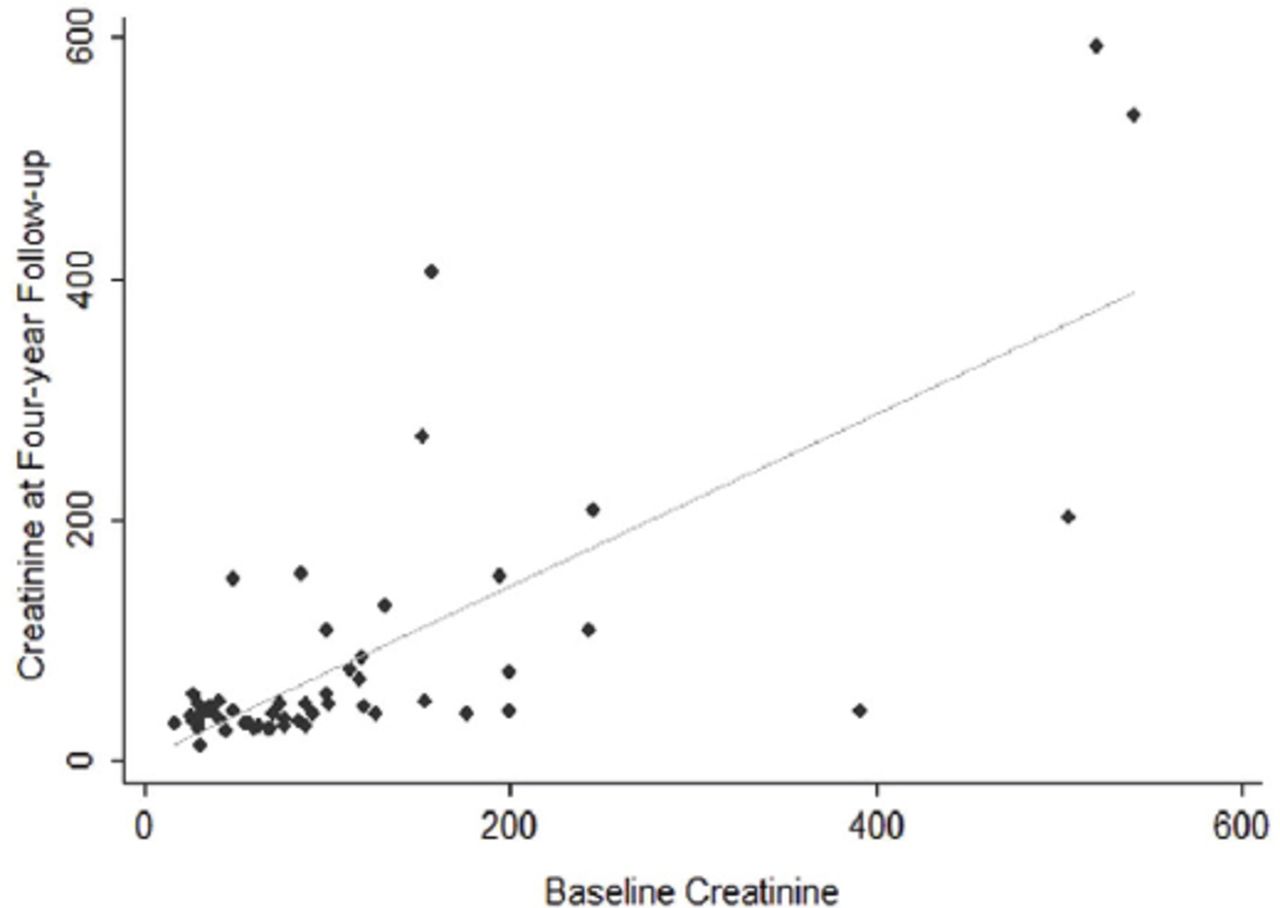
Although the baseline creatinine level did not influence the 4-year mortality (hazard ratio [HR]: 1.004; 95% CI: 1.001-1.007; adjusted for age, gender, and baseline hypertension), it significantly influenced the risk of long-term renal impairment (the 4-year creatinine level increased by 0.7 µmol for each 1 µmol increase in the baseline creatinine level; 95% CI: 0.54-0.90; adjusted for age, gender, and baseline hypertension [Figure 2]).

Effect of baseline creatinine on long-term creatinine level among neonates with renal impairment.
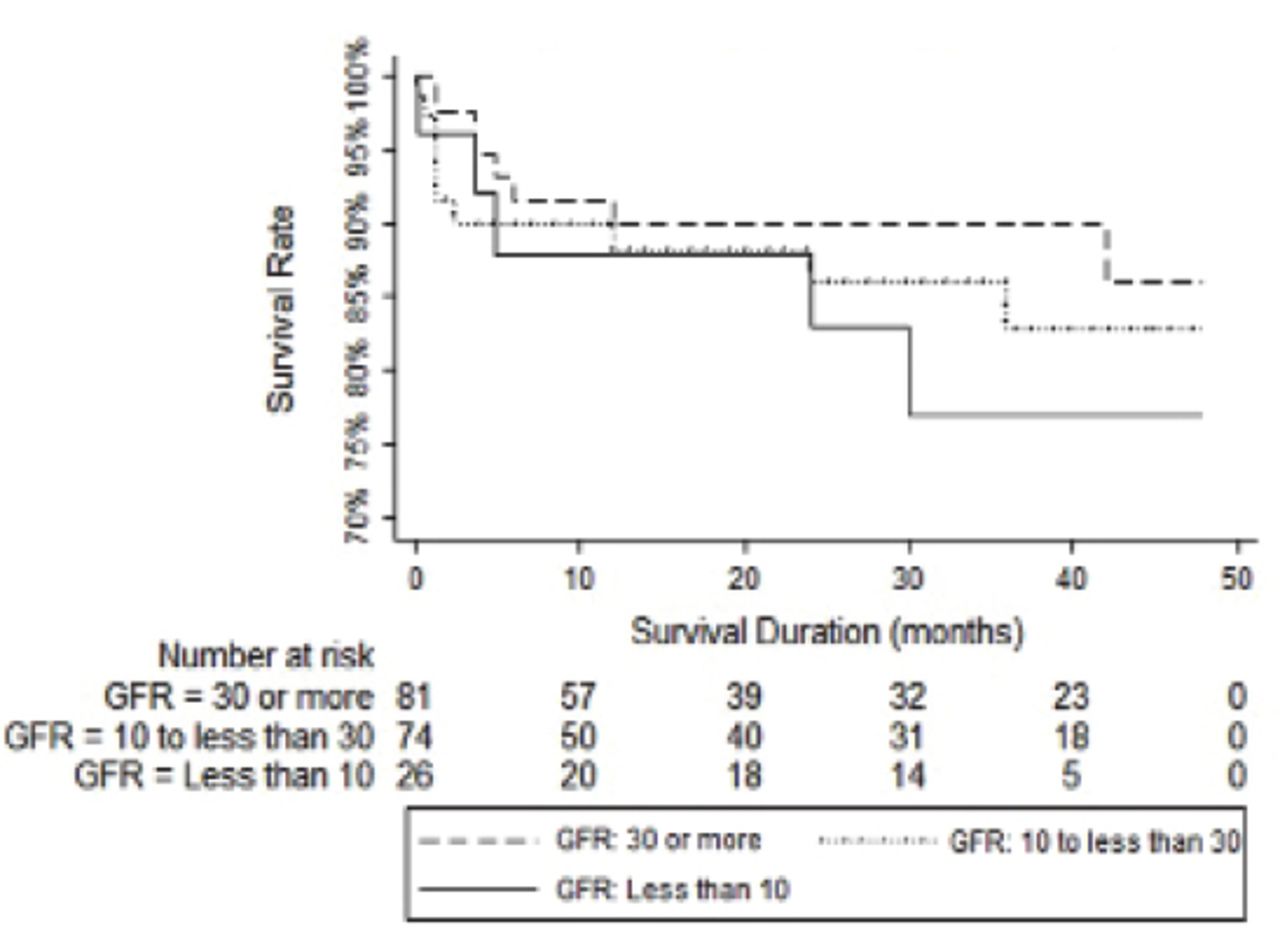
Similarly, the baseline eGFR did not significantly influence the 4-year mortality (HR: 0.98; adjusted for age, gender, and baseline hypertension; 95% CI: 0.95-1.00) (Figure 3).
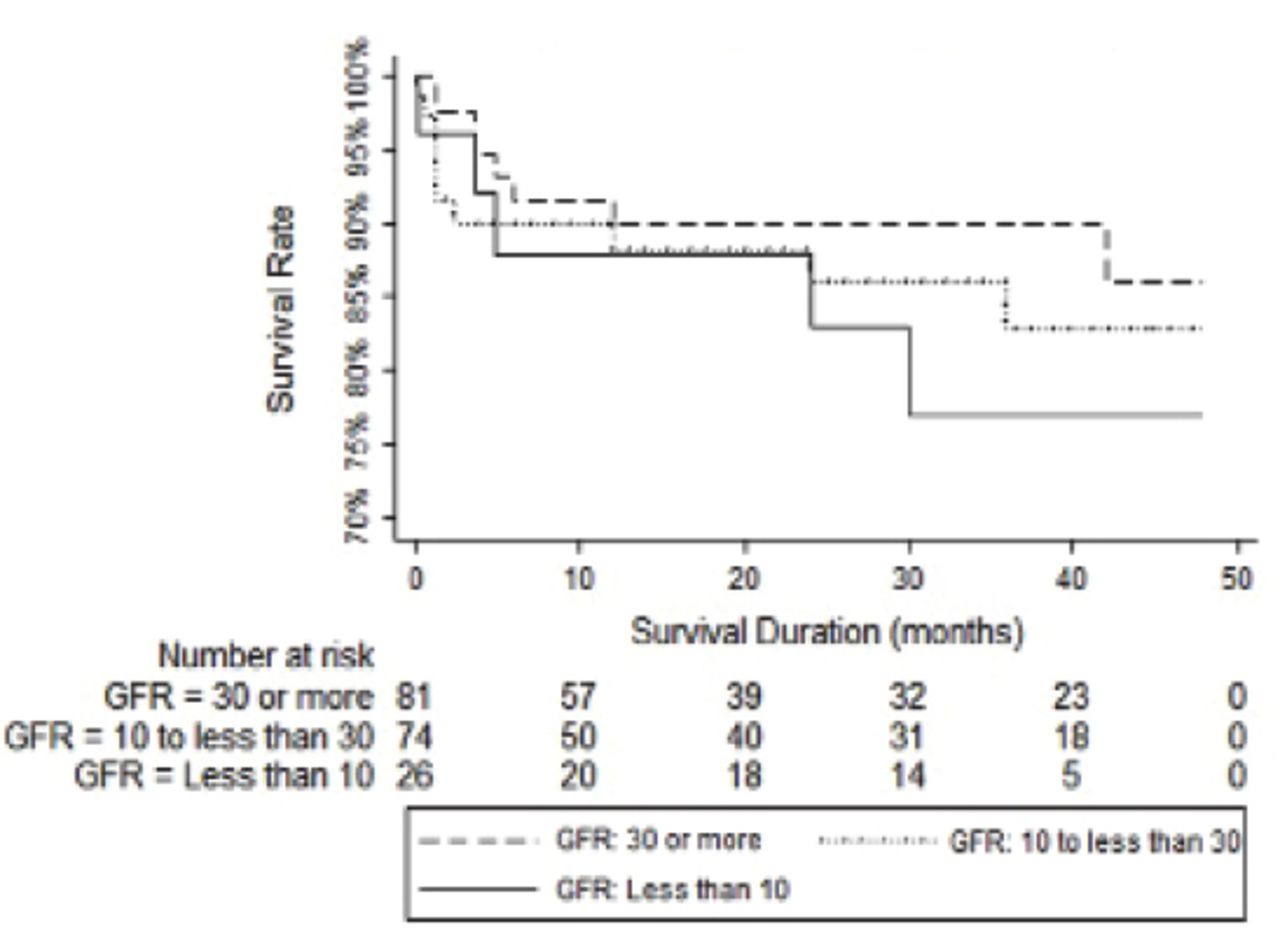
Four-year survival among neonates with renal impairment, stratified by the severity of disease at presentation. GFR - glomerular filtration rate.
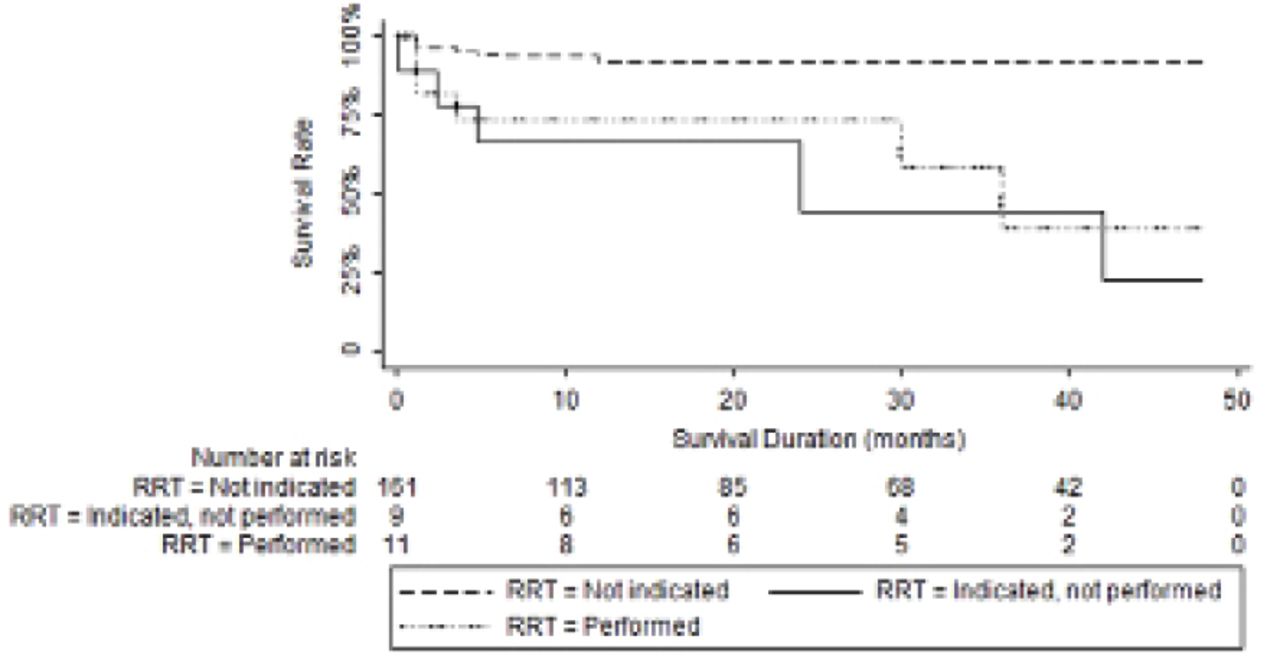
Five of 39 neonates with a serum creatinine level greater than 133 µmol/L received RRT. An additional 6 children underwent dialysis later in infancy or childhood. The parents of 3 patients refused to allow their child to undergo dialysis because of social issues or because a family member had a bad experience with dialysis; moreover, we advised 6 patients with comorbidities not to undergo dialysis. The indication and decision to perform RRT significantly influenced neonatal mortality (Figure 4). The need for dialysis was based on the serum creatinine level, eGFR, and symptoms such as fluid overload.

Four-year survival among neonates with renal impairment, stratified by requirement and performance of renal replacement therapy during. the follow-up period.
Details on the patients who received RRT during the neonatal period or later in infancy and those who did not receive RRT, despite having ESKD, are summarized in Table 2.
The clinical details of patients with ESRD who received RRT and those who did not during the neonatal or infancy periods.
At the time of the last follow-up, 42 (41%) children had hypertension and 27 (26.5%) had significant proteinuria. Twenty-two children (12.1%) died at mean (SD) age of 8.8 (11.2) months, median (range) 4.3 (0.14-42) months. The underlying cause of death was variable; however, chest infection and septicemia were the main underlying etiology of death in 6 patients who had congenital nephrotic syndrome. Progression and complication of the ESKD leading to other systems failure was the cause in the remaining children.
Discussion
We reported the epidemiology of CKD in neonates presenting to our institution over the course of 10 years. Congenital anomalies of the kidneys and urinary tract was the main underlying cause of CKD in our patient group, consistent with the results of other international reports.3,4 A combined database study representing 40 countries and 264 patients showed that the most frequent underlying etiology of neonatal ESKD was CAKUT in 55% of patients, followed by cystic kidney disease in 13%, cortical necrosis in 11%, and congenital nephrotic syndrome in 6%.4 The incidence of neonatal ESKD was reported to be about 7.1 per 1 million age-related people, and the estimated incidence of neonatal CKD being 1 in 10,000 live births.12 In our cohort, we observed a high percentage of consanguinity, which is similar to that seen in the rest of our country.13
In our cohort, only a small percentage of neonates required RRT, and this treatment was offered to only a few children in the neonatal period. Some parents refused to allow their child to undergo dialysis for various reasons, while others were advised against dialysis. The contraindications for dialysis included neonates with associated anomalies or poor social background and parental inability to perform peritoneal dialysis at home.
Apart from the presence of anuria, there are no clear indications for the initiation of dialysis in neonates with CKD. Many infants, especially those with CAKUT, have ongoing urine production, and their condition may be managed without dialysis until they have recovered from respiratory complications, which are common in neonates with CAKUT. Some patients may show a surprising improvement in kidney function, as RRT can be discontinued in 10% of neonates who have been commenced on dialysis.4 There is no international agreement on who should be responsible for clinical decision-making regarding the initiation of dialysis therapy in pediatric patients who are unable to provide consent. The United States Presidential Commission for the Study of Bioethics14 has divided ethical issues about providing treatment into 3 categories. First, for clearly beneficial treatments, the guidelines state that treatment is mandatory, even without parental consent. Second, for clearly futile treatments, the guidelines state that treatment should not be provided, even if parents insist upon treatment. Finally, when outcomes are ambiguous or uncertain, the parents should assume final responsibility regarding the most appropriate course of action. However, the French Neonatology Society15,16 recommends that although parents must be involved in the decision-making process, any important decision affecting the patient’s life is an individual medical responsibility.
In our institution, we provided RRT to neonates in whom RRT was not advised by physicians due to the presence of other comorbidities but whose parents insisted that all possible treatment options be tried. However, their outcome was poor. Some Islamic scholars17 have advised (fatwa) that life-sustaining treatment such as resuscitation should be withheld or withdrawn if recovery of the heart and lungs is deemed unlikely in the opinion of 3 trustworthy specialist doctors. Similarly, the Royal College of Pediatrics and Child Health in London18 recommends that it is ethically acceptable to withhold a treatment that is not in a child’s best interest. This is the case in many neonates with CKD requiring RRT, as this therapy could prolong their suffering, with no improvement in the outcome. This scenario is particularly true when the infrastructure is not optimum for providing this expensive treatment. In this case, withdrawal (or withholding or limiting) of treatment could be ethical because a greater benefit could be achieved by using other resources.19
It is also important to consider social issues when making decisions about the use of RRT in neonates. For example, clinicians should consider whether parents are able to provide peritoneal dialysis for neonatal patients at home prior to recommending such sophisticated treatment. Serious medical abnormalities are the most important factor affecting decision-making when providing RRT to neonates with ESKD. Other factors include anticipated future morbidity, the family’s right to decide, the doctor or medical staff’s right to decide, family socio-economic status, oliguria, and budget constraints.16 In this study, we used only peritoneal dialysis (PD) to start RRT, as we do not have the facilities to perform hemodialysis or renal transplantation in neonates at our institution. Peritoneal dialysis was used in 91.7% of the 264 neonates registered to receive RRT in the European Society of Pediatric Nephrology (ESPN)/European Renal Association-European Dialysis and Transplant Association (ERA-EDTA), International Pediatric Peritoneal Dialysis Network (IPPN), The Australia and New Zealand Dialysis and Transplant Registry (ANZDATA), and Japanese RRT registries.4 Recently, data have shown that the survival of neonates receiving RRT improves when appropriate infrastructure and expertise are available. The survival of neonates and infants who received RRT early in life in the form of PD 3 years after dialysis initiation was 78.6% and 84.6%, respectively.20 Neonatal RRT is associated with significant morbidity and mortality. A recent study21 reported that there were high rates of complications, including peritonitis (83%), malpositioned catheters (72%), and leaks (55%), after PD in neonates. An alternative option for long-term dialysis in neonates is hemodialysis. Poolack et al22 performed hemodialysis in 7 neonates, and reported that 86% (6 children) survived at 18 months of age, but there was considerable morbidity.
The results described here are consistent with those of a previous study demonstrating that there was a high mortality rate in neonates receiving RRT (65.3%), which was most likely within the first month of life (56%), with the majority (94%) occurring within the first year.20 Furthermore, among long-term survivors, 44% were severely developmentally delayed and 22% were moderately developmentally delayed. Higher survival rates were reported in combined registries (the ESPN/ERA-EDTA, IPPN, ANZDATA, and Japanese RRT registry): 81% at 2 years and 76% at 5 years.4 Nevertheless, considerable morbidities, including growth retardation (63%), anemia (55%), and hypertension (57%), were reported at 2 years of age.4 Similar to our report, another study found that the decision to begin RRT in neonates is difficult due to lack of the surgeon’s experience and evidence-based guidelines.21 The outcome of this treatment remains uncertain, and there are many ethical issues regarding the benefit of treatment in neonates with comorbidities and restricted resources. Over the last 20 years, many institutions in developed countries have begun to offer RRT routinely to neonates. However, this treatment is viewed as optional, rather than mandatory.23,24 This viewpoint is even more common in developing countries, as both medical staff and caregivers both feel that RRT is a demanding treatment with uncertain or poor outcomes. This explains the high percentage of parental refusal to start dialysis in our study. A similar situation of parents refusing therapy could occur with optimum infrastructure and expertise, leading to an ethical dilemma.25,26
Study limitation
The main limitation of our study is that it was a single-center, retrospective study in a tertiary pediatric nephrology center.
In conclusion, CAKUT is the most common etiology of CKD in neonates. Chronic kidney disease is associated with high morbidity and mortality in these patients. Further studies are required to justify offering complicated and expensive therapy to vulnerable children in developing countries and to create guidelines that help professionals make decisions about treatment.
Copyright
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
Acknowledgment
This project was funded by the Scientific Deanship of King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This project was funded by the Scientific Deanship of King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia (Grant Number G-385-140-38).
- Received December 15, 2017.
- Accepted March 19, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.