


Abstract
Objectives: To assess the knowledge levels of dental hygienists in Saudi Arabia regarding the association between systemic and oral disease in addition to evaluating their attitude about integrating this knowledge into clinical practice.
Methods: This was a cross-sectional survey using a questionnaire of 102 items among 192 randomly selected dental hygienists practicing in Riyadh, Saudi Arabia by individual interview. The research tool was pilot tested among 12 dental hygienists (8 females and 4 males) to obtain feedback about clarity and objectivity.
Results: The response rate was 83%, and the majority of respondents were female (77.5%). The respondents’ knowledge about the risk factors of cardiovascular diseases was better than other conditions. The level of education was considered to be a significant predictor in many items related to risk factors. More than the half, rated the evidence linking periodontal disease and diabetes mellitus as strong; however, the knowledge level of oral-systemic evidence was less than expected. A high percentage of the respondents were confident and comfortable managing patients with systemic conditions. Most agreed that dental hygienists must be prepared efficiently to manage medically compromised patients.
Conclusion: Dental hygienists in Riyadh, Saudi Arabia have low level of knowledge about the oral-systemic disease relationship. This study suggests that greater emphasis should be placed on this association in current and continuing education programs.
In the last decade, more emphasis had been placed in dental practice on the importance of oral health as an essential part of overall health and well-being.1 Furthermore, the association between oral health especially periodontal status and systemic conditions had been well established.2,3 Generally, the term “oral-systemic link” is widely used to refer to the association between oral and systemic health. Remarkably, oral examination can reveal more than 90% of systemic diseases.1,4 Moreover, the World Health Organization International Classification of Diseases and Somatology currently lists more than 120 diseases that have oral cavity manifestations.5 Consequently, the term “the mouth is a mirror” has been widely used to illustrate the intimate relationship between systemic and oral health.4
Many preceding studies indicated a lack of knowledge regarding the oral-systemic evidence among workers in the medical field.6,7 A study in the United States of America, revealed that 49% of participant obstetricians rarely or never recommended a dental examination; furthermore, only 9% examine their patients ‘mouth periodically.8 Another study among medical trainees and interns revealed that 90% of participants had never received any education about periodontal disease, and approximately 70% stated that they were not comfortable performing simple periodontal examinations.9 Similarly, another study conducted among certified diabetes educators’ (CDEs) in the United States of America demonstrated that oral health-related modules were not covered in the curricula of approximately 77% of participants. Furthermore, most respondents reported that they did not routinely provide oral health education to diabetic patients because of a lack of oral health knowledge.6 A survey of health professionals working in Riyadh, Kingdom of Saudi Arabia found that oral health knowledge among participants was poor. Fewer than 37% of participating medical doctors stated that dental plaque causes gingival inflammation.10
Thus, medical care providers in Riyadh, Kingdom of Saudi Arabia have limited oral health knowledge, and dental care providers have a greater responsibility in managing and predicting any oral-systemic disease complications. This is confirmed in a study by Forbes et al,11 in which the authors recommend that dentists must be more involved in the management of patients with diabetes. Although dental practitioners are not responsible for the diagnosis or treatment of systemic diseases, early detection will undoubtedly lead to better medical and dental outcomes.3,12
As the role of dentistry shifts from the diagnosis and treatment of carious teeth to include health promotion and education, knowledge of the oral-systemic disease association among oral health care providers is critical to achieve the aims of modern dentistry. Consequently, the responsibilities of oral health care providers have developed as well. One example of such a change over the last decades is in the dental hygiene profession. Previously, dental hygienists predominantly provided scaling and cleaning services. Today, the responsibilities of dental hygienists have expanded to include patient screening procedures, assessment of oral health conditions, oral cancer screening, and dietary counseling.13
While most previous studies assessed the knowledge and practices of dental practitioners regarding the association between systemic conditions and oral health, the role of dental hygienists was neglected.14 Relatively few studies have been conducted to explore knowledge and attitude of oral hygienists regarding the oral-systemic disease association, moreover, a thorough review of the literature has revealed the absence of similar studies in the Middle East and North Africa. A survey among American dental hygienists in North Carolina, United States of America, revealed that the participants had incorporated some aspects of the oral-systemic evidence into their practice; however, 50% were extremely likely to refer patients to a medical practitioner for follow-up.15 Another study in North Carolina, United States of America, found that dental hygienists had high knowledge level in some aspects of the oral-systemic disease association; further training was recommended in the areas of osteoporosis and pregnancy complications.14
The objectives of this study were to survey practicing oral hygienists in Riyadh, Kingdom of Saudi Arabia and to assess their knowledge regarding systemic diseases and related risk factors; assess their awareness regarding the association between periodontal disease and systemic conditions; and evaluate their attitude and behavior in clinical practice regarding the oral-systemic disease association.
Methods
Study design and data collection
The study consisted of a cross-sectional survey of 192 licensed dental hygienists practicing in either the public or private sector in Riyadh city, Kingdom of Saudi Arabia. The survey was conducted between January-April 2016. All procedures related to this survey were approved by the research and ethical committee of Al-Farabi College of Dentistry in Riyadh, Kingdom of Saudi Arabia and were in accordance with the principles of the Helsinki Declaration (IRB: OM; 0219). The survey was given out personally by 2 investigators to randomly selected dental hygienists. All participants were asked to sign an informed written consent prior to contribution.
Questionnaire development and description
The questionnaire was developed by the University of North Carolina at Chapel Hill, United States of America, to assess the knowledge, attitude, and behavior among dentists and dental hygienists in the United States of America regarding the oral-systemic disease relation when managing medically compromised patients.14,16 However, in order to assess the validity and reliability of the questionnaire in the Middle East region of the Kingdom of Saudi Arabia the questionnaire was pilot tested among 12 dental hygienists (8 females and 4 males) to obtain feedback about clarity and objectivity.
Demographic data were collected from all respondents including gender, age, working sector (either public or private), level of education (either 2-year diploma or 4-year bachelor degree), and the number of working hours per week.
The survey questionnaire consisted of 102 items that were designed to induce either dichotomous or Likert-scale answers. Many sections were formulated in the survey to meet the objectives of the study, which comprised participants’ demographics, scientific backgrounds, level of confidence, practice behavior, and finally opinions about previous training and collaboration with other specialties.
Data analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) software version 22.0 (IBM Corp., Armonk, NY, USA). A Chi-squared test was used to check the association among the variables. Ordinal logistic regression analysis was performed to examine the role of gender, age, educational level, number of working hours per week, and working sector of the study participants as possible predictors for the subjects’ responses. A p-value<0.05 was considered significant.
Results
One hundred and sixty subjects agreed to participate in the study out of 192 subjects that were initially interviewed (response rate 83%); 124 females (77.5%) and 36 males (22.5%). The mean age of the study participants was 32.8±7.1 years ranging between 21-59 years. The mean age of male subjects was 34.2±8.9 years; for females it was 32.4±6.5 years. The level of education (diploma or bachelor), nature of the working sector (public or private), in addition to the number of working hours per week of the study participants are shown in Table 1.
Demographic and employment characteristics of dental hygienists.
Table 2 lists the percentage of participants identifying 14 factors as risk factors for periodontitis, cardiovascular diseases (CVDs), diabetes mellitus (DM), pregnancy complications, and osteoporosis. A high percentage of the participants identified oral bacteria (93.6%) as a risk factor for periodontitis followed by systemic inflammation (68.1%). For CVDs, 95% of the participants identified high blood pressure as a risk factor followed by more than 86% for smoking and high cholesterol level. While 83.8% of participants cited diet as a risk factor for DM, only 68.7% stated physical inactivity as a risk. For pregnancy complications, just 63.8% of the participating subjects stated alcohol use was a risk factor followed by genetics (53.8%). However, a smaller percentage of the respondents identified the risk factors for osteoporosis accurately ranging from less than 5% for high cholesterol level to 46.9% for menopausal. Multiple regression analysis revealed that the level of education was significant in the relationship in 13 items (Table 3). In addition, gender was found to be significant predictors in 2 items; the working sector was a significant predictor in just one item (Table 3).
Participants’ responses about the risk factors of five different common conditions.
The relationship between risk factors/diseases and significant determinants.
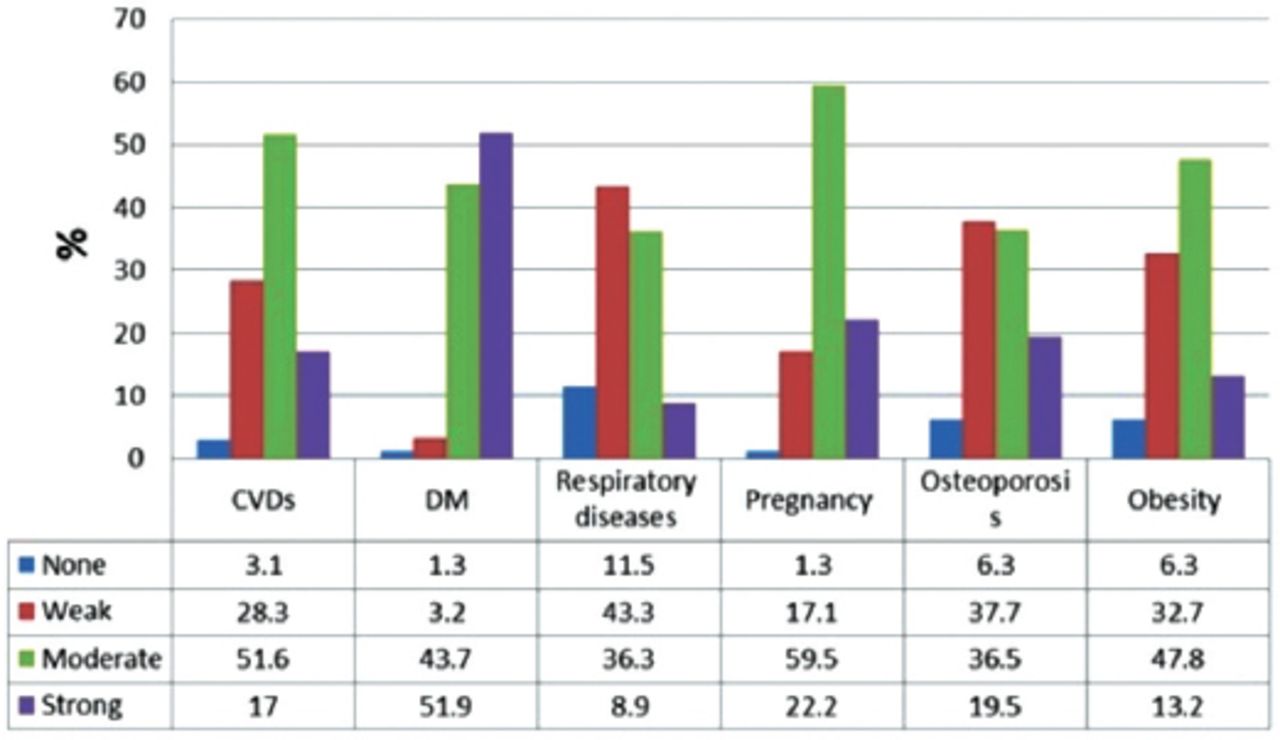
The participants’ opinions about the strength of evidence linking periodontal diseases to 6 different systemic conditions are illustrated in Figure 1. More than half of the respondents (51.9%) rated the evidence linking DM and periodontal disease as strong. About a fifth of the study participants stated that the link between pregnancy and osteoporosis with periodontal disease is strong. At the same time, 17% reported that the evidence strongly linked periodontal disease with CVDs, followed by 13.2% for obesity. Finally, fewer than 10% of the respondents stated that there was strong evidence linking periodontal disease with respiratory diseases.

The respondents’ knowledge about the strength of evidence connecting periodontal disease with different systemic conditions by percentage of respondents to each item. CVD - cardiovascular diseases, DM - diabetes mellitus
The dental hygienists’ confidence and comfort level while managing patients with systemic conditions are shown in Table 4. The respondents were slightly more comfortable asking patients about their smoking habits than their alcohol habits. In addition, participants were more comfortable treating periodontal patients who have diabetes (82.7%) compared with periodontal patients with CVDs (73.7%). Furthermore, they were less comfortable treating pregnant women with a higher risk of pregnancy complications or referring smokers to a smoking cessation clinic. More than 80% of the respondents felt confident discussing smoking cessation or the negative consequences of alcohol on the general health with their patients. Similarly, dental hygienists were consistently confident discussing the potential oral-systemic complications with patients who had periodontal disease, CVD, or diabetes or who were pregnant (range 75-80%).
The comfort and confidence levels among the study participants regarding several areas of oral-systemic health.
Table 5 shows the agreement level among the participants with statements regarding the inclusion of oral-systemic evidence in clinical practice. About three-quarters of participants either agreed or completely agreed that they thoroughly assess the patient’s risk for systemic disease. Similarly, more than 73% of the participants agreed/completely agreed that they ask very detailed follow-up questions on the medical history form. More than 84% of the respondents agreed that they adjust the frequency of dental visits for patients with systemic conditions. A comparable proportion (84.1%) stated that their knowledge about periodontal disease is current; consequently, 82.8% stated that they are interested in expanding their practice to include the management of patients with complicated medical conditions. Most participants (87.7%) either completely agreed or agreed that they provide thorough periodontal therapies to their patients. More than 82% of these dental hygienists agreed that their employers encourage staff members to incorporate evidence about oral-systemic disease into clinical practice.
Participants’ level of agreement with statements regarding the inclusion of oral-systemic evidence in clinical practice.
The respondents’ opinions about the professional training of dental hygienists, collaboration with other professions in the medical field, and patients’ expectations are shown in Table 6. More than 80% agreed that dental hygienists must be trained efficiently to identify possible risk factors for oral-systemic diseases. Similarly, 87.2% of the participants agreed that both medical and dental professionals must be trained to practice in a more collaborative way. Regarding the collaboration between the dental and medical professions, most of the responding dental hygienists stated that medical providers must be trained to screen patients with periodontal diseases (84.6%); more than 86% of the respondents agreed that medical providers have knowledge regarding the oral-systemic relations. Of these dental hygienists, approximately 84% stated that they were interested in collaborating more with physicians and nurses to improve patients’ inter-professional care. Regarding patient expectations, approximately three-quarters of the participants reported that patients appreciate being asked more than 76% of the respondents reported that patients wanted them to take a more “active role” in the management of systemic conditions. Similarly, 76.4% of our study participants perceived that patients were asking more questions about oral-systemic relationships.
Participants’ level of agreement with statements regarding training, collaboration with other specialties, and patient expectations in clinical practice.
The role of gender, age, educational level, number of working hours per week, and working sector of the study participants were assessed by ordinal logistic regression as significant predictors for participants’ responses. However, none of these factors were a significant predictor.
Discussion
Participants were asked about the risk factors associated with 5 common conditions to assess their knowledge about systemic diseases. While most factors were strongly documented as risk factors for the listed conditions, the knowledge level among our participants was low.
Contrary to previous studies that documented a strong relationship between smoking and periodontitis (the odds ratio for developing periodontitis among smokers ranged between 2.5-7.28 fewer than the half of our respondents identified smoking as a risk factor for periodontitis).17-19 Similarly, obesity is the most common risk factor for pregnancy complications, but fewer than 25% of our participants accurately responded to this item.20,21
The level of awareness among the study participants was extremely low compared with other studies. A study of dental hygienists in North Carolina, United States of America, in 2012 revealed that more than 90% of the participants identified DM, smoking, and genetics as risk factors for periodontitis. In contrary, less than 60% of our participants stated that DM is a risk factor for periodontitis, followed by less than 50% for smoking and about 30% for genetics for our study subjects.14
At the same time, our findings revealed that respondents were less knowledgeable about the risk factors of osteoporosis and adverse pregnancy complications compared with other conditions. This is consistent with a study by Bell et al,14 that revealed similar findings.
Multivariate analysis revealed that the level of education has a significant impact on the participants’ responses regarding specific items. In fact, bachelor degree holder’s responded correctly to some items compared to diploma holders. This could be because of differences in their knowledge. Likewise, gender was a significant predictor when the respondents identified race as a risk factor for osteoporosis. This could be imputed to a higher knowledge level among the females compared to males in issues related to menopause. However, no significant difference between males and females was found regarding pregnancy. This may be attributed to the fact that pregnancy is a more common state, and both genders have attained same level of knowledge.
On the other hand, periodontal disease is considered the second most common disease affecting the oral cavity next to dental caries.22-24 Therefore, managing and treating patients with periodontal disease is a routine procedure in dental practice.25 In addition, periodontal disease has been identified as the body’s most abundant source of chronic low-grade inflammation.26 This causes a decrease in the body’s immune response, contributes to the total inflammatory burden of the body, and eventually causes irreversible damage to the immune system.26 Hence, all dental staff should be knowledgeable about factors related to periodontal disease such as etiology, underlying pathological process, associated risk factors, and related negative impact on other tissues.
Our findings revealed that approximately 85% of the respondents stated that their knowledge about periodontal-systemic interactions is current; similarly, most expressed that they provide comprehensive periodontal therapies to their patients. However, the knowledge-related items in our survey revealed that the level of awareness among them regarding the risk factors of periodontal disease was low in general. While approximately three-quarters of dentists and dental hygienists in previous studies stated that the link between periodontal disease and CVDs was strong and less than a fifth of our participants agreed with that. This study revealed a lack of knowledge among participants about the strength of evidence connecting periodontal disease with respiratory diseases, osteoporosis, and obesity. This agrees with the findings of other studies.14,16
More than three-quarters of our participants stated that they asked their patients thorough questions about their systemic health; in addition, more than 80% adjust the appointments of medically compromised patients to avoid possible complications. Therefore, despite the lack of knowledge among our study respondents, the respondents were aware of several precautions that must be considered while managing medically compromised patients.
Nevertheless, our findings revealed that most respondents were confident and comfortable managing medically compromised patients. Perhaps as a result of apprehension from serious medical complications or legal liability, the comfort level of respondents decreased from more than 80% when asked about DM to approximately 66% for pregnancy complications. Bell et al,15 identified the barriers of incorporating oral-systemic evidence into dental practice. The main barriers were lack of time (52%), legal risks (44%), and lack of education (27%).
Our findings suggest that more education regarding systemic diseases is required for dental hygienists. This is similar to the recommendations of other studies.14,27 Interestingly, more than 82% of our study participants had a readiness to expand their practice to include management of medically compromised patients, which is considerably higher than the findings of other surveys.14,16 Furthermore, most of our respondents were aware of the importance of incorporating oral-systemic evidence into a daily dental practice; in addition, a high percentage of the participants agreed that dental and medical professionals should work in collaboration while managing medically compromised patients. This finding is consistent with the results of other studies.14,16,28
However, evidence suggests that inter-professional education directly reflects optimized healthcare services, strengthening medical systems, and improving health outcomes.29 Moreover, the Commission on Dental Accreditation in the United States of America requires preparation of dental hygiene graduates for inter-professional collaboration.30 Similarly, an editors’ consensus report of the American Journal of Cardiology and Journal of Periodontology in 2009 stated that ‘on the basis of current data, untreated or inadequately controlled moderate to severe periodontitis increases the systemic inflammatory burden, periodontitis may independently increase the risk of CVD’s.31 Consequently, the consensus report endorsed that both dental and medical professionals should closely collaborate to optimize cardiovascular risk reduction and periodontal care. A recent study in 2017 revealed that inter-professional continuing education program among dental and non-dental health care professionals improved the oral-systemic health practice immediately.32
These findings are promising and suggest that the level of knowledge among the dental hygienists could be raised easily by training and education. Further training could be achieved in 3 ways: by revising college curriculums and incorporating topics about oral-systemic relations, by establishing specialized continuing education programs that focus on the oral-systemic evidence, and by enhancing the inter-professional collaboration between the health professionals to enable an interdisciplinary sharing of expertise, perspectives, and resources.
Study limitations
The study enrolled many dental hygienists practicing in Kingdom of Saudi Arabia and especially Riyadh, which is inconclusive. Another limitation is related to generalizability, the distribution of the survey was limited to Riyadh, which is the capital and the first most populous city in Kingdom of Saudi Arabia. Thus, it is difficult to generalize our findings to all dental hygienists in Kingdom of Saudi Arabia. Another study limitation was the survey did not ask about the barriers that deterred respondents from incorporating oral-systemic evidence into their practice.
In conclusion, Dental hygienists in Riyadh, Kingdom of Saudi Arabia demonstrated low level of knowledge and awareness regarding the oral-systemic evidence. Dental hygienists were confident and showed a desire to be engaged in the management of medically compromised patients. They appreciated the collaboration with medical professionals. However, comprehensive educational programs regarding the oral-systemic evidence must be established to promote the role of dental hygienists in the community.
Acknowledgment
The authors would like to thank Mr. Joseph Raheb, Sessional academic, Oral Health Therapy, School of Pharmacy and Biomedical Sciences, Faculty of Health Sciences, Curtin University, for his valuable remarks and feedback on the manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 15, 2018.
- Accepted September 26, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.