


Abstract
Objectives: To evaluate the presence of Coxiella burnetii (C. brunetii) infection among patients presenting with fever of unknown origin (FUO).
Methods: A cross-sectional study of 100 patients (54 men and 46 women; mean age: 34.3 ± 19.2 years) with FUO was conducted at King Khalid University Hospital, Riyadh, Saudi Arabia between March 2015 and June 2016. Phase 1 and phase 2 C. burnetii-specific antibodies in serum samples were detected by enzyme-linked immunosorbent assay.
Results: Coxiella burnetii phase 1 and phase 2 antibodies were detected in 16% of the patients. Phase 2 IgM was present in 2% of the patients, whereas phase 2 IgG antibodies were detected in 11% of the patients. Coxiella burnetii-specific phase 1 IgG was found in 2% of the patients, and 8% of the patients harbored phase 1 IgA antibodies in their serum.
Conclusion: The presence of C. burnetii-specific antibodies in many patients suffering from FUO highlights the importance of Q fever screening among patients presenting with febrile illness.
Q fever is a zoonotic disease caused by Coxiella burnetii and is found worldwide. This disease may present as an acute or chronic febrile illness and has the potential to cause outbreaks.1,2 Coxiella burnetii is a pleomorphic, obligate intracellular coccobacilli with a gram-negative cell wall. This spore-forming organism is able to survive for long periods in food products and under hostile environmental conditions. Notably, C. burnetii undergoes well-defined phase variation.3
Lipopolysaccharide (LPS) is a major virulence determinant of C. burnetii.4 Following isolation from animals or humans, C. burnetii expresses phase I antigens and is highly infectious (a single bacterium may infect a human). Phase I LPS, with its extended carbohydrate structure, sterically blocks access of an antibody to surface proteins thus allowing bacterial persistence after acute infection.4 Sub-culturing of C. burnetii has been shown to induce antigenic shift in LPS to phase II which is a relatively less infectious form and is accessible to antibodies.4,5 Lipopolysaccharide seems to be the only antigenic difference between phase I and II6 and is extremely valuable for the serological differentiation between acute and chronic Q fever.
Coxiella burnetii is found in arthropods, rodents, and other animals.7 This disease has been documented in Saudi Arabia and other Arabian Gulf and Middle Eastern countries (UAE and Oman) in humans and animals;8-14 however, data are scarce. Infected domestic animals such as goats, cattle, sheep, cats, and dogs3 shed desiccation-resistant organisms in urine, feces, milk, and other products for human consumption. Recent reports have indicated that the prevalence of C. burnetii among domestic livestock in Saudi Arabia is approximately 30%, indicating that Q fever is a potential threat to the local population.15
Coxiella burnetii can be transmitted to humans by direct contact or by airborne, vector-borne, and common vehicle routes. Q fever is mostly asymptomatic; however, patients occasionally become ill with severe retrobulbar headache, fever, chills, fatigue, and myalgia. Patient with Q fever can present acutely with pneumonia, hepatitis, or chronically with endocarditis. Acute Q fever is traditionally treated with either tetracycline or doxycycline for over a period of 2 weeks.16
Q fever is usually diagnosed by serological tests, including microagglutination, complement fixation, radioimmunoassay, indirect immunofluorescence assay (IFA), indirect hemolysis test, enzyme-linked immunosorbent assay (ELISA), enzyme-linked immunosorbent fluorescence assay, dot immunoblotting, and western immunoblotting.17 However, additional, more accurate methods are needed to identify C. burnetii in different phases.
In this study, we aimed to screen serum samples from patients presenting with fever to determine the presence of phase 1 and phase 2 C. burnetii-specific antibodies.
Methods
This cross-sectional study was conducted at King Khalid University Hospital (KKUH), Riyadh, Saudi Arabia between March 2015 and June 2016. In total, 100 patients were enrolled in this study, including 54 men and 46 women (mean age: 34.3 ± 19.2 years). The inclusion criteria were as follows: patients presenting with fever of unknown origin (FUO) with negative test results for blood culture, antibody detection for brucellosis, typhoid fever, and serological tests for other bacterial and viral infections. A single blood specimen was collected from patients for screening because the symptom duration among all patients was over one month. Clinical details of the patients were not available due to lack of access to patient records. All patients were tested for phase 1 IgA and IgG and for phase 2 IgM and IgG C. burnetii antibodies. The study was performed according to the ethical standards of the Declaration of Helsinki. The study was approved by the Institutional Review Board of the College of Medicine, King Saud University, Saudi Arabia.
Detection of Coxiella burnetii antibodies
Coxiella burnetii-specific antibodies were detected by ELISA using commercial kits (SERION, Germany) in accordance with the manufacturers’ instructions. For detection of phase 1 IgA and IgG, 10 µL serum was diluted with 1000 µL sample diluent. For detection of phase 2 IgG C. burnetii-specific IgG antibodies, 10 µL patient serum was diluted in 1000 µL sample diluent, and an aliquot of 50 µL was further diluted in 200 µL of the same buffer for detection of phase 2 IgG. For detection of phase 2 IgM, 10 µL patient serum was treated with 1000 µL of 1:4 diluted rheumatoid factor absorption solution. Following sample preparation, all tests were performed under similar conditions. Briefly, 100 µL of diluted samples or controls was dispensed in a 96-well plate precoated with C. burnetii antigens. The plate was then incubated for 30 min at 37°C to allow formation of antigen-antibody complexes. The plate was washed 4 times, and alkaline phosphatase conjugate was added and incubated for an additional 30 min at 37°C. Thereafter, a washing step was performed, and 100 µL substrate solution (para-nitrophenylphosphate) was added. Finally, the reaction was stopped using 100 µL stop solution (<0.1 N sodium hydroxide, 40 mM ethylenediaminetetraacetic acid), and the colorimetric signal was determined by measuring the absorbance at 405 nm using a spectrophotometer. Since repeat sampling was not possible, any sample yielding a borderline result was tested for a second time and was reported as negative if the result remained the same.
Results
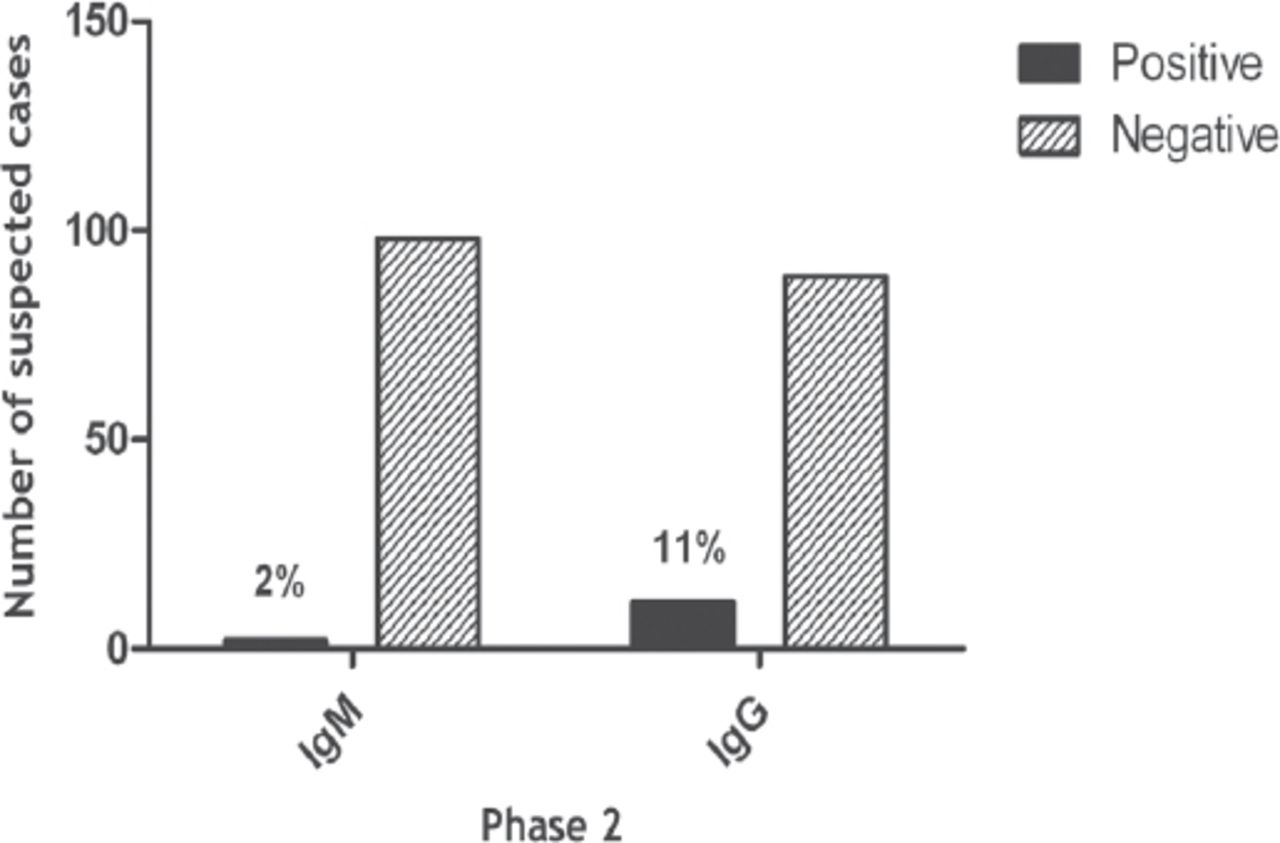
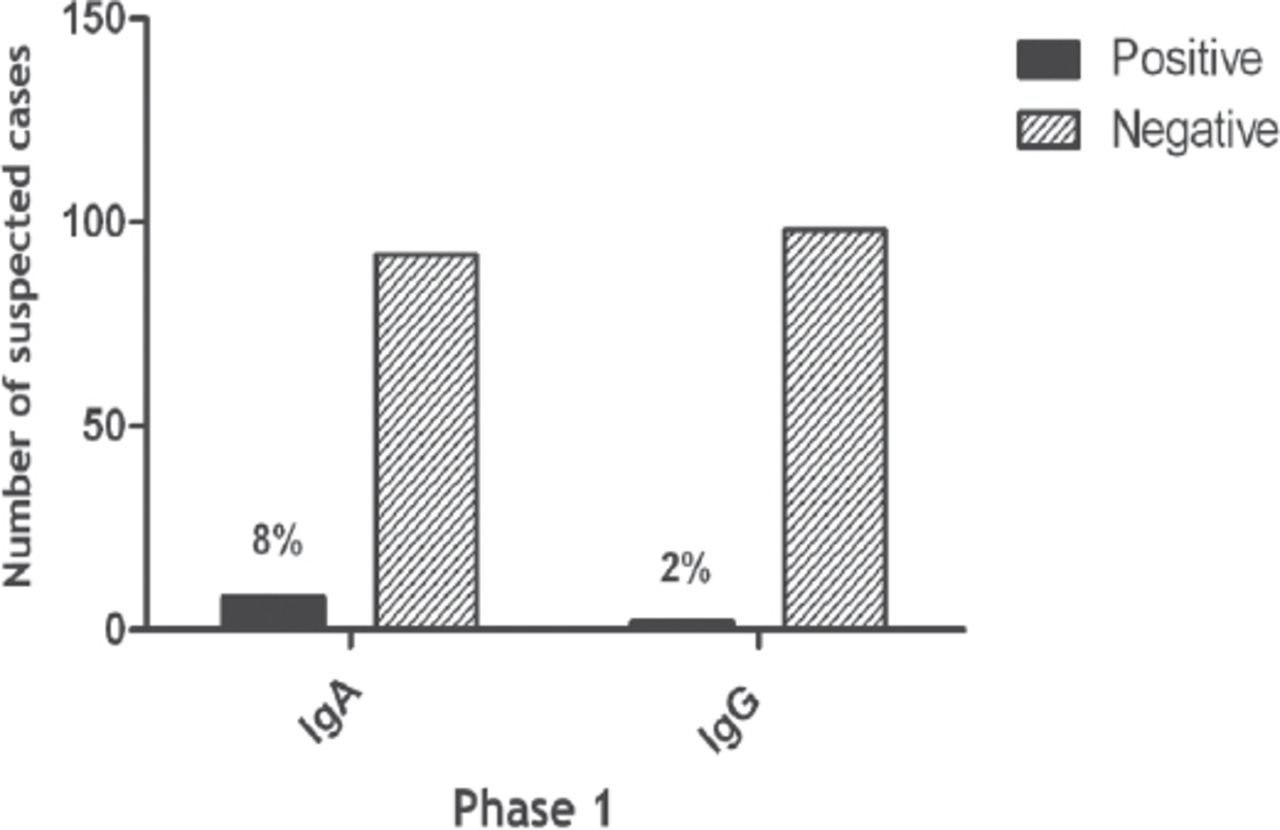
Among the 100 patients suffering from FUO screened for C. burnetii-specific antibodies, 16 (16%) patients (8 men and 8 women) were found to harbor phase 1 and phase 2 antibodies (Table 1). Figure 1 shows data for C. burnetii-specific phase 2 IgG and IgM antibodies of the 100 patients tested, only 2 tested positively for phase 2 IgM, and 11 patients had phase 2 IgG C. burnetii antibodies in serum samples. Phase 1 testing for C. burnetii-specific antibodies revealed that phase 1 IgG antibodies were present only in 2 patients, whereas 8 patients had phase 1 IgA C. burnetii-specific antibodies in serum samples (Figure 2). Phase 2 IgG and phase 1 IgA antibodies were detected together in 5 patients, whereas phase 2 IgG, phase 1 IgA, and phase 1 IgG were detected together in only 2 patients (Table 1).
Fever of unknown origin cases.
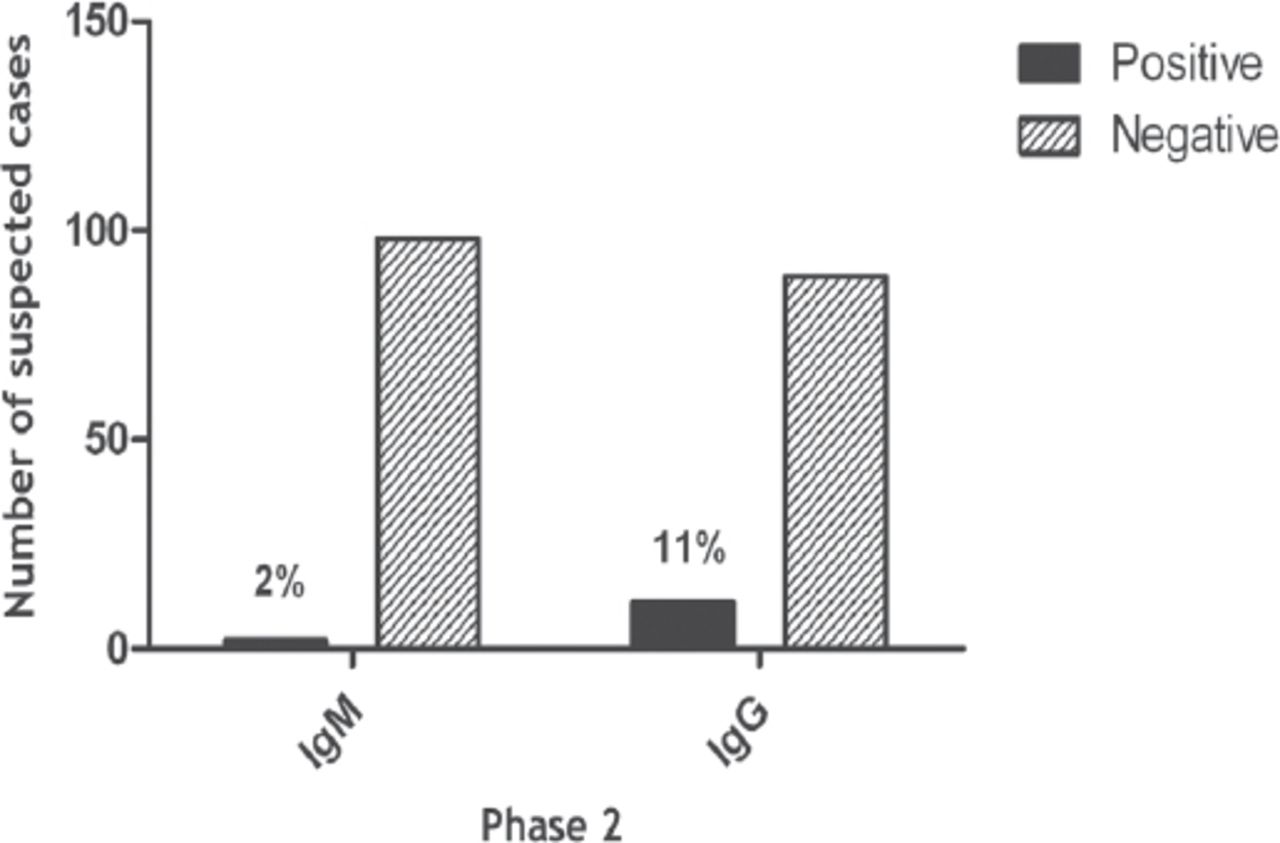
Coxiella burnetii-specific phase 2 IgG and IgM antibodies.
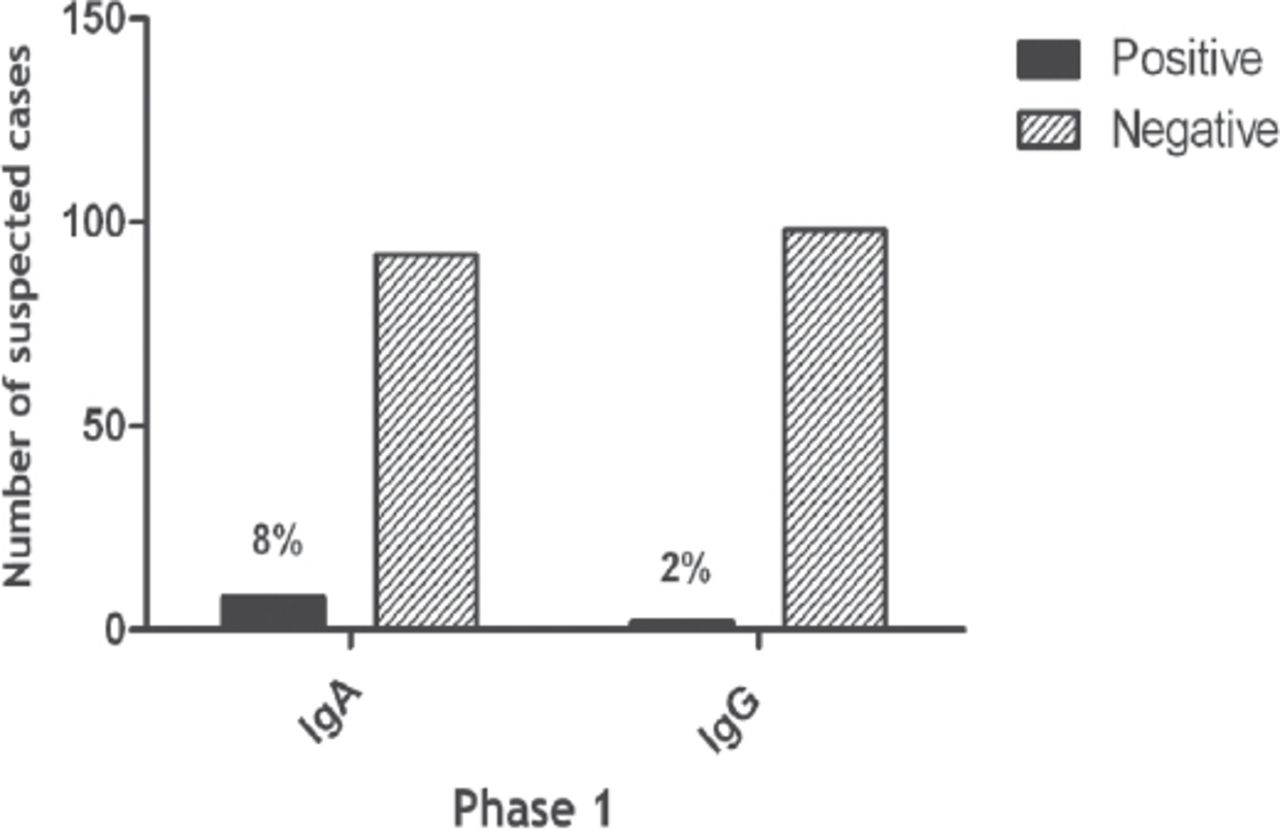
Coxiella burnetii-specific phase 1 IgG and IgM antibodies.
Discussion
Based on the detection of phase 1 and phase 2 C. burnetii-specific antibodies, 16% of patients harbored evidence of C. burnetii infection in the present study. In the northeastern region of Spain, the seroprevalence of C. burnetii in humans was reported to be 15.3%.18 In contrast, in this study, the study population comprised patients with FUO, and the actual seroprevalence in the local population appears to be lower than 16%. A seroprevalence of 4.8% was reported among 459 unexposed women from Denmark.19 Moreover, in Western Kenya, the prevalence rate has been reported to be as low as 2.5%.20 Seven years after an outbreak of Q fever in the Netherlands, the seroprevalence of Q fever remains high, at 33.8%.21 Collectively, these observations indicated regional variations in the prevalence of Q fever that may be due to differences in the prevalence rates among animals, as well as differences in human exposure, previous outbreaks of Q fever in the community, selection of the study population, and the methods used for detection of C. burnetii infection.
Coxiella burnetii-specific antibodies in the serum of patients suffering from FUO were detected by ELISA in the present study. Using IFAs, a prevalence of 35.2% has previously been reported from the Kingdom of Saudi Arabia in a similar study population.22 The prevalence of Q fever observed in the present study (16%) was almost half that reported previously in the Kingdom of Saudi Arabia. Although IFAs have been shown to detect higher percentage of C. burnetii-specific phase 1 and phase 2 antibodies compared with ELISA,23 there is evidence refuting these claims.24 Two consecutive studies, including the present study, have clearly demonstrated the presence of serological evidence of C. burnetii in the local human population. These observations have emphasized the need for large-scale epidemiological studies using more than one testing modality among the local human and animal populations to assess the prevalence of C. burnetii in Saudi Arabia.
Both phase 2 and phase 1 C. burnetii-specific antibodies were detected in the present study. At least 13% of patients with Q fever are believed to evade diagnosis either due to no attempt to screen the patients for the presence of C. burnetii specific antibodies or screening for C. burnetii in the early stages of infection before the appearance of detectable titers of C. burnetii specific antibodies. Phase 2 IgM appear within first 2 weeks after the onset of symptoms, reaching a maximum concentration by 4-8 weeks and remain detectable for a relatively short period.25 Phase 2 IgG antibodies appear later as the disease progresses and tend to persist for years or even for life.26 These observations suggest that among the local population, all patients suffering from FUO should be offered C. burnetii screening to avoid Q fever-associated morbidity and mortality.
Phase 1 C. burnetii IgA antibodies were detected in 8% of the study population in the present study. These antibodies have been shown to exhibit a strong correlation with Q fever in general, particularly with endocarditis.27,28 For the same reason, the presence of IgA phase 1 antibodies has been considered as a diagnostic marker of chronic Q fever.27 However, there is evidence demonstrating that phase 1 C. burnetii antibodies may contribute little to the diagnosis of Q fever28 but can serve as a useful marker for the follow-up of treated patients.29 The absence of a 4-fold decrease in phase 1 IgG and IgA antibodies and the presence of phase 2 IgM antibodies at the end of 1 year are among the determinants associated with mortality in Q fever.30
Despite the important findings of our study, the results should be interpreted based on the limitation that few cases were repeatedly within the gray zone for a single antibody marker, hindering interpretation of the findings; these patients could not be reached to collect additional samples. Thus, further studies with more patients are needed to confirm these findings.
In conclusion, phase 1 and phase 2 C. burnetii antibodies were detected in a relatively large proportion of patients with FUO. Evidence continues to emerge documenting the presence of Q fever in livestock and humans in the Kingdom of Saudi Arabia. These observations indicate the necessity for national investigations to determine the exact prevalence of Q fever among humans and animals in Saudi Arabia and to introduce Q fever screening for suspected cases on a regular basis.
Acknowledgment
The authors would like to thank the Faculty of Medicine, King Khalid University Hospital; and the Deanship of Scientific Research and Researchers Support & Services Unit, King Saud University, Riyadh, KSA for their technical support.
Footnotes
Disclosure. This study was approved by the Institutional Review Board of the College of Medicine, King Saud University, Riyadh, Saudi Arabia (Project no. E14-1135).
- Received August 21, 2018.
- Accepted October 21, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.