


Abstract
Objectives: To quantitatively evaluate palatal bone thickness in adults with different facial types using cone beam computed tomography (CBCT).
Methods: The CBCT volumetric data of 123 adults (mean age, 26.8 years) collected between August 2014 and August 2016 was retrospectively studied. The subjects were divided into a low-angle group (39 subjects), a normal-angle group (48 subjects) and a high-angle group (36 subjects) based on facial types assigned by cephalometric radiography. The thickness of the palatal bone was assessed at designated points. A repeated-measure analysis of variance (rm-ANOVA) test was used to test the relationship between facial types and palatal bone thickness.
Results: Compared to the low-angle group, the high-angle group had significantly thinner palatal bones (p<0.05), except for the anterior-midline, anterior-medial and middle-midline areas.
Conclusion: The safest zone for the placement of microimplants is the anterior part of the paramedian palate. Clinicians should pay special attention to the probability of thinner bone plates and the risk of perforation in high-angle patients.
Miniscrews have been widely used in orthodontic clinics. Their application has increased the viability of skeletal anchorage due to their ability to be positioned in many areas including the buccal alveolus and the hard palate.1,2 However, the interradicular spaces are limited by the proximity of neighboring roots or of the periodontium, resulting in failure. These risk factors can be avoided by the use of “rootless areas” such as the hard palate.3 The palate is a suitable location for the implantation of miniscrews due to its richly keratinized mucosa, low risk of potential root or blood vessel injury and ease of access.4-6 The palate consists of cortical bone, which is sufficiently thick and dense to support a miniscrew and to sustain orthodontic loads. Many orthodontists have used palatal miniscrews to move the entire frontal group back and for molar distalization without loss of anchorage.7-9 The thickness of the palate bone is crucial to the suitability of selected implantation sites. Sufficient bone depth would prevent inserted implants from perforating the nasal floor or the maxillary sinus. The morphology of the maxillomandibular complex may be related to the surrounding muscular system, which can affect vertical face patterns.10 Ozdemir et al11 reported that, in high-angle patients, all miniscrew insertion sites on both jaws have significantly lower values than in low-angle patients. Palatal bone thicknesses will also differ in patients with different facial patterns.
Three-dimensional measurements and analyses of parameters of the maxillomandibular complex such as the morphology and cortical bone thickness of the mandible have become popular recently.10,12 Studies have demonstrated that cone beam computed tomography (CBCT) can provide noninvasive tridimensional (3D) images of oral structures. Cone beam computed tomography can reflect the structure of palatal bones. Evaluation of palatal bone depth with CBCT is easy and accurate. Previous studies have investigated palatal bone thickness with CBCT.13,14 However, in these studies, subjects with different facial types were not studied. Few comprehensive studies have investigated how palatal bone thickness, as related to mini-implant insertion sites, is affected by different vertical patterns. The objective of the present study was to investigate total palatal bone depth for the placement of orthodontic miniscrews in adults with different facial types.
Methods
All participating individuals provided written informed consent before CBCT scanning, and this study was approved by the Ethical Committee of the Chongqing Medical University, Chongqing, China, which complies with the Declaration of Helsinki. The inclusion criteria were patients with malocclusion who were between 18 and 40 years old. Subjects were excluded if they had a history of orthodontics; facial asymmetry; severe skeletal abnormalities, anomalies, or asymmetric occlusions; impacted teeth or any systemic illnesses. After all inclusive and exclusive criteria were applied, 123 adults (57 men, 66 women) aged 18 to 35 years (mean age, 26.8 years) were selected.
The subjects were divided into 3 groups according to vertical facial types, which were assessed by one senior orthodontist on the basis of the sella turcica (S)-gonion (Go)/nasion (N)-menton (Me) ratio, Frankfort Horizontal (FH)/Go-Me and the S-N/Go-Me angle as measured on lateral cephalograms (Figure 1). Subjects were defined as high- and low-angle if they had S-Go/N-Me ratios less than 61% or greater than 69%, respectively, and the remaining subjects were classified as normal-angle.15 Patients with FH/Go-Me angles less than 22°, between 22° and 32° and greater than 32° was classified as low-, normal- and high-angle, respectively. Patients with S-N/Go-Me angles less than 27°, between 27° and 37° and greater than 37° were classified as low-, normal- and high-angle, respectively.16 Subjects with measurements that were inconsistent or borderline were excluded. However, no subject was excluded during the assessment of facial types. The CBCT scans of 123 patients were analyzed. According to vertical facial types, Group A (the low-angle group) included 39 subjects (22 males, 17 females); group B (the normal-angle group) consisted of 48 subjects (26 males, 22 females); and group C (the high-angle group) comprised 36 subjects (17 males, 19 females).
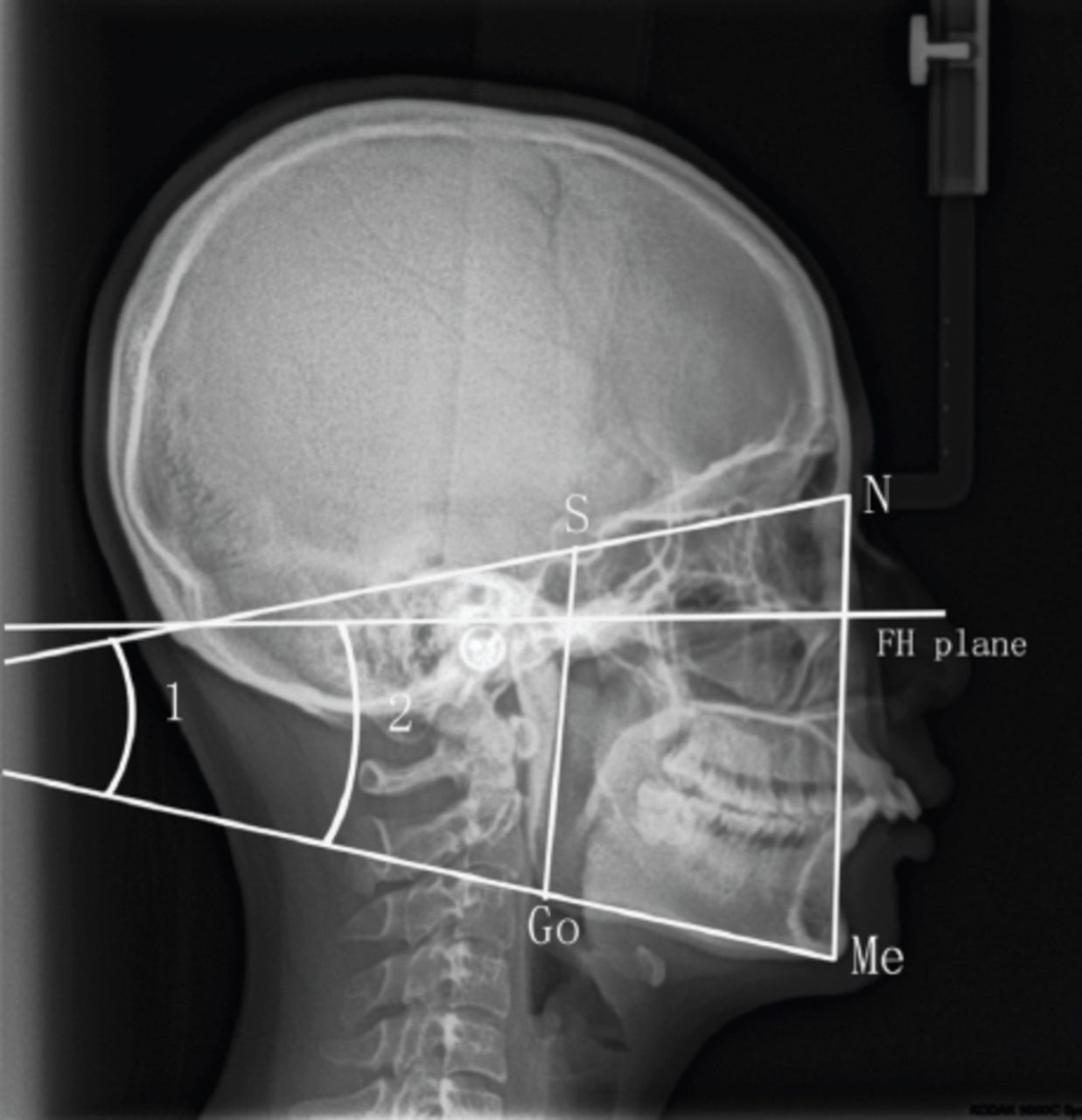
Cephalometric data showing skeletal variables. N - nasion; S - sella turcica, Me - menton, Go - gonion. ∠1 - S-N/Go-Me angle, ∠2 - FH/Go-Me angle. Vertical facial types were assessed on the basis of the S-Go/N-Me ratio, FH/Go-Me and the S-N/Go-Me angle. FH - Frankfort Horizontal
Data were obtained using a KaVo 3D eXam (KavoSybron, Orange, CA). The settings used were as follows: 120 kV, 50 mA, 13×10 cm field of view, exposure time 4 seconds. Digital volumetric tomograms were reconstructed with a 0.4 mm slice thickness in Invivo 5.0 software (Anatomage, San Jose, CA, USA).
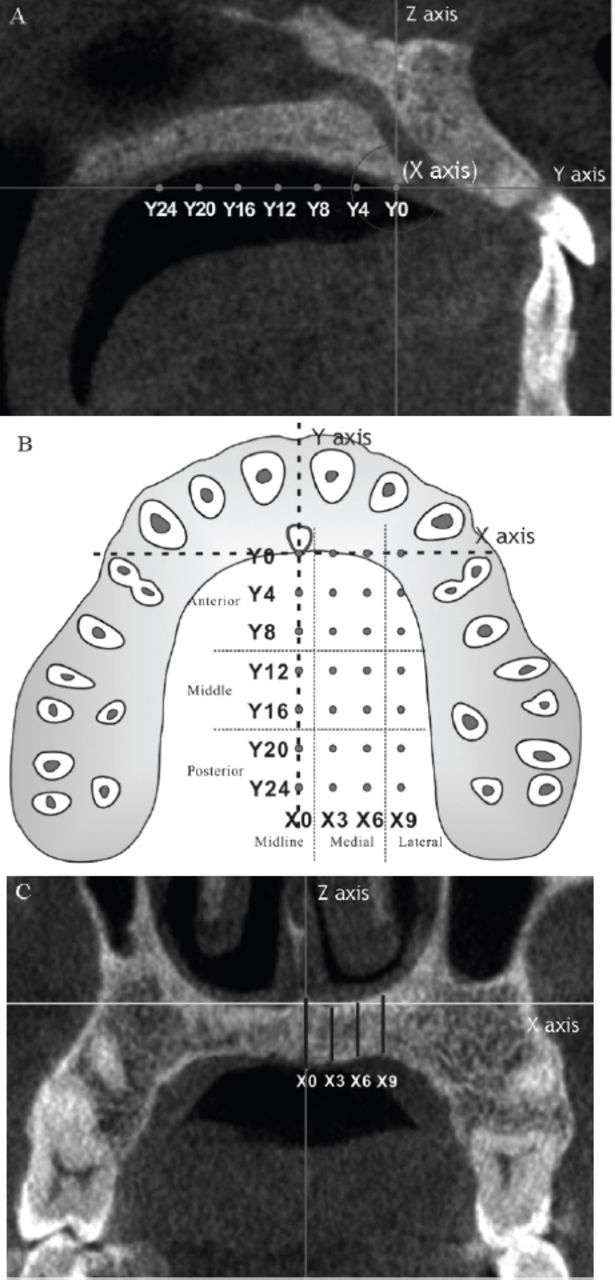
The line passing through the midpoint of the posterior border of the foramen incisivum and the posterior nasal spine (PNS) was defined as the midline (Figure 2A). Along the midline, the midsagittal plane was created by multiplanar reconstruction. The line perpendicular to the midsagittal plane was defined as the X-axis. The image was rotated around the X-axis to align the midline on a horizontal plane. On the horizontal plane, 28 measurement points were arranged in 4 rows at intervals of 3 mm mediolaterally; each row contained 7 measurement points with intervals of 4 mm anteroposteriorly17 (Figure 2B). In the coronal view, bone thickness was measured parallel to the Z-axis at each measurement point (Figure 2C). Measurements were taken twice by one operator. As previous studies have reported, no significant differences were found between the left and right sides of the palate; hence, only data obtained from the left side were analyzed further. Cone beam computed tomography scans from 20 subjects were selected randomly and re-assessed by the same person, 2 weeks after the initial survey. The intraclass correlation coefficient was used to test intraexaminer reliability.
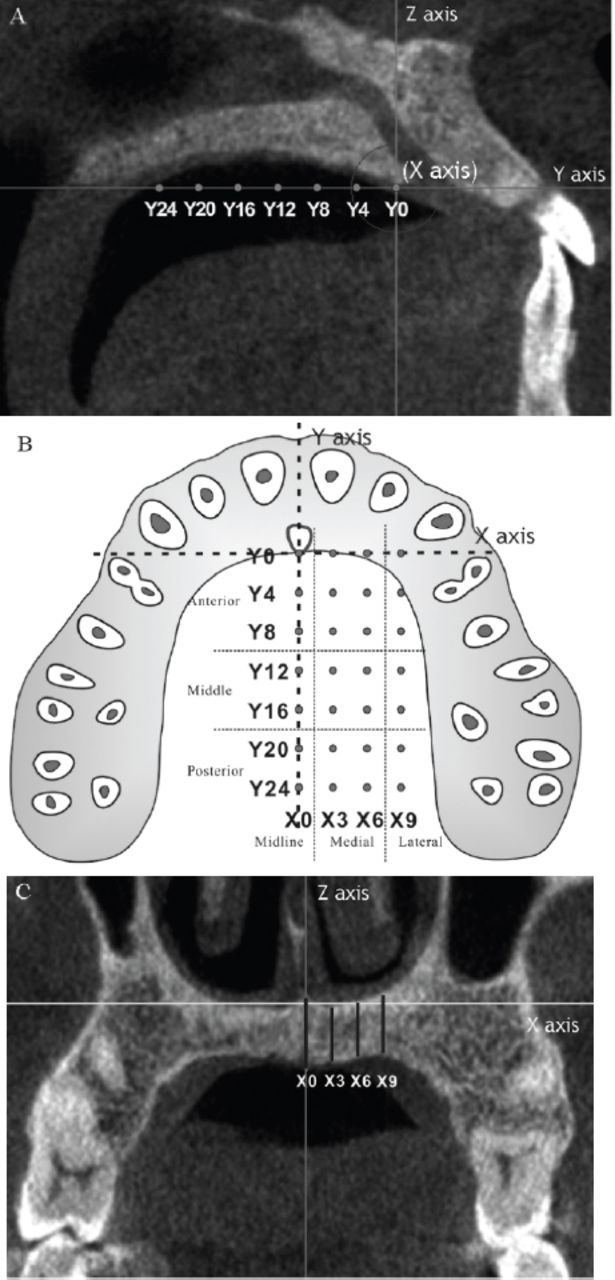
Measurements of total palatal bone depth. A) Sagittal view showing the designated points along the midline. The line passing through the midpoint of the posterior border of the foramen incisivum and the posterior nasal spine (PNS) was defined as Y axis and midline. On the sagittal view, The line passing through the midpoint of the posterior border of the foramen incisivum and perpendicular to the Y axis was defined as Z axis. The line passing through the midpoint of the posterior border of the foramen incisivum and perpendicular to the Y axis and Z axis was defined as X axis (not shown). The measurement points on the Y axis with intervals of 4 mm anteroposteriorly were numbered from Y0 to Y24. B) The sketch map of measurement points on the horizontal plane. For easier understanding, The plane passing through the X axis and Y axis was defined as the horizontal plane. 28 measurement points were arranged in 4 rows at intervals of 3 mm mediolaterally and 7 lines at intervals of 4 mm anteroposteriorly. The measurement points were divided mediolaterally and anteroposteriorly into 9 areas. C) Coronal view showing a the measurement of bone depth. The dark line passing through each measurement point indicates the bone depth.
Statistics analysis
Data analysis was performed using SPSS (Release 13.0, standard version; SPSS, Chicago, IL). The measured bone thickness values were divided mediolaterally and anteroposteriorly into 9 areas18 (Figure 3). Three designated mediolateral areas were defined: the midline area at the midline palatine suture, the medial area at the reference lines 3 and 6 mm lateral to the midline palatine suture and the lateral area at the line 9 mm lateral to the midline palatine suture. Similarly, three anteroposterior areas were defined: the anterior area at lines 0, 4 and 8 mm; the middle area at lines 12 and 16 mm; and the posterior area at 20 and 24 mm posterior to the distal margin of the foramen incisivum (Figure 3). The repeated-measure analysis of variance (rm-ANOVA) test was used to test for differences among measurements at designated areas, and Fisher’s LSD test was used for pairwise comparison. p<0.05 was considered statistically significant.

The bone thicknesses at different areas of the palate. The thickness of mediolateral areas were shown in different shapes. Thickness unit: millimeter (mm).
Results
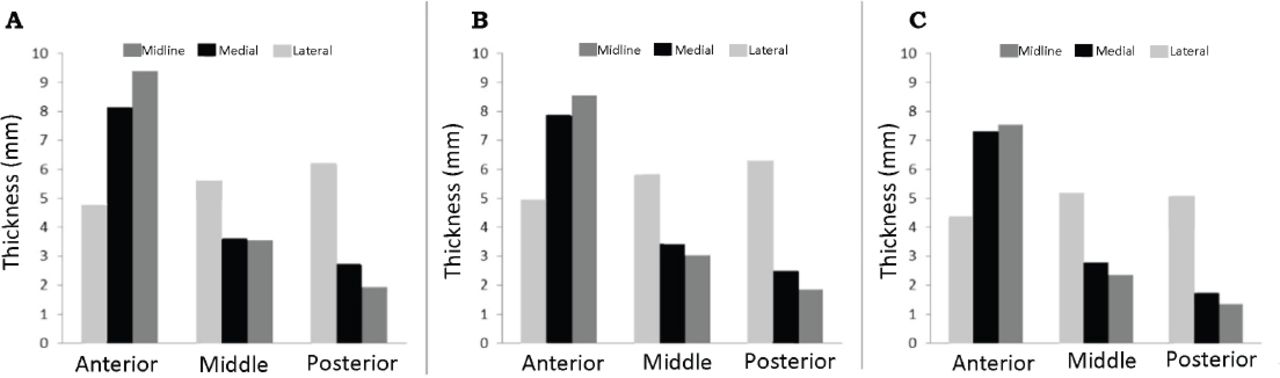
The intraclass correlation coefficient (ICC) between the 2 assessments showed high reliability (p>0.8). Significant differences in palatal bone thickness were found among the anterior, middle, and posterior areas.13 The anterior bone thickness was significantly lower than the posterior bone thickness in the midline area (p<0.05), but thickness decreased consistently in the posterior direction in the medial and lateral areas (p<0.05). Additionally, we found significant differences among bone thicknesses in the lateral, medial and midline areas (p<0.05). Bone thickness in the midline area decreased progressively in the lateral direction in the middle and posterior areas, except for the anterior area (Table 1, Figure 3). The association between bone thickness and facial types was statistically significant (p<0.05) in the same area of the palate except for the anterior-midline, anterior-medial and middle-midline areas. We found that bone in the low-angle and normal-angle groups was significantly thicker than in the high-angle group in the posterior areas (p<0.05). Further, the bone thicknesses in the low-angle group were significantly higher than in the high-angle group in the anterior-lateral, middle-medial and middle-lateral areas (p<0.05) (Table 2, Figure 4).
The thickness of palatal bone in different regions.
Comparison of the thickness of palatal bone in volunteers with different facial types.

The bone thicknesses of subjects with different facial types showing the A) low-angle, B) normal-angle, C) high-angle The thickness of mediolateral areas were shown in different grayscale. Thickness unit: millimeter (mm).
Discussion
Depending on mechanical requirements, either buccal or palatal sites of insertion can be useful. Interradicular sites may allow for the stable buccal insertion of skeletal anchorage in most cases. The paramedian palate (PP) is considered an alternative site for the insertion of miniscrews. Another advantage of palatal insertion is that miniscrews with wider diameters can be used, improving stability. Anatomy, particularly bone depth, may directly influence the safety of insertion.19 Thicker bone can support longer mini-implants, which provide greater primary stability,20,21 a factor related to the success of the implant.22 The anatomy of the PP must be determined, with special attention to mapping bone thickness and classifying potential sites for implanting miniscrews. Cone beam computed tomography can provide excellent measurements of bone thickness in the PP, allowing the 3D quantitative measurement of a region of interest (ROI). Surveys of bone thickness in designated planes of the PP have been reported in the literature.23,24 Using CBCT to examine an ROI provides a precise method for evaluating bone depth at these locations, and for detecting critical structures such as the canalis incisivus and maxillary sinus.
In this study, the thickest palatal bones were measured in the medial and lateral parts of the anterior area, except for the anterior midline area. In the midline area, the anterior bone thickness was found to be significantly lower compared with the posterior bone thickness. This might be due to the incisive canal, which extends in a posterior-superior direction in the anterior part of the midline area. As our study indicates, the anterior part of the paramedian palate provides sufficient bone volume for microimplants. Consistent with our study, Kang et al18 and Ryu et al25 reported reduced palatal bone thickness along the lateral and posterior directions in adults. In the middle-medial, middle-lateral, posterior-medial and posterior-lateral areas, the palatal bone thickness was lower compared with that in the midline and anterior areas. Clinicians inserting implants in these areas should either pay more attention to the risk of perforating the nasal cavity or choose shorter mini-implants. According to this study, bone thickness along the anterior midline is less than in the anterior medial region. This information is also valuable for the clinicians to take into account when inserting long miniscrews in the midpalatal suture in patients with all facial types.26
Poon et al27 found that palatal bone thickness is not associated with tongue position, the existence of a posterior crossbite, or palatal morphology. However, in females, the FMA angle is significantly inversely associated with palatal bone thickness, primarily in the middle to posterior region of the palate. In the present study, we found that palatal bone thickness was significantly related to facial type. The palatal bone depth in high-angle facial type group was significantly thinner than in the low-angle group. These results are in agreement with those of previous studies that evaluated other parameters of different facial types.11,28-30 Fulya et al11 found that the cortical bone thickness of both the maxilla and mandible is significantly related to facial type. Low-angle subjects had significantly higher cortical bone thicknesses than high-angle subjects. Similarly, Li et al29 found correlations between facial types and cortical bone thickness in their studies on 3-dimensional images of 101 Asian participants. In the mandibular molar region, cortical bone thicknesses in the low-angle group were significantly thicker than those in the high-angle group. In a clinical study by Moon et al,31 success rates and influencing factors of 778 mini-implants were evaluated, and subjects with a high Frankfort-mandibular plane angle and a low-angle facial type were found to have significantly lower odds ratios than those with other facial types. Facial types cause differences in cortical bone thickness, thereby affecting the success of diverse microimplants. Our study found that, for all facial types, the safest zone in the palate for the placement of microimplants was the anterior part of the paramedian palate. However, clinicians should pay special attention to the probability of thinner bone plates and the risk of perforation in high-angle patients.
The success of mini-implant insertion is influenced by many factors. The minimum bone thickness necessary for microimplant insertion remains controversial, particularly when stability and the protection of other anatomic structures are taken into consideration. Further research regarding palatal bone density, palatal shape and arch form type could provide more information for clinicians.
In conclusion, the anterior part of the paramedian palate provides sufficient bone volume for the insertion of microimplants. For all facial types, the safest zone in the palate for the placement of microimplants is the anterior part of the paramedian palate. Clinicians should pay special attention to the probability of thinner bone plates and the risk of perforation in high-angle patients.
Authorship entitlement
Excerpts from the Uniform Requirements for Manuscripts Submitted to Biomedical Journals updated November 2003.
Available from www.icmje.org
The international Committee of Medical Journal Editors has recommended the following criteria for authorship; these criteria are still appropriate for those journals that distinguish authors from other contributors.
Authorship credit should be based on 1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) intellectual content; and 3) final approval of the version to be published. Authors should meet conditions 1, 2, and 3.
Acquisition of funding, collection of data, or general supervision of the research group, alone, does not justify authorship.
An author should be prepared to explain the order in which authors are listed.
Acknowledgment
The study was fund by Program for Innovation Team Building at Institutions of Higher Education in Chongqing in 2016 (CXTDG201602006), Chongqing Municipal Key Laboratory of Oral Biomedical Engineering of Higher Education, Health and Family Planning Commission of Chongqing (2015MSXM053) and by Chongqing Research Program of Basic Research and Frontier Technology ([2014]42), Chongqing, China.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. The study was funded by the Program for Innovation Team Building at Institutions of Higher Education in Chongqing in 2016 (CXTDG201602006), Chongqing Municipal Key Laboratory of Oral Biomedical Engineering of Higher Education, Health and Family Planning Commission of Chongqing (2015MSXM053) and by Chongqing Research Program of Basic Research and Frontier Technology ([2014]42), Chongqing, China.
- Received May 9, 2017.
- Accepted July 12, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.