


Abstract
The iliac vein is an extremely rare site for mesenchymal chondrosarcoma, and patients with primary extraskeletal mesenchymal chondrosarcoma arising from a vein always suffer a very poor prognosis. We report a case of a 45-year-old female who presented with a 5-month history of left leg edema in 2015. Contrast-enhanced computed tomography showed a large mass in the left iliac vein with scattered calcifications. Wide-margin resection was performed, and histopathologic and immunohistochemical analyses confirmed the presence of intraluminal mesenchymal chondrosarcoma with local invasion out of the vein wall. Due to poor patient compliance, postoperative neoadjuvant chemotherapy and radiotherapy were not started, and a bone scan performed 16 weeks postoperatively showed multiple bone metastases. The patient died on the twenty-fourth postoperative week.
Mesenchymal chondrosarcoma is a rare and highly malignant tumor with a poor prognosis corresponding to a 5-year survival rate of 54.6% and a 10-year survival rate of 27.3%.1 It can occur at extraskeletal locations and is mainly found in the soft tissues of the orbital, cranial, and spinal meningeal coverings and lower limbs.2,3 Primary venous mesenchymal chondrosarcoma is extremely rare.4,5 We report here a case of primary mesenchymal chondrosarcoma arising from the iliac vein.
Case Report
Patient information
A 45-year-old female presented in December 2015 with a 5-month history of left leg edema (Figure 1).

Timeline of a 45-year-old female presented with a 5-month history of left leg edema.
Clinical findings
On physical examination, no ulceration or pigmentation was observed. No lymphadenopathy was present in the inguinal region. There was no history of trauma, and her personal and family medical histories were unremarkable.
Diagnostic assessment
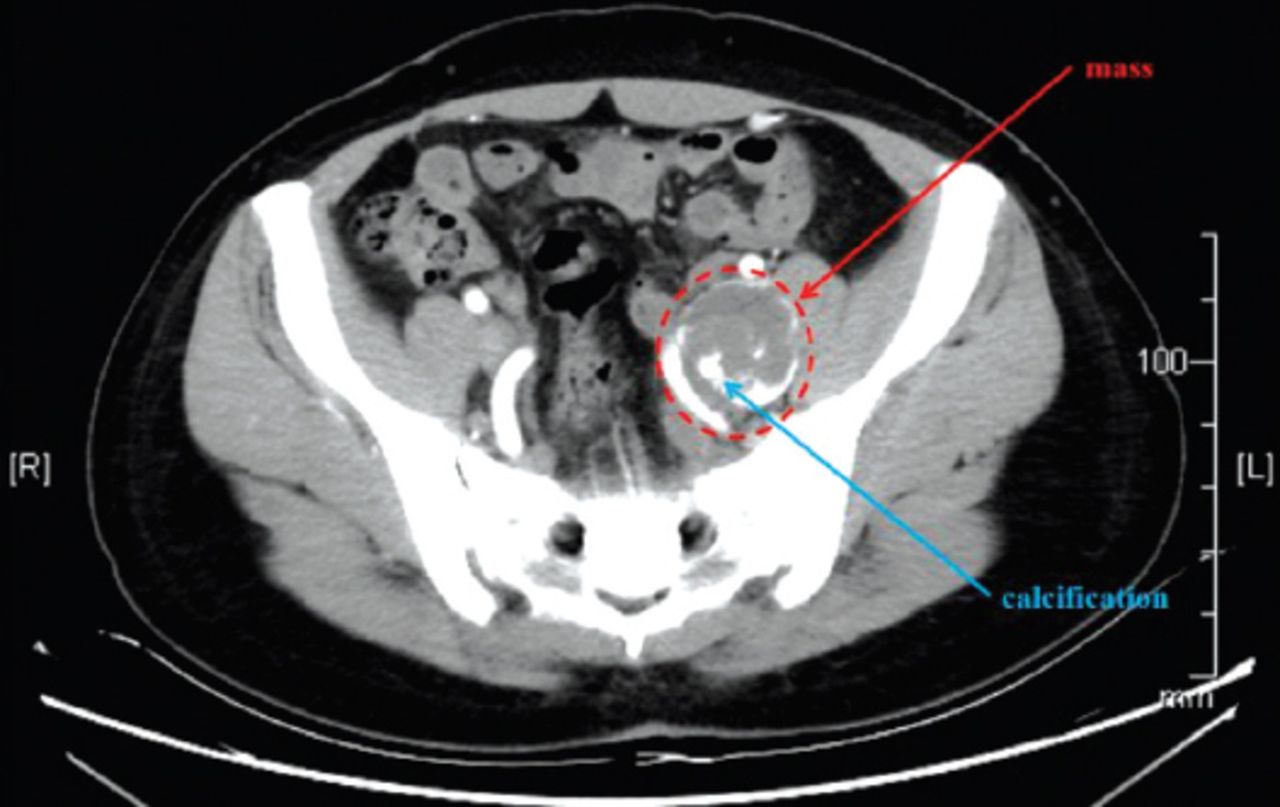
Contrast-enhanced computed tomography showed a large lobulated mass in the left iliac vein with scattered calcifications, and the intraluminal mass extended to the confluence of the left external and internal iliac veins (Figure 2). Routine chest x-ray, abdominal ultrasound, and bone scanning were performed, and no evidence of distant metastasis was found. In additional laboratory tests, the patient’s red blood cell count (RBC) was 1.72×1012/L and hemoglobin (Hb) was 49 g/L. After a blood transfusion, the anemia was rectified with the RBC increasing to 2.63×1012/L and Hb to 83 g/L.

Contrast-enhanced computed tomography revealed a large mass (red arrow) in the left iliac vein and scattered calcification (blue arrow).
Therapeutic intervention
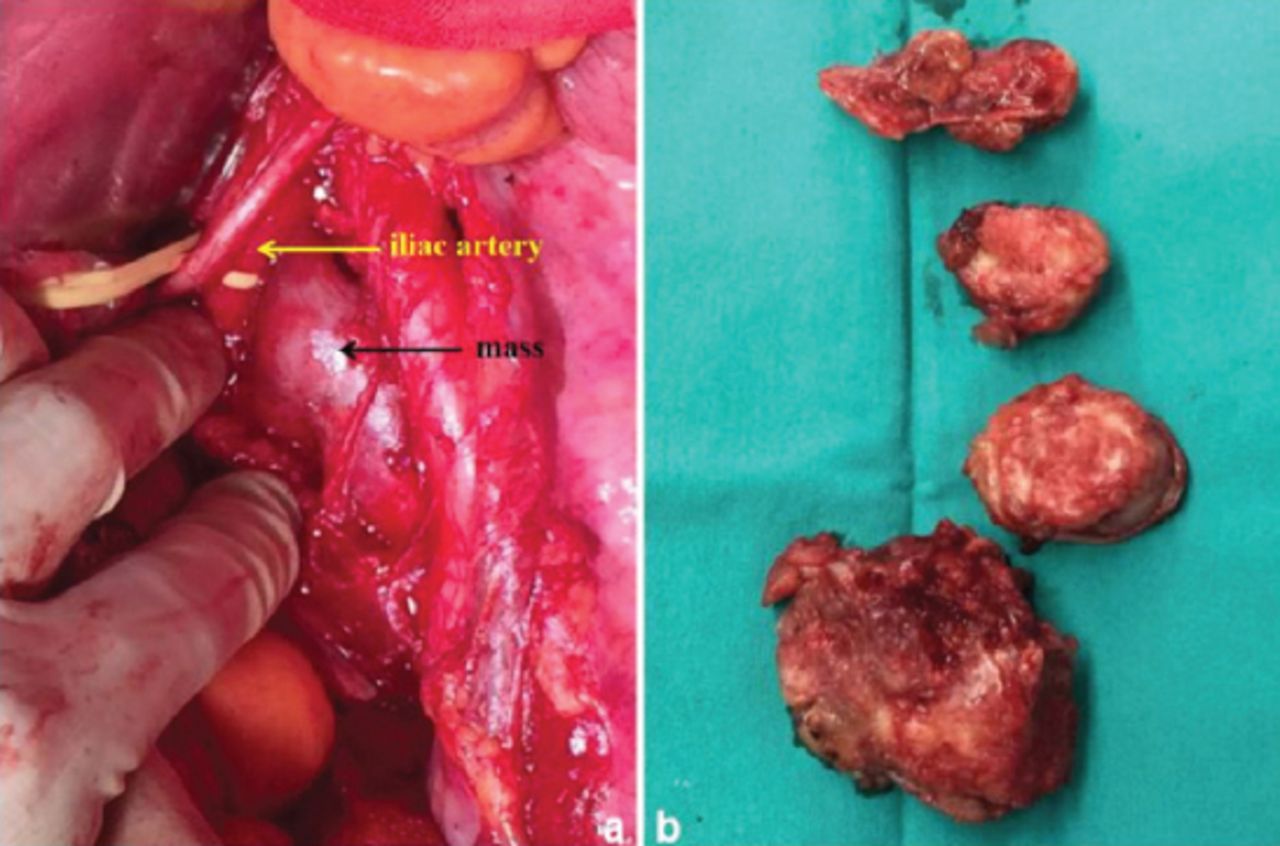
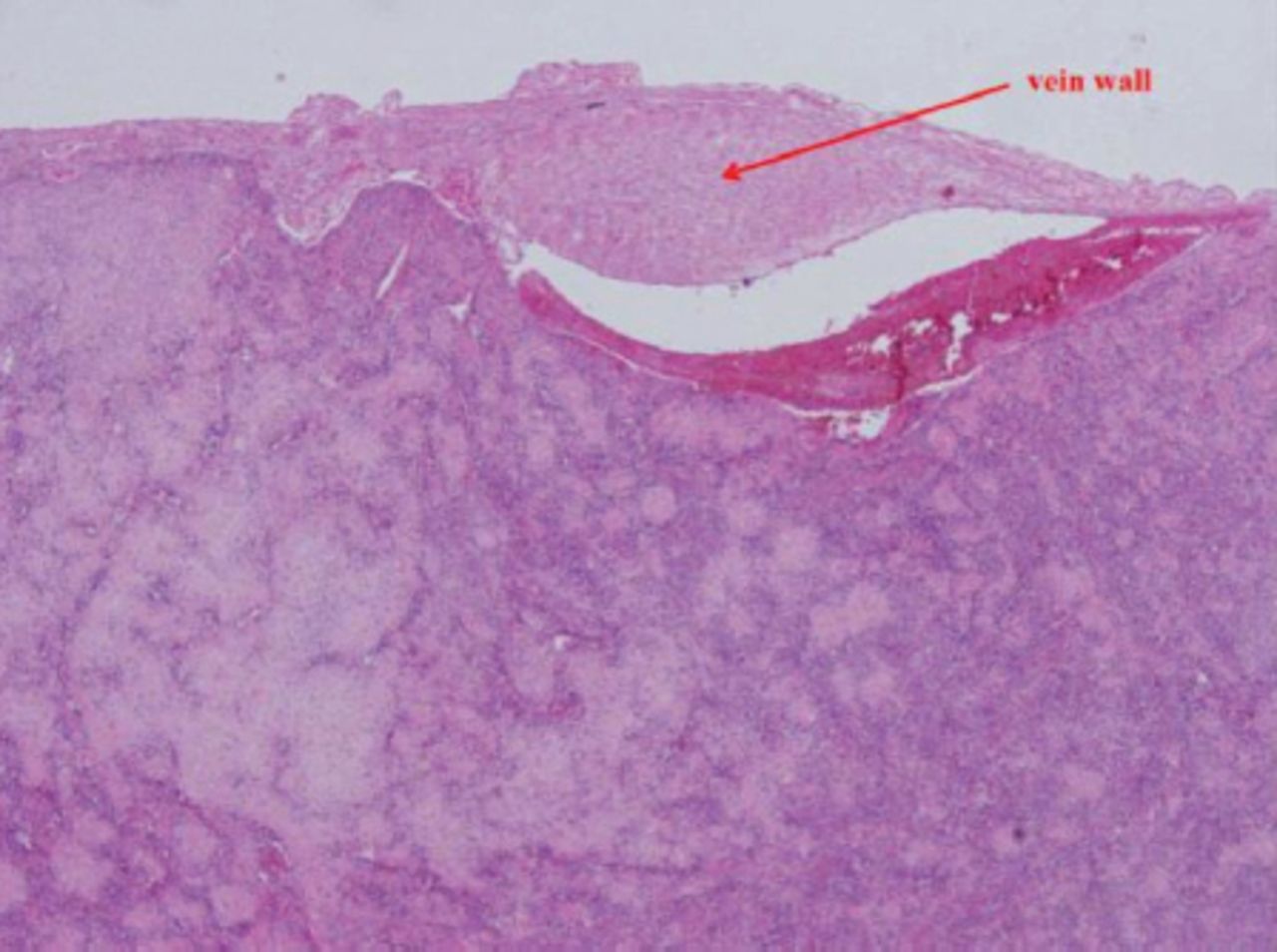
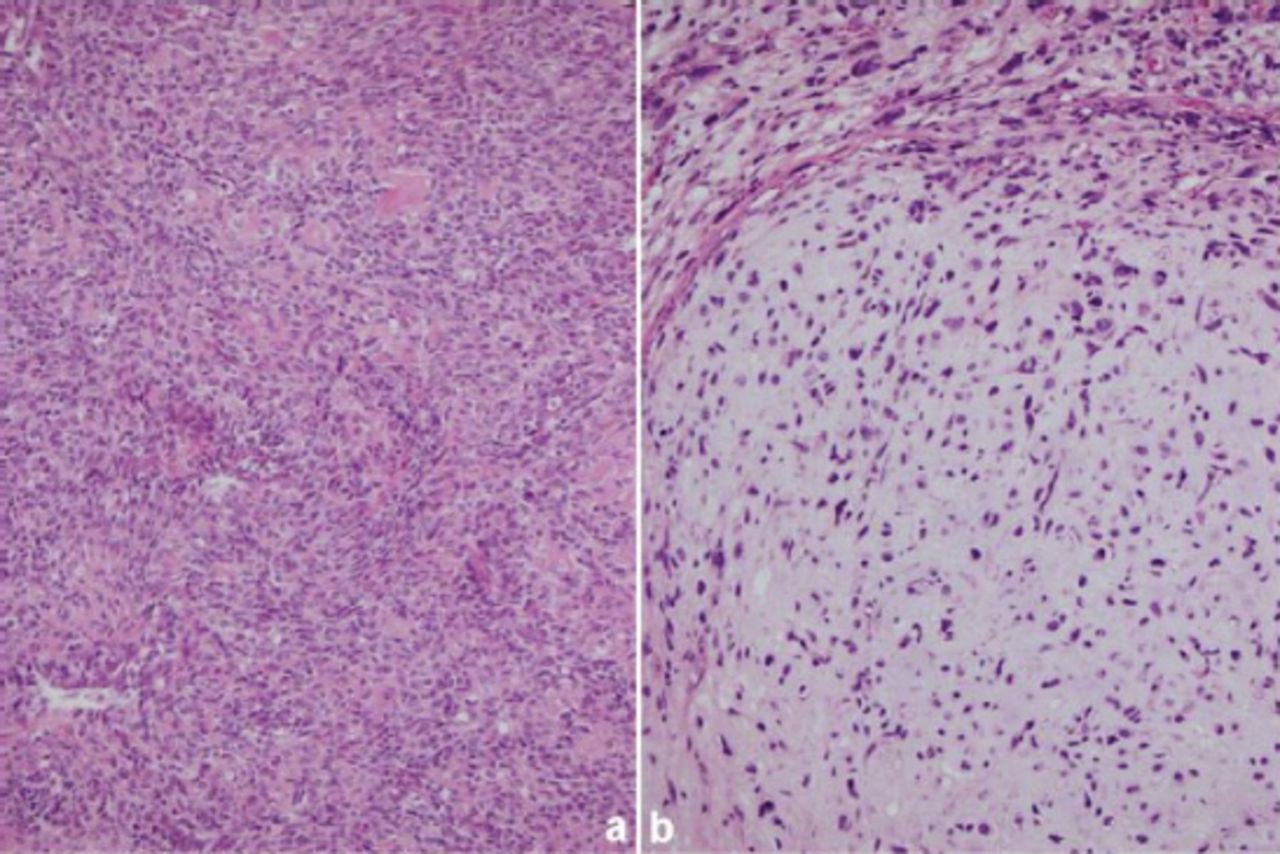
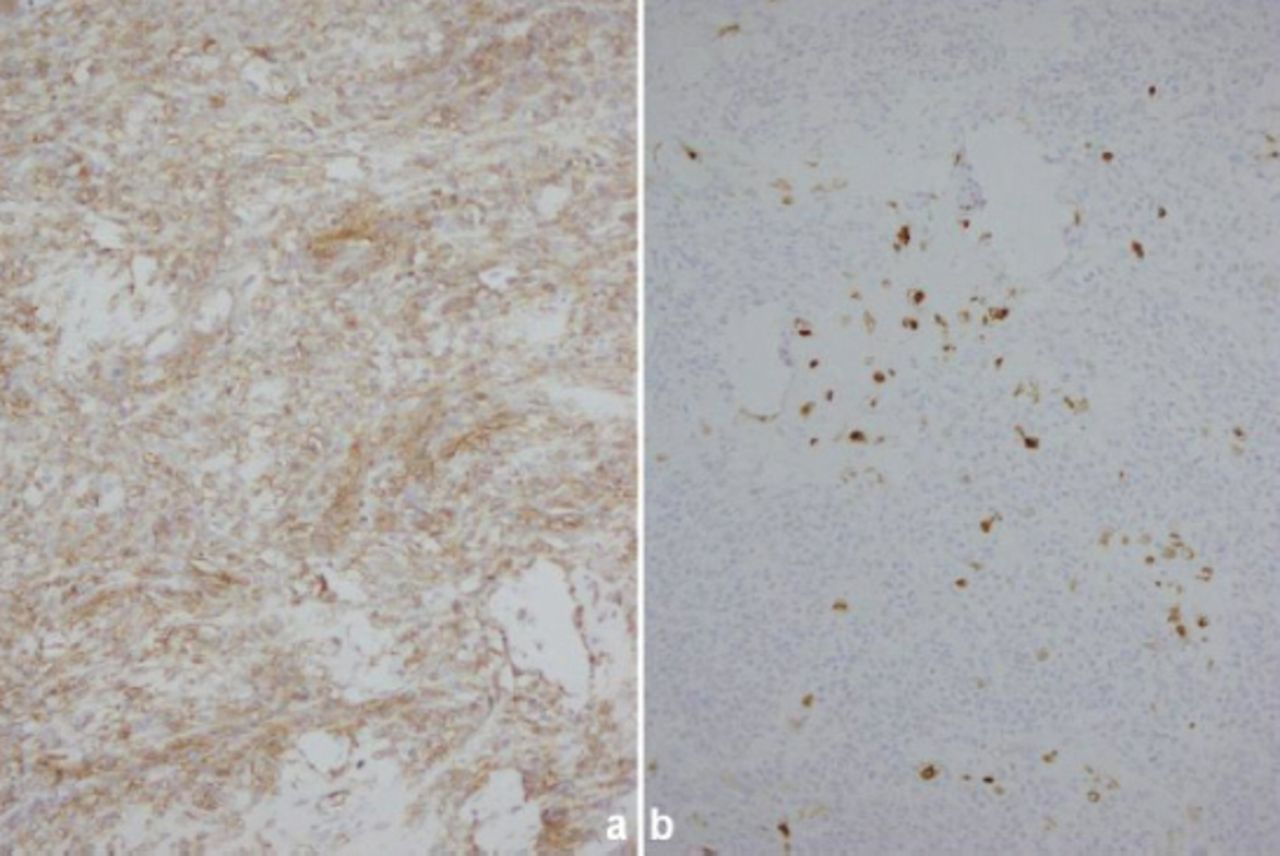
Surgical resection was performed while the patient was under general anesthesia. A skin incision was made in the left lower abdominal region. The iliac artery was dissected, and the iliac vein mass was found to be a tumor measuring 82×36×33 mm with rich blood supply and adherence to the surrounding muscle. The tumor encompassed the confluence of the external and internal iliac veins, and the intraluminal mass was unmovable. After intravenous injection of 4000 U of heparin, the tumor was resected and sent for preparation of frozen sections for histopathologic analysis, which indicated the mass was an intraluminal malignant tumor. To avoid recurrence and metastasis, we performed a wide-margin resection (expanded the resection margins to 50 mm) from the proximal and distal ends of the normal veins. Considering the rich pelvic collateral circulation, the proximal and distal ends were severed. The intraluminal portion of the mass was mostly pinkish-gray and solid (Figure 3). Histopathologic examination showed that most of the mass was confined within the venous intima, and local invasion out of vein wall was present (Figure 4). There was no invasion into the margin of the surgical specimen. Moreover, the mass showed a bimorphic pattern, with areas of poorly differentiated small cells and well-differentiated chondral islands. Calcification and chondrosteosis were present in some areas. The poorly differentiated small cells had ovoid or elongated hyperchromatic nuclei and scant cytoplasm (Figure 5A). The chondral regions were relatively well-defined islands of benign-appearing chondroid tissue (Figure 5B). Immunohistochemical staining showed that the poorly differentiated small cells were positive for CD99 but those in the chondral regions were negative for CD99 (Figure 6A). However, the cells in the chondral regions were positive for S100 (Figure 6B).
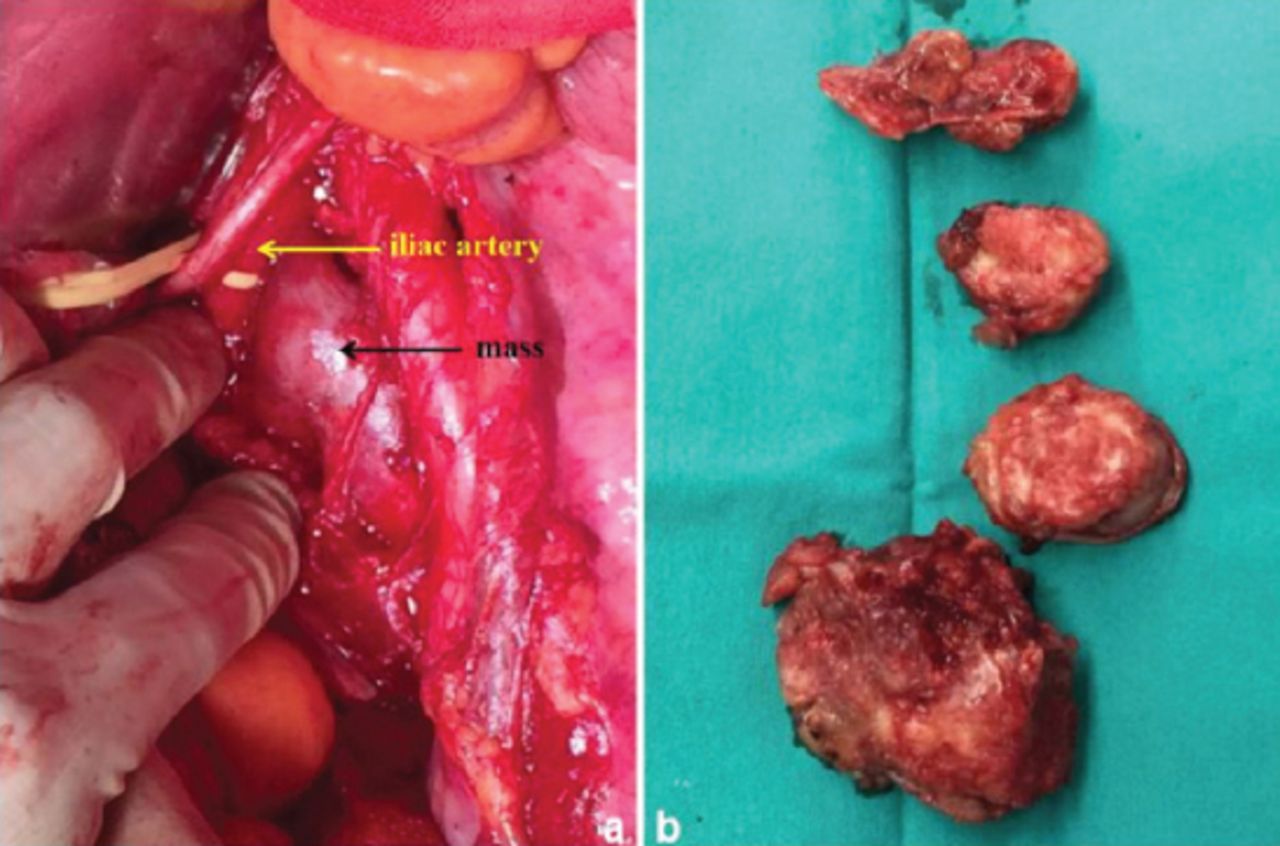
Images showing that: A) the mass (black arrow) was next to the iliac artery (yellow arrow); and B) the excised mass was mostly pinkish-gray and solid.

Histopathologic examination (magnification, 40×) showed that most of the mass was confined within the vein wall (red arrow).

Histopathologic examination (magnification, 200×) revealed: A) ovoid or elongated hyperchromatic nuclei and scant cytoplasm in the poorly differentiated small cells; and B) chondroid tissue in the chondral regions.

Histopathologic examination (magnification, 200×) revealed: A) ovoid or elongated hyperchromatic nuclei and scant cytoplasm in the poorly differentiated small cells; and B) chondroid tissue in the chondral regions.
Follow-up and outcomes
The patient was discharged 6 days after surgery, and we advised her to start neoadjuvant chemotherapy and radiotherapy in the third week postoperatively. However, the chemotherapy and radiotherapy were never started due to poor compliance. Finally, a bone scan performed 16 weeks postoperatively showed multiple bone metastases, and the patient died on the twenty-fourth postoperative week.
Discussion
Mesenchymal chondrosarcoma is a rare tumor characterized by chondrogenesis. In literature, there has not been case suffered the tumor arising from the iliac vein yet. It was first reported by Lichtenstein and Bernstein in 1959.6 As a rare tumor in bone and soft tissue, it accounts for 3% to 10% of all chondrosarcoma and 0.2% to 0.7% of all bone tumors.1 Most patients are 10-50 years old with no significant gender difference.7 With high rates of recurrence as well as local and distant metastasis, patients usually suffer a poor prognosis8 (Table 1).
Published studies reporting on the prognosis of mesenchymal chondrosarcoma.
Primary venous tumors, including leiomyosarcoma, hemangioendothelioma, and mesenchymal chondrosarcoma, are clinically uncommon. They share features of high malignancy, rapid growth, rich blood supply, and local venous thrombosis. In general, primary venous leiomyosarcoma usually is found in the inferior vena cava and lower extremity veins. In 1992, Dzsinich et al9 conducted a retrospective study of 210 cases of primary venous leiomyosarcoma and reported that approximately 33% of cases occurred in lower extremity veins, with most tumors found in the great saphenous veins, femoral veins, external iliac veins, and popliteal veins. Leiomyosarcoma mainly originates from vascular smooth muscle cells, and the typical microscopic manifestations include disordered arrangement of muscle fibers and small spindle cells, with positive staining for eosinophilic cytoplasm, desmine, and actine, of which the latter 2 are immunohistochemical staining markers of smooth muscle cells. It is difficult to distinguish leiomyosarcoma from mesenchymal chondrosarcoma based on clinical signs, radiological images, and ultrasonic examination. Hemangioendothelioma mainly originates from vascular endothelial cells with less potential for metastasis. In addition, primary venous non-Hodgkin’s lymphoma was reported, and proliferation and invasion of lymphocytes in vascular tissue were reported.10
Chondral calcification can be found through radiological examination in mesenchymal chondrosarcoma, but it is not specific.3 Notably, histopathologic and immunohistochemical examinations are the main methods for identifying mesenchymal chondrosarcoma. Moreover, the latter is very important for distinguishing mesenchymal chondrosarcoma from Ewings sarcoma, lymphoma, hemangiopericytoma, and embryonal rhabdomyosarcoma. The typical histopathologic manifestation of mesenchymal chondrosarcoma is disordered arrangement of well-differentiated chondral lesions and poorly differentiated mesenchymal lesions, which is called dimorphism.1,6 Calcification and chondrosteosis in chondral lesions and transitional zones between chondral lesions and mesenchymal lesions can be found in histopathologic examination.1 Furthermore, the mesenchymal lesions are always CD99(+), Leu7(+), and S-100(-), the chondral lesions are S-100(+).1,2 In the present case, calcification and positive staining for S-100 were found in chondral lesions, and the mesenchymal lesions were CD99(+) and S-100(-).
In conclusion, primary extraskeletal mesenchymal chondrosarcoma in any location is very rare, and patients always suffer a poor prognosis. The patient in the present case died on the twenty-fourth week postoperatively. Further, case series studies are needed to provide systematic diagnostic criteria and treatment recommendations for primary extraskeletal mesenchymal chondrosarcoma.
Acknowledgment
Authors gratefully acknowledge Dr. Sean Luo, Wake Forest Baptist Health, Winston-Salem, NC, USA, for medical editing and writing assistance.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 11, 2017.
- Accepted August 16, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}