


Abstract
Objectives: To determine the applicability of Jones, Hansen, and Wasserman predictive equations for maximal oxygen consumption (VO2max) in Saudi females.
Methods: This cross-sectional study was conducted at Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia, between March and May 2017. Maximal oxygen consumption was measured directly through the COSMED system for cardiopulmonary exercise testing in 102 girls with normal body mass index (19-25 years old). Maximal oxygen consumption was indirectly predicted by Jones, Hansen, and Wasserman equations. Paired t-test, Pearson correlation, and Bland-Altman plot were used for comparison, correlation, and agreement analysis.
Results: The difference between the mean and standard deviation (±SD) VO2max values of the direct measurement (27.39±4.06 ml/kg−1/min−1), and the Jones (35.19±2.12 ml/kg−1/min−1), Hansen (33.64±0.24 ml/kg−1/min−1), and Wasserman (35.20±0.17 ml/kg−1/min−1) equations, was statistically significant (p<0.001). Bland-Altman plot analysis suggested a lack of agreement between direct and predicted VO2max. Pearson correlation failed to reveal any correlation between direct VO2max and VO2max calculated with any of the 3 equations.
Conclusion: Jones, Hansen, and Wasserman equations for prediction of VO2max cannot be justified in the studied population. For the better prediction of VO2max, either these equations should be modified, or a new equation should be developed for the Saudi population.
Exercise is prescribed as the first line of treatment for several medical problems in the modern world. Cardiorespiratory fitness/maximal oxygen consumption (VO2max) testing plays a pivotal role in exercise physiology.1 It helps in developing exercise programs and monitoring the progress of participants in such programs. It apprises people of their current fitness status while comparing it to norms and identifies high-risk individuals. Maximal oxygen consumption is an important physiological variable that is strongly associated with decreasing the risk of developing cardiovascular diseases (CVD).2 According to an international meta-analysis by Kodama et al,3 13% reductions in all-cause mortality and 15% reductions in coronary heart/vascular disease morbidity, can be achieved by just a 12% improvement in VO2max. Given that cardiovascular disease accounts for 37% of all deaths in Kingdom of Saudi Arabia, a readily available measure of VO2max would be very useful in clinical settings.
The gold standard method of measuring VO2max is expired gas analysis during an incremental exercise test to exhaustion using a treadmill or cycle ergometer.4,5 However, despite the reliability and accuracy of the gas analysis, its use is limited because it requires expensive high-tech equipment and the assistance of trained personnel. This makes it infeasible for use in most clinical/research settings.6 Moreover, accurately measuring VO2max involves an intense physical effort which certain older or higher-risk individuals may not be able to perform. To address these issues, researchers have generated several non-exercise-based equations using variables for predicting VO2max, such as age, weight, height, body mass index (BMI), body fat percentage, gender, and so forth.1
A majority of the VO2max prediction equations have been derived from studies of Western populations.7-9 Race or ethnicity is a persistent determinant of VO2max due to inter-racial variations in genetically determined race-specific skeletal muscle properties and hemoglobin concentration.10,11 In addition to race, other variables that may affect VO2max are body composition, nutrition, physical activity, and socioeconomic factors.12 Owing to this, prediction equations derived from one population may not accurately measure VO2max in other populations. Multiple studies have reported such interracial differences.13-16 Because of these facts, prediction equations for estimating VO2max derived from the Western population might not accurately reflect the results among Asian Arabs. The objective of the current study was to measure VO2max directly and cross-validate the 3 Caucasian-based internationally published VO2max prediction equations (Jones, Hansen, and Wasserman) in the Saudi female population.17,18 The female version of these equations was selected.
Methods
This cross-sectional study was conducted in the Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia, between March and May 2017. The sample size was calculated using G*power 3.1 statistical power analysis software version 19 based on the calculation of the effect size to give a power of 95%. The effect size 0.39 was calculated using the mean VO2max value of the null hypothesis (H0: 33.7), the standard deviation (SD: 10.97) (mean VO2max and SD values were taken from the local study).20 Meanwhile, the mean VO2max value of the alternative hypothesis was (H1: 40). The participants (n=102; age 19-25 years) composed of Saudi young females recruited from various health colleges in Imam Abdulrahman Bin Faisal University in Dammam, Kingdom of Saudi Arabia. Simple random selection was performed using a Microsoft excel sheet. Each student in these colleges was allotted a random value. Later, the values were sorted in ascending order and the required sample was chosen from the top of the list.
The recruitment was carried out via phone. Criteria for inclusion in the study were apparently healthy females, having a normal body mass index (BMI) of 18.50-24.99 (kg/m−2), and sedentary as defined by the international physical activity questionnaire.21,22 Students with prior history of cardiovascular diseases, respiratory diseases, orthopedic or musculoskeletal lesions, taking any regular medication, lactating, pregnant or smokers were excluded. Prior to testing, written informed consent was obtained from all eligible participants. The research was approved by the Institutional Review Board of the university (IRB approval number: IRB-PGS-2017-01-219). All procedures were performed according to the principles of the Helsinki Declaration.
Height was measured in centimeters (cm) by a stadiometer (Seca, Hamburg, Germany; Model 217) and the body mass was measured in kilograms (kg) by a digital weight scale (Seca, Hamburg, Germany; Model 8813306100327), while the participant wore lightweight clothing and no shoes. Participants were instructed to drink plenty of water and avoid vigorous physical activity one day before testing and to not consume heavy meals or caffeine for 3 hours prior to testing. Maximal oxygen consumption was measured using the COSMED system for cardiopulmonary exercise testing (Quark CPET, COSMED, Rome, Italy; Model C02900-01-04). The system was calibrated in accordance with the manufacturer’s instructions. Participants were asked to rest quietly for 5 minutes before resting heart rate (HRrest) was measured using the 3 bipolar leads of electrocardiogram. During the test, all subjects performed a maximal exercise test on a stationary bicycle ergometer using a one-minute incremental test. The height of the seat was adjusted to keep the subject’s legs at near full extension during each pedal revolution.23 The selection of the work rate increment was calculated using the previously published formula.24 Briefly, the formula were: oxygen uptake (VO2) unloaded in milliliters per minute= (150+6* body mass in kilograms); peak VO2 in milliliters per minute (height in centimeters - age in years) *14 for sedentary women; work rate increment per minute in watts equals (peak VO2 in milliliters per minute-VO2 unloaded in milliliters per minute)/100.
After a period of rest, the incremental protocol allowed the subject initially to cycle for 3 minutes of unloaded pedaling as a warm-up period. Then, the power output started at 20 Watts and was increasingly incremented by 15 Watts every minute by computer control until the subject was limited by debilitating symptoms despite verbal encouragement. The cycling frequency was maintained at 50 revolutions per minute (rpm) throughout the exercise. Finally, the subjects were asked to continue cycling for 3 minutes without resistance in the recovery period. Time until exhaustion (TTE) was recorded to exclude the subjects who took longer than optimum time (6-12 minutes) for recording VO2max. Subjects were asked about the reason of stopping the exercise test.
The subjects wore a nose clip and breathed through a mouthpiece. Metabolic gases were collected using breath by breath gas analysis system. The participants’ heart rate (HR) and blood pressure were monitored every 2 minutes. Ratings of perceived exertion (RPE) score was recorded at the end of each stage. The Borg rating of perceived exertion scale was specifically used. It rates the intensity of the exercise from 6 to 2025 and duration. Respiratory exchange ratio and VO2max was considered valid when at least 2 of the following criteria were met: plateau of oxygen consumption despite an increase in workload; respiratory exchange ratio of ≥1.1; age-predicted maximal heart rate (220- age); and RPE of ≥17.25
The plateau of oxygen consumption was determined by the maximum value of VO2 achieved by the subject as a clear plateau of VO2 max in the graph of VO2 versus time was difficult to be obtained from all subjects.
The American College of Sports Medicine (ACSM) Guidelines of indications for terminating exercise testing were followed.26 Subjects were excluded from the study as they did not reach VO2max. For indirect VO2max calculation, following 3 prediction equations were used: Jones et al,17 (Jones 2 equations): VO2 (l/min−1)= -2.26+0.025 *height+0.01 −body mass-0.018 −age. Hansen et al,17 (Hansen/Wasserman equations): VO2 (l/min−1) = 0.001 −height −(14.783-0.11 −age) + 0.006 −body mass (actual-ideal), age of 30 years was put for adults younger than 30 years; ideal body mass = 0.65 −height-42.8). Wasserman et al,18 equation: VO2 (l/min−1) = (body mass + 42.8) − (22.78-0.17 −age)/1000.
In all the aforementioned equations, height was in cm, body mass was in kg and age was in years. The results of the predicted VO2max from these equations were converted from (l/min−1) to (ml/min−1) for comparison with the actual VO2max values.
The Statistical Package for Social Sciences, version 22 (IBM Corp., Armonk, NY, USA) was used to perform the statistical analyses. Testing for normality of distribution was performed by using Shapiro-Wilk test. Mean±SD, minimum and maximum were obtained by descriptive statistics. Paired t-test was used to compare direct VO2max with predicted VO2max obtained by 3 different equations. Pearson correlation test was run to find out the possible correlation between direct VO2max and predicted VO2max. Bland-Altman plots were used to analyze the agreement. For Bland-Altman plots, mean difference between the 2 methods of measurement, namely, the actual and predicted VO2max values and mean of the 2 methods of measurement were calculated.27
Results
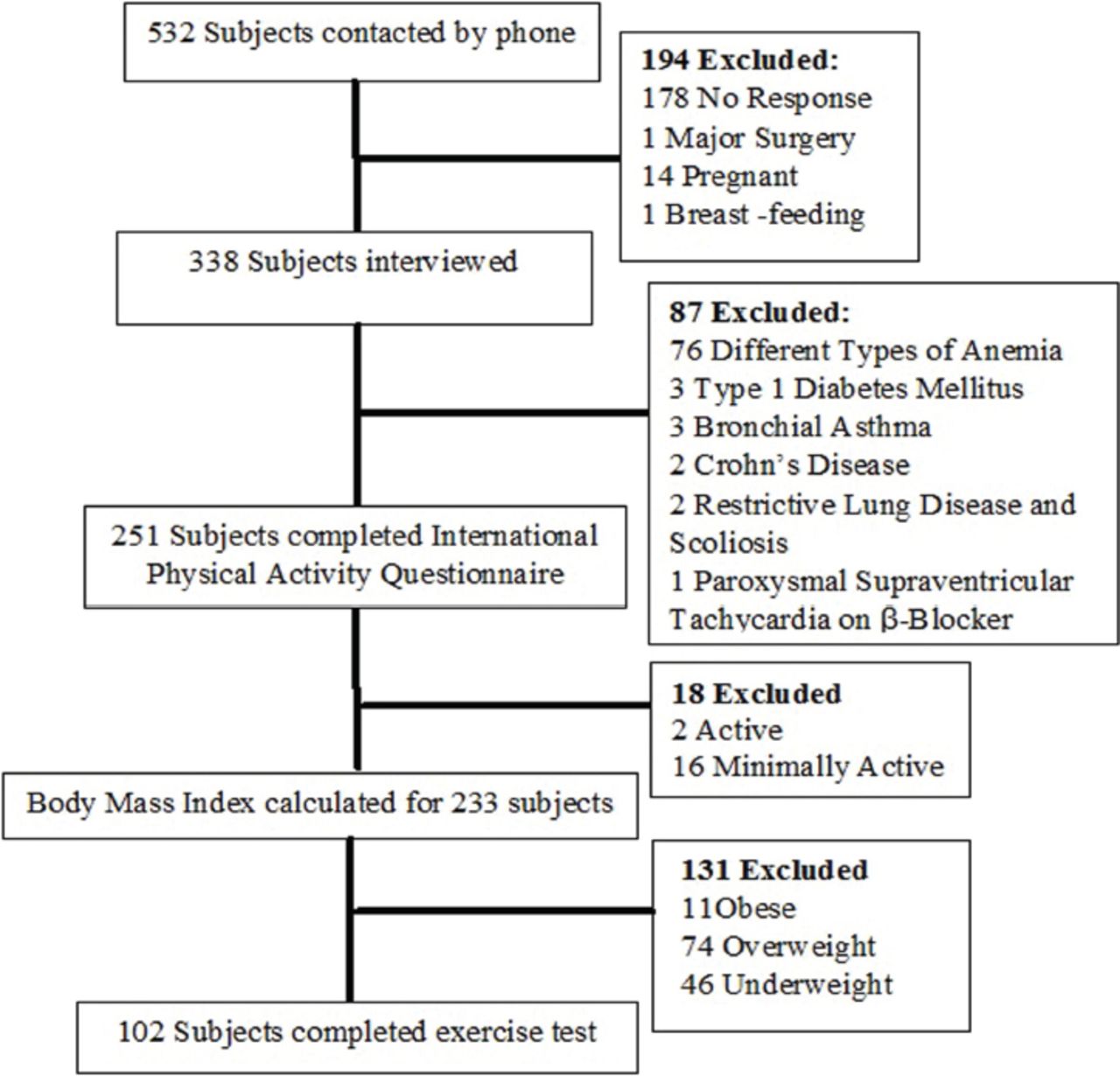
The selection of study participants as shown in Figure 1. Table 1 provides the baseline characteristics, direct and predicted VO2max values. Approximately 21.6% of the participants were having “very poor” VO2max, whereas 53.92% of participants had “poor” VO2max as per the fitness categories of Heyward (Table 2).28 Differences between VO2max values measured by direct method (27.39±4.06 ml/kg/minute) and each one of the predicted equations, Jones (35.19±2.12 ml/kg/minute), Hansen (33.64±0.24 ml/kg/minute) and Wasserman (35.20±0.17 ml/kg/minute) were statistically significant (Table 3). In fact, all 3 predictive equation significantly overestimated the VO2max compared to direct method measured value (Table 1). Table 3 shows the p-value obtained by paired t-test, mean difference and 95% limits of agreement of all 3 predicted equations.

Selection of 102 participants.
Physical parameters and predicted and measured VO2max values of the 102 participant.
Classification of the participants’ VO2max values based on physical fitness specialist certification manual (Heyward, 1997).28
Comparison between direct VO2max and predicted VO2max.
A lack of correlation between direct VO2max and VO2max calculated by Jones (r=0.006, p>0.05), Hansen (r = 0.164, p>0.05) and Wasserman (r = 0.133, p>0.05) equations as shown in Table 4.
Pearson coefficient correlation.
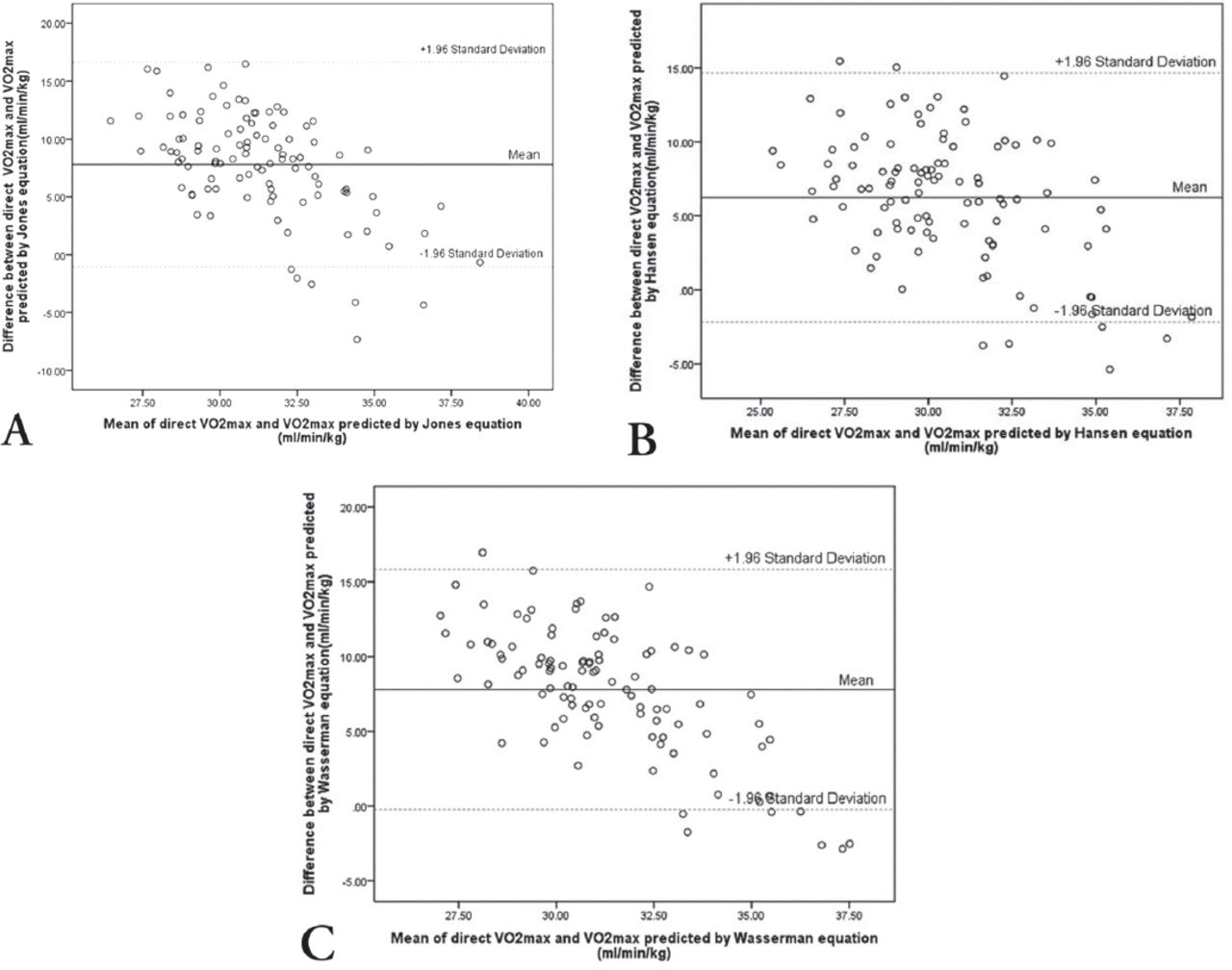
Analysis of the data using the Bland and Altman method for limits of agreement between direct VO2max and VO2max predicted by Jones equation revealed that the limits of agreement were 16.73 to -1.15. With Hansen and Wasserman equations, limits of agreement were 14.81 to -2.33 with Hansen equation and 16.01 to -0.41 with Wasserman equation (Figure 2).

Bland-altman plot showing the difference between actual VO2max and VO2max predicted by A) Jones, B) Hansen, and C) Wasserman equations.
Discussion
The objective of the current study was to determine reference values for VO2max by direct method and to cross-validate equations by Jones, Hansen, and Wasserman for prediction of VO2max in the young Saudi female population. The VO2max values of our study participants, obtained by the direct method, are comparatively lower than those of other populations. In a study involving young, healthy, British females, VO2max was 39.8±7.2 ml/kg−1/min−1, much higher than our values.29 In another study, involving Spanish sedentary nursing college students, VO2max was higher than ours (33.3±7.1 ml/kg−1/min−1).30 The Fitness Registry and the Importance of Exercise National Database (FRIEND) registry reference data of VO2max for a healthy young US female population revealed VO2max values of 30.8±9.4 ml/kg−1/min−1.24 Souza e Silva et al,31 measured VO2max in 101 females with a mean age of 28.5± 5 years and a normal mean BMI. The value of their VO2max was 29.9±7.3 ml/kg−1/min−1. Neder et al,32 studied the VO2max of 20 sedentary female subjects and found it to be 1679±228 ml/min−1 in contrast to 1449.10±233.92 ml/min−1 in our study. The higher values of VO2max in these populations could be justified by the genetic variations or due to higher levels of physical fitness.
As evident from Table 3, compared to directly measured VO2max; the 3 predicted equations overestimated VO2max, with a mean difference of 7.79 (Jones), 6.24 (Hansen), and 7.80 (Wasserman) (ml/min/kg). Hence, our study demonstrated that none of the predicted equations can be applied for use with the studied population (young Arab females). In addition, there is a lack of correlation between the direct VO2max and the VO2max that these equations predict. Limits of agreement analysis suggested no agreement of actual VO2max with any of the predicted equations. Hence, we suggest caution in indirect measurement of VO2max by the Jones, Hansen, and Wasserman equations in the Arab population. Our results are in accordance with Ahmadian et al,33 who reported significantly increased predicted VO2max values derived from these 3 equations (Wasserman, Jones, and Hansen) as compared to direct VO2max in symptomatic patients who underwent cardiopulmonary exercise testing. Likewise, Almedia et al,34 demonstrated a significantly increased (p=0.001) predicted VO2max in a Brazilian population by the Jones equation and the Wasserman algorithm compared to direct VO2max. Although Almedia et al,34 linked this overestimation to variations in the experimental protocol, namely, the use of a cycle ergometer while deriving the equations versus the use of a treadmill while performing the comparison, this justification is less likely in our study, as we used a cycle ergometer for our research. Our results agree to Debeaumont et al,16 who found predicted VO2max through Wasserman et al,18 equation as valid and correlated to actual VO2max in French obese women with metabolic syndrome; however, the accuracy was low on Bland-Altman analysis. That led them to develop a new prediction equation adapted specifically for their studied population. Likewise, Racil et al,35 compared predicted VO2max obtained through Wasserman et al’s,18 and Debeaumont et al’s,16 equations to actual VO2max in obese women and found predicted VO2max by Wasserman equation significantly differed from actual VO2max. Similarly, Scott et al,36 compared 3 prediction equations (Scott et al,36 and 2 commonly used FitnessGramTM equations) with actual VO2max in children and reported that both FitnessGram™ equations significantly underestimated the VO2max.
Several factors, such as ethnicity, genetics, habits, body composition, and physical activity, vary from population to population. Predicted equations derived from one population and cross-validated in the same may not provide an accurate VO2max in another population.1,8 Hence, either these equations should be modified, or new equations should be derived in other ethnic populations. Thus, our study supports the development and validation of population-specific prediction equations for the estimation of VO2max in the Saudi population.
Study limitations
The present study has some strengths. A key strength was that the VO2max was measured directly, which is the gold standard test for cardiopulmonary fitness. Also, the study has cross-validated prediction equations in the Saudi population. Because VO2max changes with gender, increasing age, and degree of physical activity, we limited our study to females who were sedentary and aged 18-25 years, thereby eliminating these confounding variables. However, one limitation was that all our subjects were females, and recruited from a single university. Therefore, our findings cannot be generalized.
In conclusion, our results indicate that young Saudi females may have poor cardiorespiratory fitness. Probably, there is a need to develop a new equation or to modify the previous equations for the prediction of VO2max in the Saudi population so that accurate measurements of VO2max can be obtained, resulting in a reduced mean bias, a narrower limit of agreement, and a significant correlation with direct VO2max. We suggest further research to be undertaken with a greater number of participants and wider age ranges.
Copyright
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
Acknowledgment
The authors gratefully acknowledge Correction Perfection (www.cperfection.com) for English language editing.
Footnotes
Disclosure. This study was funded by the Deanship of Scientific Research, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia (Grant Number 2015292).
- Received March 19, 2019.
- Accepted June 19, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.