


Abstract
Objectives: To investigate the effectiveness of a bone-anchored hearing implant system (Bonebridge implant technology) as a rehabilitation treatment for individuals with conductive or mixed hearing losses.
Methods: This is a retrospective cohort study. Twelve implanted ears with conductive or mixed hearing losses were implanted with this device at a tertiary university hospital between 2012 and 2016. Audiological tests included pure tone air conduction (AC) and bone conduction (BC) measurements and unaided and aided sound-field thresholds. To evaluate the speech intelligibility in a quiet environment, the speech discrimination score (SDS) was tested using Arabic monosyllabic words, and the speech reception threshold (SRT) was measured using Arabic disyllabic words spoken in front of them. The subjective sound quality was assessed with the Hearing Implant Sound Quality Index (HISQUI).
Results: In comparison with the unaided condition, there was a significant improvement in the aided thresholds, SDS, and SRT. Comparing the aided and unaided thresholds, the average AC threshold improved with an average functional gain of 40±6.3dB. The unaided SRT improved from 72.5 dB hearing levels (HL)(median) to 27.5 dB HL (median) when aided, and patients performed 71% better, on average, based on the SDS with the help of the device. The HISQUI questionnaire revealed high satisfaction with the device sound quality.
Conclusion: Patients with conductive and mixed hearing loss substantially benefit from the Bonebridge active transcutaneous BC hearing implant.
The air conduction (AC) pathway is modified, restricted, or completely lost in patients with conductive or mixed hearing loss. Although defects of the tympanic membrane and the ossicular chain can be treated to a certain extent by surgery, adequate hearing restoration is not achieved in some cases even with the addition of conventional hearing aids. Active bone conduction (BC) implants can be beneficial to these patients as BC transmission of the acoustic signal bypasses the normal AC pathway.1 Consequently, BC hearing implants have become a mainstream treatment for conductive, mixed, or single-sided hearing loss that does not benefit from conventional hearing aids.2 Attempts to effectively restore hearing in these patients have included surgical implantation of percutaneous BC implants. Although effective, safe, and well-established in the market, they were associated with a significant number of post-operative complications leading to revision surgery.3 In an extensive series of patients (n=602) over a 20-year period, Hobson et al4 reported a complication rate of 24% and a revision surgery rate of 12%. Therefore, the transcutaneous BC implants were introduced to minimize the complication rate.
The Bonebridge System (BB, Med-El Corporation, Innsbruck, Austria), is one of these transcutaneous bone conduction hearing implants. It is an intact skin semi-implantable hearing system consisting of 2 components: the external audio processor and the internal implantable part known as the BC implant. The transcutaneous BC implants including BB avoids drawbacks associated with percutaneous implants such as skin reactions, the growth of skin over the abutment, implant extrusions, wound infections, and fixture losses. Therefore, it is reported that, the complication rate is higher in percutaneous BC implant in comparison with transcutaneous one.5 As the BC-implant is secured to bone by screws, the osseointegration process is not required and the device may be activated within 2 or 3 weeks after it is implanted.
It is reported that, the performance of active transcutaneous bone conduction hearing implant is also superior to the passive skin-drive BC devices with implanted magnets that are subjected to atranscutaneous signal attenuation of 10 to 15 dB,6 because in active transcutaneous BC implant the signal is independent from the thickness of the skin and hair.
The purpose of the present study was to evaluate the audiological outcome as well as the speech benefit of the BB implanted patients in our center.
Methods
After approval by the Institutional Review Board of King Saud University, College of Medicine, Riyadh, Saudi Arabia data were retrospectively compiled for this study. We reviewed hospital charts of 12 implanted ears that received BB implantations at our university hospital (tertiary referral center) between July 2012 and February 2016. All implanted patients during that period have been included. The incomplete file was our exclusion criteria. Data regarding the general demographics as well as the cause of deafness, onset and duration of deafness, number of patients who had minor or major complications, or those who required revision were collected.
Prior to implantation, pure tone AC and BC thresholds were obtained in both the unaided and aided conditions. When calculating the puretone average (PTA4), the 0.5,1, 2, and 4 kHz thresholds were utilized. The functional gain was calculated as the difference between the mean PTA4AC and aided PTA4.
To evaluate the speech intelligibility, the speech discrimination score (SDS) was tested using Arabic monosyllabic words; speech stimuli were presented at 65 dB hearing level (HL) in a quiet environment. The speech reception threshold (SRT) was measured using Arabic disyllabicwords (50% correct) with speech and the noise signal arriving from the front. All hearing tests were performed monaurally, where the contralateral side plugged and masked while testing the implanted ear.
The Hearing Implant Sound Quality Index (HISQUI) questionnaire was used to evaluate the subjective sound quality of the BB. The questionnaire consists of 29 questions with 7 possible answers each, ranging from “never” to “always”. An example question is: “Can you effortlessly distinguish between a male and a female voice?” Each answer has a value between 1 and 7, those values are totaled to obtain the HISQUI score. The HISQUI score corresponds to one of 5 categories between poor and very good sound quality.
Post-operative BB-aided thresholds and audiological data obtained in one-year follow-up visits were compared to the preoperative results. Due to the low number of data points, a normal distribution of the data could not be confirmed. The non-parametric Wilcoxon test was performed to test for significance between groups and the software STATISTICA 12 was used. Graphs were created using GraphPad Prism 7.02.
Results
The individual demographic and clinical data for 12 implanted ears are shown in Table 1. In 9 ears, the BC-FMT was placed in the sinodural angle and in 3 ears the BC-FMT had to be placed using a retrosigmoid approach. No intraoperative, minor, or major postoperative complications were observed. There was no incidence of revision surgery in any of the patients.
Demographic and clinical data of 12 implanted ears.
Pure tone audiometry
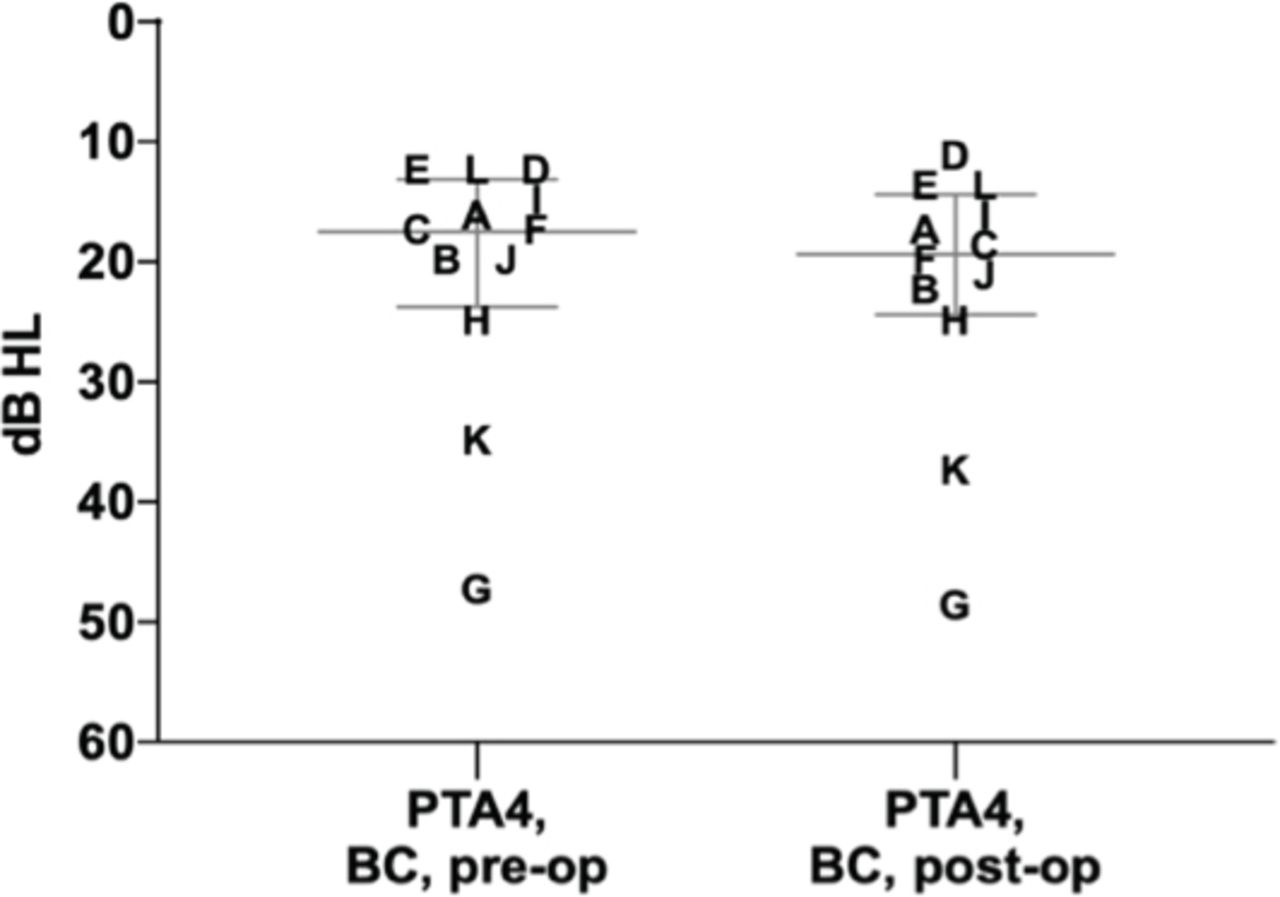
We compared the pre- and post-operative BC thresholds (PTA4BC) to assess the safety of the surgical procedure. The difference was not larger than 5 dB for any patient; thus, all were within the accuracy interval of the BC measurement (±5 dB) (Figure 1).

A comparison of bone conduction (BC) thresholds as pre-operation (pre-op) versus post-operation (post-op) puretone average (PTA4) values. The plot shows the individual data points and each letter represents a tested ear (n=12) and the median (long line) with the interquartile range (25th and 75th percentile, whiskers). The greatest difference between pre- and post-op BC PTA4 values is 2.5 dB hearing levels (HL) (ear B, F and K), which is within the retest variability of 5 dB. Consistent with this trend, all frequency related post-op BC values differ less than 5 dB from the pre-op value.
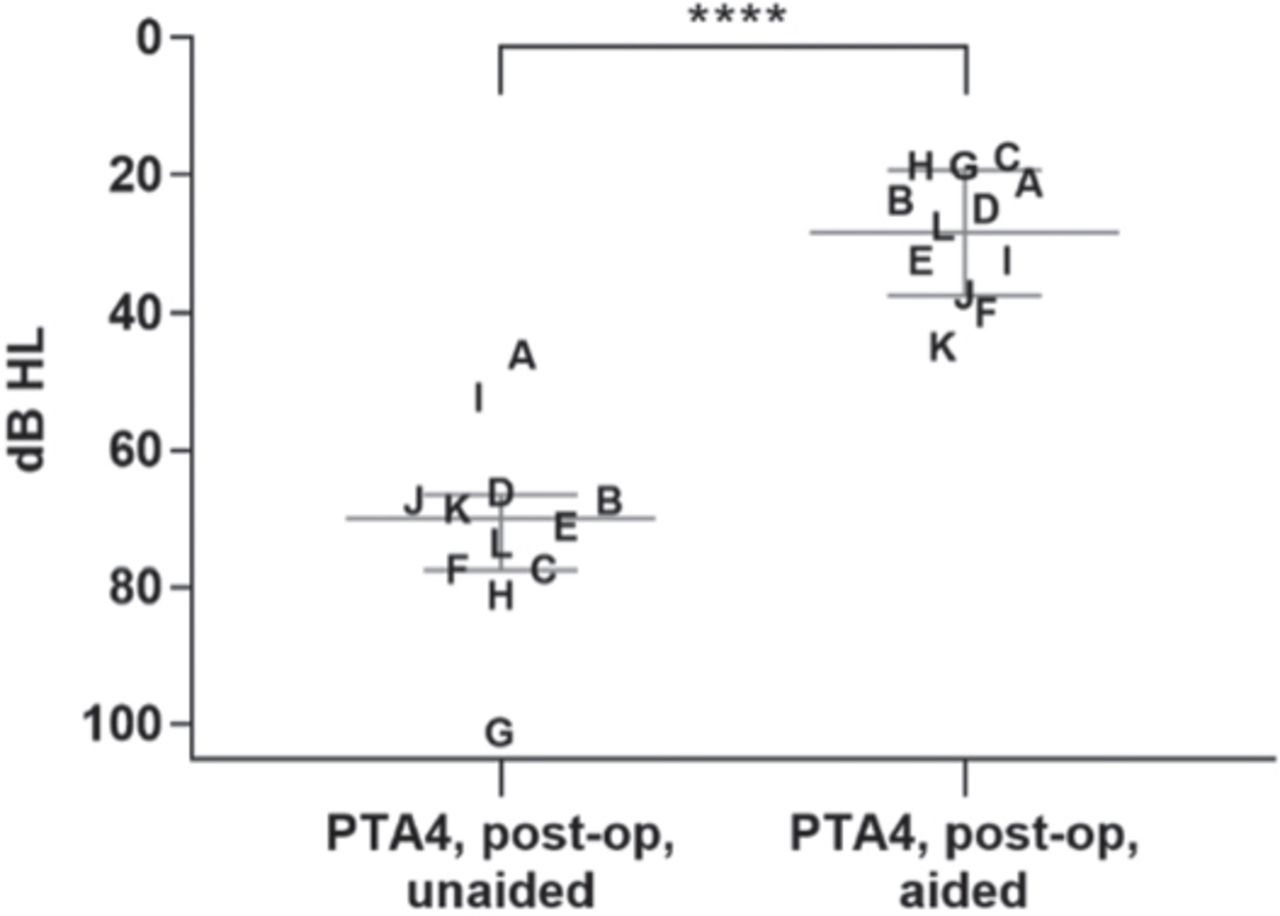
Across all frequencies, aided sound field (SF) thresholds were significantly improved by the BB. The mean aided PTA4SF was 29.8dB HL compared with the mean unaided PTA4SF of 74.6 dB HL. The average functional gain was 40±6.3dB HL (Figure 2).

A comparison of the post-operation (post-op) puretone average (PTA4) (0.5, 1, 2, and 4 kHz) unaided and aided with the Bonebridge implant. The scatter plot shows the individual data points where each letter represents a study participant and the median (long line) with the interquartile range (25th and 75th percentile, whiskers). The non-parametric Wilcoxon test was used to test for statistical significance (p=0.0001, n=12). AC - air conduction, HL - hearing level.
Speech audiometry
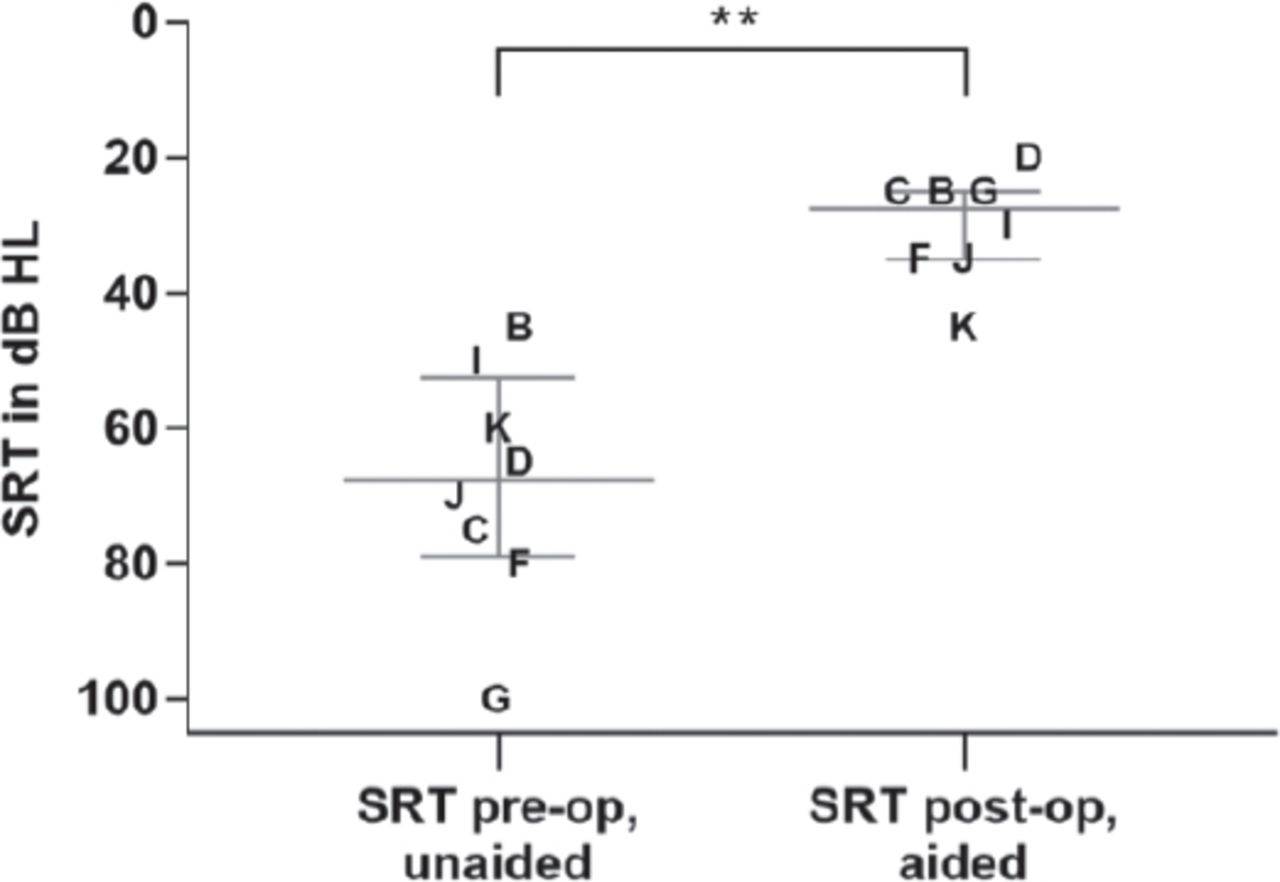
The hearing ability in a quiet environment also significantly improved. The SRT with BB was lower in all patients compared to the pre-operative SRT. The mean pre-operative SRT decreased from 67.8 dB HL (SD 18.5 dB HL) to 27.9 dB HL (SD 5.6 dB HL) (Figure 3).

A comparison of the pre-operation (pre-op) speech recognition threshold (SRT) in a quiet environment, unaided, with the aided values measured post-operatively (post-op). The speech material consisted of Arabic disyllabic words. The plot shows the individual data points where each letter represents a study participant and the median (long line) with the interquartile range (25th and 75th percentile, whiskers). The normal distributed t test was used to test for statistical significance (p=0.001, **p≤0.05, n=8).
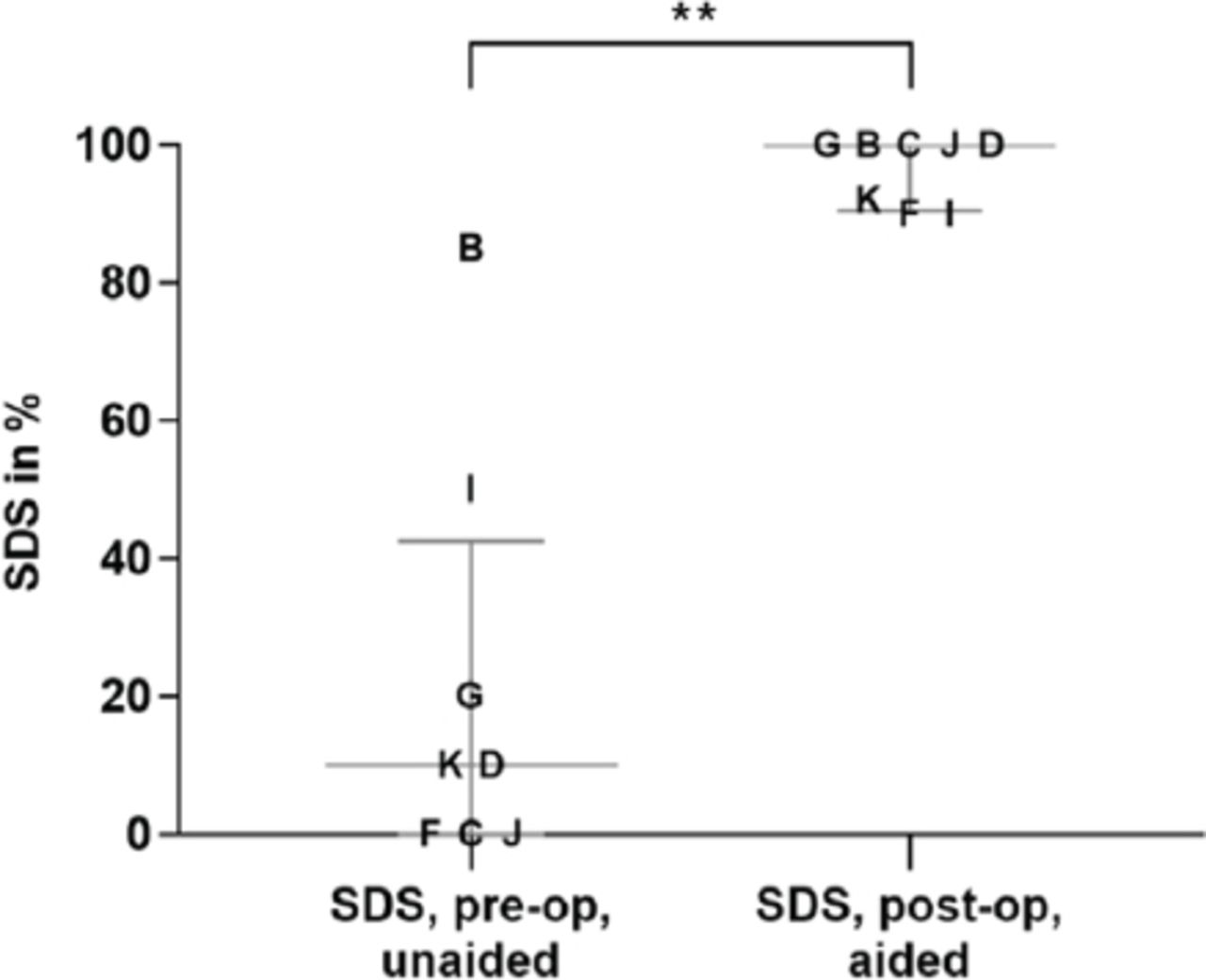
Before implantation of the BB, the mean SDS was 26.7% (SD 34%) in the unaided condition. One year after implantation, the mean SDS was 90-100% for monosyllables at 65 dB sound pressure level (SPL) (mean: 97.1%, SD 4.8%). The improvement in sound discrimination was statistically significant (p=0.0078) (Figure 4).

A comparison of the unaided pre-operation (pre-op) speech discrimination score (SDS) versus the post-operation (post-op) score aided with the Bonebridge. The SDS was measured at 40 dB sensation levels (SL) (65 dB hearing levels (HL), Arabic monosyllabic words). The plot shows the individual data points where each letter represents a study participant and the median (long line) with the interquartile range (25th and 75th percentile, whiskers). The median value of SDS pre-op was 10%, whereas this value was 100% for post-op. The nonparametric Wilcoxon test was used to test for statistical significance (p=0.0078, ** p≤0.05, n=8).
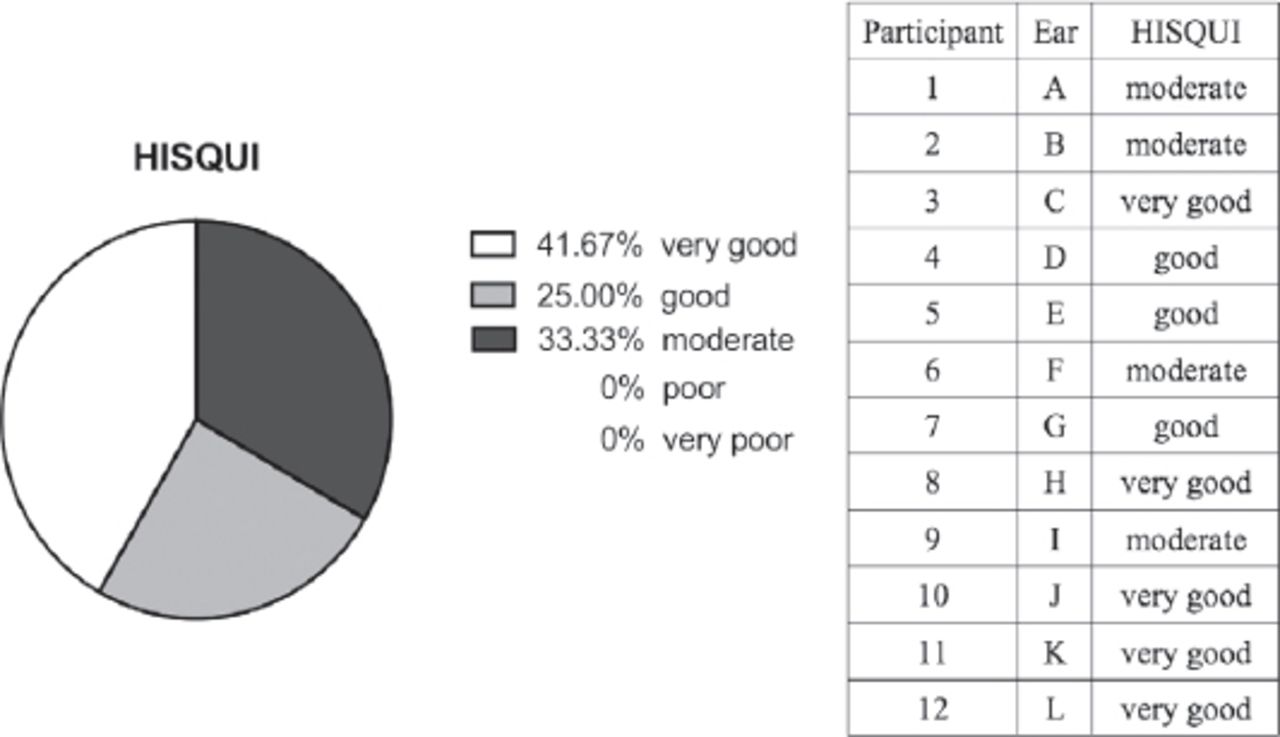
Hearing Implant Sound Quality Index (HISQUI)
The HISQUI questionnaire was used to evaluate the subjective sound quality of the BB. The total satisfaction of the participants regarding sound quality of the BB system was good. (Figure 5). Sixty-seven percent of the participants rated the improvement as good to very good.

The hearing implant sound quality index (HISQUI) questionnaire was used to evaluate the subjective sound quality of the Bonebridge (n=12).
Discussion
This study demonstrates the clinical and subjective benefit of the BB in patients with conductive or mixed hearing losses. In agreement with other recent reports,7-9 we demonstrated that the BB implant procedure can be considered safe; also, there are clinical and subjective improvements of the hearing threshold in its users. Audiological results showed an improved ABG as well as PTA4, SRT, and SDS values with the BB. Similar to other studies,7,10 the post-operative BC thresholds remained stable in all the patients implying that their residual hearing was unaffected by the surgical procedure.
The functional gain observed in this analysis (40±6.3dB) was slightly better than those reported by Ihler et al11 (33.6 ± 7.2 dB), Barbara et al12 (36.5 dB), Manrique et al,8 and Hassepass et al.5 Similarly, another study conducted in 20139 reported a mean functional gain of more than 20 dB across all frequencies (0.5, 1, 2, 4 kHz). However, Hougaard et al17 reported that the functional gain in conductive or mixed hearing loss patients by using BAHA attract was 19.8 dB, which is much lower than the improvement reported by using BB implant. Also, in our study, a significant improvement was observed in speech recognition in a quiet environment; the improvement was on par with those reported by other researchers that used German monosyllabic word lists11 and by those that used disyllabic word lists in Spanish.8 In a quiet environment, the efficacy of the BB found in the present study (97.1%, SD 4.8%) was in the same range reported by other studies. Schmerber et al2 reported a follow-up period of one year, similar to the present study, and their participants achieved a mean speech recognition score of 95% (SD 15%). Meanwhile, Sprinzl et al9 reported a mean monosyllabic word recognition score of 14.2% in pre-operative investigations that improved to 92.9% post-operatively. A similar improvement, 16.7% pre-operatively versus 80% post-operatively, was observed by Ihler et al.11 Manrique et al8 obtained a mean recognition score of 66.2% pre-operatively, improving to 86.2% post-operatively, using a disyllabic word list.
Percutaneous BC implants have been widely used in the treatment of hearing loss for a long time. However, the drawback of percutaneous implants is the risk of infection at the abutment. The intact skin above the BB implant decreases the rate of infection and places the BB in an advantageous position over the well-established percutaneous BC implants. Moreover, it will also help to reduce the stigmatization associated with implantation. Though the BB and the bone anchored hearing aid (BAHA), another hearing implant system,13 present comparable outcomes, the BB may be more appealing to patients.
Sprinzl et al9 demonstrated that BB implantation has a very low rate of minor adverse events (5.12%) and revision surgery (0.85%). In our study, after 2 years of BB use, no revision surgery and no skin reactions were reported, similar to short-term follow-up studies.2,5,8,9,11,14 Moreover, the BB has a much lower complication rate than the BAHA implant (24%) that is associated with a higher rate of revision surgery (12%).4 In the long-term follow-up (mean: 14 years) of BAHA use, the skin reaction rate (31%), loss of osseointegration (17%), and need for revision surgery (34%) have been reported.15 The relatively large size of BB implant necessitates a good preoperative radiological evaluation of temporal bone, to examine if the patient has adequate place which could accommodate the implant. Laske et al16 measured the subjective satisfaction of 9 patients after BB implantation with 2 questionnaires (a modified version of the Speech, Spatial, and Qualities of Hearing questionnaire [SSQ-B] and the Bern Benefit in Single-Sided Deafness Questionnaire [BBS]). Similar to their findings, the majority of our patients reported moderate improvements and 57% rated the improvement as good to very good.
Study limitation
The sample size was a major limitation of the present study.
In conclusions, patients with conductive or mixed hearing losses substantially benefit from the BB active transcutaneous BC hearing implant without minor or major complications.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 28, 2019.
- Accepted July 8, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.