


Abstract
Objectives: To systemically review the evidence concerning the prevalence and reported risk factors of smoking among adolescents in Saudi Arabia.
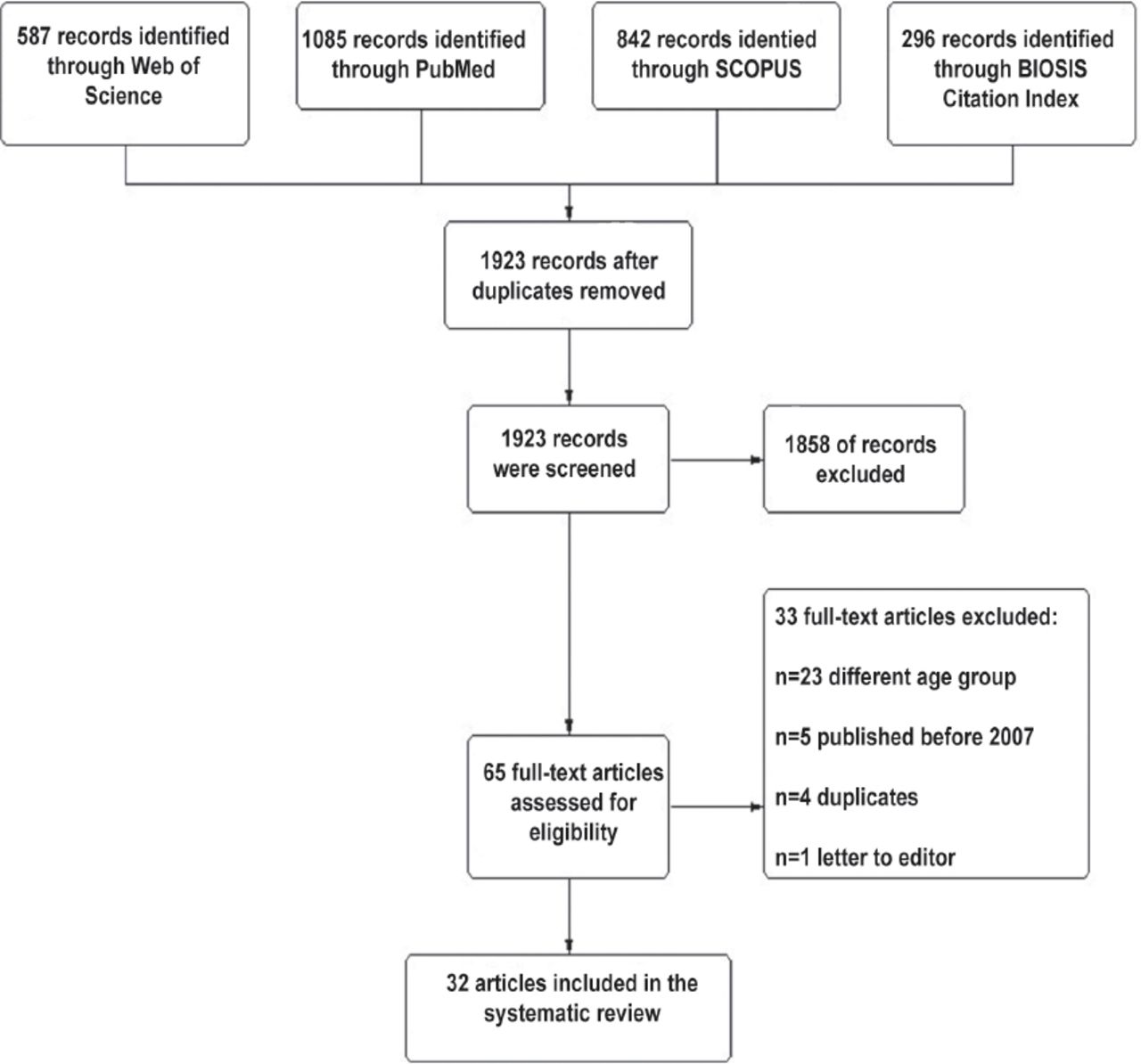
Methods: Following the PRISMA guidelines, studies that examined the prevalence and risk factors of smoking among adolescents in Saudi Arabia were identified through a computerized literature search using the following databases up to March 2018: PubMed, SCOPUS, Web of Science, and BIOSIS. The following search terms were used: smoking OR smok* OR tobacco OR cigar* OR shisha OR shesha OR sheesha AND Saudi Arabia OR KSA. Peer-reviewed articles published within the period from 2007 to 2018 were selected. Studies that reported prevalence data, patterns, and risk factors of smoking among adolescents were included. Extracted data from each study were tabulated, and data were narratively synthesized.
Results: Thirty-two studies that reported the prevalence of smoking in the adolescent age group were included in the narrative evidence synthesis. These studies were conducted on secondary school students (n=11), college students (n=14), and an adolescent age group without educational specifications (n=7). According to published reports between 2007 and 2018, the prevalence of tobacco smoking among adolescents in Saudi Arabia ranged from 2.4% to 39.6%. Influence of friends, and family negligence were the most commonly reported risk factors for smoking.
Conclusion: The prevalence of smoking is relatively high among adolescents in Saudi Arabia. The social influence of friends, teachers or parents, low academic performance, having spare time, living away from home, and the desire to relieve stress were the most commonly reported risk factors for smoking.
PROSPERO REG. NO: CRD: 42018108053
Smoking is the greatest preventable risk factor of illness and death. The number of smokers worldwide is approximately 1.3 billion, with more than 80% of smokers living in low- and middle-income countries.1 Recent reports showed a global decline in the prevalence of smokers between 1980 and 2012, mostly noticed in some north American and Scandinavian countries. However, the prevalence of smoking over the same period has risen dramatically in developing countries such as Cote d’Ivoire, Kazakhstan, Serbia, and Mauritania and in high-income countries including Croatia and Saudi Arabia.2 Recent estimates demonstrate that approximately 20% of Saudi Arabia citizens are tobacco smokers and similar rates have been reported among adolescents.3,4 According to the World Health Organization (WHO), the prevalence of smoking among adolescents in Saudi Arabia in 2016 was 21.2% among males and 9.1% among females. The smoking prevalence among Saudi adults was 23.7% for males and 1.5% for females.5 It is worth pointing out that smoking was more prevalent in female adolescents compared with adult females. Unfortunately, the WHO statistical trends show that the rate of smokers increased gradually among Saudi adolescents from 12.45% in 2000 to 15.1% in 2010. If tobacco control in Saudi Arabia remains at the same intensity, WHO estimates that by 2025 38% of males and 2% of females aged 15-24 years will be smokers.6 Smoking behavior often starts during the adolescence, and those who start smoking early in adolescence are less likely to quit smoking.7 It is also estimated that approximately 90% of new smokers are younger than 18 years of age, highlighting the importance of commencing efforts to prevent or control smoking in the adolescent population.8 Family history, companionship, personal character, and psychological problems are common risk factors for the commencement of smoking among adolescents. A WHO-collaborative study including students from 35 countries in North America and Europe found that youths from low-income families and those who have a poor relationship with their parents and other family members were more likely to be smokers.9
The aim of this review was to establish the evidence related to the prevalence of smoking and reported risk factors among adolescents in Saudi Arabia.
Methods
The systematic review presented was conducted per the standards set out in PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) (Table 1) and MOOSE (Meta-analysis of Observational Studies in Epidemiology) statement guidelines.10,11 The review was additionally conducted per the Cochrane Handbook of Systematic Review and Meta-analysis.12 It included articles that were published in peer-reviewed journals between 2007 and 2018. All included articles reported prevalence and risk factors of smoking among adolescents in Saudi Arabia.
The summary of included studies.
Literature search strategy
PubMed, SCOPUS, Web of Science, and BIOSIS were searched through to March 2018 using a combination of the following keywords as well as MESH keywords: smoking OR smok* OR tobacco OR cigar* OR shisha OR shesha OR sheesha AND Saudi Arabia.
Study selection
The first author and a research assistant independently screened the literature search results for relevant studies. The screening for included studies was performed in 2 steps; the first step was screening based on titles and abstracts of the retrieved records, and the second step was based on screening of full-text articles. Discussion with a third reviewer resolved any disagreement between review authors.
Eligibility criteria
Studies that met the following criteria were included in this review: 1) studies whose population was Saudi Arabian adolescents, 2) studies evaluating the prevalence or risk factors of smoking tobacco products among the Saudi Arabian adolescent population.
Data extraction
The final included papers were extracted independently by 3 reviewers. The extracted data include 1) characteristics of the study design of included studies, 2) characteristics of the study population, and 3) data related to the study outcomes including prevalence and risk factors of smoking.
Quality assessment
The Newcastle-Ottawa scale for risk of bias assessment among cross-sectional studies was employed. It consisted of 7 domains including sampling, statistical measures, and outcomes. Three independent authors assessed the quality of included studies and any discrepancies were resolved through discussion.
Synthesis of results
Included studies were classified according to the type of the population into: 1) studies on intermediate and secondary school students, 2) studies on college students, and 3) studies on an adolescent age group from various educational levels. Extracted data from each study were tabulated and data were reviewed narratively. Microsoft Excel was utilized to provide simple descriptive statistics of numbers and proportions whenever needed.
Results
Characteristics of included studies
The search resulted in the retrieval of 32 unique studies published between 2007 and 2018 that met the inclusion criteria. These studies were undertaken in the following cities in Saudi Arabia: Riyadh (n=12), Western Region (n=5), nationwide multicenter (n=4), Madinah city (n=3), Al-Hassa (n=2), Eastern Region (n=3), Jazan Region (n=1), Northern Region (n=1), Tabuk (n=1). The study selection process is shown in Figure 1. The summary of included studies is shown in Table 1.

The PRISMA flow diagram of the study selection process.
Quality of included studies
All studies rated as good quality with a total score of 7 to 8 stars. All articles showed stars regarding representativeness of the sample, satisfactory recruitment rate, validated measurement tool and clear statistical analysis. Self-report was granted a star since all studies were based on survey design.
Prevalence of smoking among secondary school students
Eleven studies investigated the prevalence of smokers among secondary school students in Saudi Arabia. Their prevalence estimate ranged from 9.72% to 37%. The highest prevalence of 37% was reported in a study that included 695 high school boys in Jeddah,19 followed by 33% in a 2010 study included 1272 high school students in Riyadh,13 followed by 28.6% in another study of 225 students in Riyadh.21 The lowest prevalence of 9.72% was reported in a study of 1019 students in 2010 in Jeddah,26 followed by 10.7% in a study conducted in 2011 in Jazan region with 3923 students.24
Three studies reported the prevalence of secondary school students who had ever smoked. The prevalence of students who had ever smoked was 17.3% in Riyadh 2010, 25.4% in Al-Hassa 2009, and 42.8% in Madinah 2013. Al Moamary et al13 estimated prevalence of water-pipe smoking at 10.2% (8.6% in males, 1.6% in females), while they reported that 33% (65.9% in males versus 34.1% in females) had ever smoked. On the other hand, Amin et al15 reported waterpipe smoking at a rate of 53.9%. Fida et al20 found that the majority of students (83.7%) started smoking at the age of 14 years or less. In other studies, Al Moamary et al13 reported that 68.1% initiated waterpipe smoking from the age of 11 years, and Al Nohair21 reported that the majority (89%) of adolescent smokers began to smoke before the age of 15 years. Even more alarming is the study by Al Ghobain et al18 who reported that 13.5% of adolescents reported using tobacco for the first time before the age of 10 years.
Prevalence of smoking among college students
From 14 college studies, the findings showed that the smoking prevalence ranged from 2.7% to 8.5% among females and 13% to 30.9% among males. The highest prevalence of college students was 30.9% in a study that included 337 male college students,30 followed by 29.8% in a study that included 715 male college students,35 and 25% among a cohort of 336 dental students.31 The lowest prevalence rate reported was 2.4% in a study of female medical students,33 followed by 8.6% among female students who joined other schools in Dammam, Saudi Arabia,39 and 11.1% in a study that included 910 medical students in Riyadh.37 Al-Mohamed and Amin reported that at the time of their survey waterpipe smoking was 14.6% in a total of 1382 students in Al-Hassa at King Faisal University.29
Knowledge and attitudes of smoking among adolescents
A study by Al-Bedah et al27 surveyed 825 students in health schools from different regions in Saudi Arabia and revealed that 65% to 85.6% of the participants knew the hazards of tobacco use/smoking, while only 35.3% to 40.5% knew about tobacco-related diseases. The study reported that 84.5% to 97.1% of health professional students agreed with banning smoking in restaurants, 87.1% to 100% to enforcing the banning of smoking in enclosed public places, 87.1% to 100% recommended banning smoking in cafes, 82.6% to 94.1% agreed with the banning of smoking advertisements, and 81.1% to 94.1% agreed with the prohibition of selling tobacco to adolescents. A 2017 study by Mansour31 included 420 dental students and reported good awareness of the commonly risks of second-hand smoke; however, students were less aware of the risks of shortening life span. Al Moamary et al13 in his study of 1272 high school students, reported that 86.4% of the participants perceived that smoking was harmful. The study also reported that 79.6% of the participants supported banning waterpipe smoking. In addition, 59% of the smokers were willing to quit waterpipe smoking, and 48% of the smokers reported that they had tried to quit smoking. High awareness about smoking hazards was also reported in the studies by Amin et al,15 Ansari and Farooqi,28 Almutairi,34 Baig et al,36 and Algorinnees et al.44
Smoking prevalence in Saudi Arabian cities
Regarding the geographical distribution, studies about the prevalence of smoking among adolescent age groups in Saudi Arabia were not consistent. However, all reports showed a relatively high prevalence rate of smoking, highlighting the need for public health interventions and educational campaigns to reduce the number of new and existing smokers in the adolescent age group. The highest prevalence rate of smoking among adolescents was found in Jeddah and Riyadh. The summary of prevalence rates according to the study setting (cities and geographical locations) are shown in Table 1.
Smoking prevalence among adolescents by gender
Smoking prevalence rates among boys were greater than girls in all the included studies regardless of their age or educational levels. A study with a total of 1272 participants reported a smoking prevalence of 31.2% for males versus 8.9% for females in Riyadh city, Saudi Arabia from April to June 2010.18 Another study reported that 30.3% of males, but only 8.5% of females smoked waterpipe.13 A significant difference between males and females was also found in another study (12.43% for males and 6.65% for females).26 Males smoke 2 to 6.4 times more than females. For shisha smoking, this was 1.2% to 5.7%.27 Gaffar et al24 reported that 16.2% of males and 3.8% of females were smokers. A recent study reported substantially higher rates of smoking among males than females in secondary schools (26.2% versus 7.9%), and among males than females in intermediate schools (17.1% versus 8.8%).23 In Tabuk region, 34% of boys and 11.1% of girls in secondary school were smokers.41 Al Moamary et al13 reported 8.6% male waterpipe smokers versus 1.6% female waterpipe smokers.
Risk factors of smoking among adolescents
The included studies illustrated a number of risk factors for smoking among adolescents in Saudi Arabia. Smoking friends and/or families were the most commonly reported risk factors.18-20,23,29 Amin et al15 reported that outings with friends, company of friends, boredom, and spare time were the motives for waterpipe smoking. Having spare time (81.6%), stress relief (63.2%), and watching smoking teachers (61.8%) were the most common risk factors associated with smokers as reported by Al Nohair et al.21 Being from high income families, receiving high daily allowances, studying less, skipping class, describing themselves as less religious and not being involved in religious activities, being males, and spending more time away from home were the most common associated risk factors of smoking according to Al Agili 2012.26 Al-Mohamed and Amin reported that the most common predictors of smoking were living outside home as well as having a family member or a friend who smoked.29 Al Zalabani and Kasim23 showed that smoking parents, understanding of smoking-related hazards, mass media, and pocket money were other important factors in predicting smoking among adolescents in Madinah, Saudi Arabia.
Discussion
The prevalence of smoking among adolescents in KSA varied immensely in different studies, ranging from 9.72% to 37% among secondary school students, 2.4% to 30.9% among college students, and 12.7% to 39.6% among adolescents age group regardless of their educational stages. In all studies, prevalence was reported to be significantly higher in males than in females. The prevalence of smoking ranged from 8.6% to 37% in male adolescents and 1.6% to 11.1% in female adolescents. A possible reason for Arab males having higher smoking rates may be because they spend free time with their peers without the restrictions and supervision females experience. Additionally, males believe that smoking could help increase the masculine image and the maturity perception among peers.23-26 In contrast, social stigma may be responsible for the low smoking prevalence among females. Additionally, females believe that smoking could affect their feminine Islamic image and reputation, thus affecting marriage chances.48 In addition, it is thought that the cultural censure of smoking among females may also contribute to the low prevalence.
Our findings also showed that waterpipe smoking prevalence ranged from 10.2% to 53.9%. The prevalence of those who had ever smoked ranged from 17.3% to 42.8%. There are variations in the prevalence of smoking in terms of year of research and location of residency (Table 1).
Addressing factors associated with smoking is a critical approach to reducing the prevalence of smoking and improving the health of a nation. The included studies reported several predictors of smoking in Saudi Arabia. Imitating friends and family negligence represented the most common risk factors for smoking.49 Saudi Arabia is currently undergoing a rapid phase of modernization in which socialising out of the home environment is growing. Adolescents expressed their adulthood through spending more time with their peers out of the home, particularly in the hastily growing cafes/restaurants, thus, increasing smoking prevalence among adolescents.14 Other risk factors have been reported, such as older age,29,49 male gender,16,18 parental smoking,29 friends smoking,20,24 socioeconomic status,24 perception of health hazards of smoking,49 and single parent.24 A study reported a strong association between khat chewing which is a natural stimulant on the central nervous system, extracted from the Catha edulis plant and tobacco smoking.24 However, there are reductions to the risk of smoking by educated parents; approximately by 51% among fathers and 39% among mothers.23 Religious beliefs are negatively associated with smoking attitudes and could be a strong predictor of the intention not to smoke.50
Religious values have a paramount effect in helping adolescents quit smoking. A study reported lower smoking prevalence in Islamic secondary school than in other schools.51 Furthermore, Al-Mohrej et al53 reported that the majority of ex-smokers (57%) had decided to quit because of religious and social reasons. Also, Health was another reason for 40% of the quitters, while only 3% stopped due to financial constraints.
Encouraging parents to abstain from smoking, advising students to avoid any gathering that includes smoking, and controlling the use of cigarettes among the young may be an effective strategy to reduce the prevalence/uptake of smoking. Broadening the knowledge of smoking-related hazards through enhancing the scholastic curriculum, mainly from the first year of school life, life, has proved to be one of the effective approaches. The media have a role in increasing the awareness of students and their families about the dangers of smoking. Ansari et al28 reported that approximately 70% of smokers quit smoking because they had greater knowledge and information on smoking hazards. These findings are in agreement with the results of a previous study in King Faisal University with a total of 12400 students included (males=8200, females= 4200) in the academic year 2006 to 2007.29
Primary and secondary prevention programs have a vital role in reducing smoking among adolescents in Saudi Arabia. School-based tobacco control programs that pay particular attention at the sociocultural context of smoking habit, consider the associated risk and protective factors, and reflect the differences between male and female gender are useful methods in reducing the onset of smoking among students.54,55 Anti-smoking clinics should be established to provide pharmacological and non-pharmacological treatments for smokers. Treatment of nicotine dependence and tobacco-related diseases should also be reinforced. Other interventions, including implementing strict rules regarding cigarette sales to minors under 18 years, prohibiting smoking on health and educational premises and on public transport, banning smoking advertising in the media, and raising taxes and the cost of tobacco products, could be used to reduce the uptake and prevalence of smoking.23,28 Moreover, a systematic review assessed adolescent smoking prevention programs and confirmed the need for new school-based programs to reduce the prevalence of smoking. These programs should target risky populations, depend on qualified health professionals, and use updated methods to achieve widespread success.57
Our findings are consistent with the results of a 2014 systematic literature review exploring the prevalence of smoking among Saudi students which was published in 2014 with 12 relevant studies published until October 2013. In that review, the prevalence of smoking among adolescents ranged from 10% to 30%.58 The literature also suggests that males smoke more than women.59 Likewise, the current study accords with a 2013 report of the WHO which reported that the prevalence of tobacco smoking was 25.2% among males and 1.9% among females in Saudi Arabia.5
In its 2011 report regarding smoking prevalence in the Middle East and North Africa, the WHO announced that the lowest smoking prevalence was found in Morocco (15.1%), whilst the highest prevalence was found in Lebanon (38.5%). Among males, the lowest smoking prevalence was reported in Saudi Arabia (20.2%) while the highest was found among the Syrians (62%). Among females, it varied from 0.2% among Moroccans to 31.5% among Lebanese.60 Our results are in agreement with the results of western studies. In 2015, the proportion of smokers in the UK was 23.1%, while in the United States it was 22.3% among adults.5 A systematic review of 59 studies published up to 2011 reported that the tobacco use ranged from 2.4% to 22% among Brazilian adolescents.61
This study has been limited by the lack of quantitative meta-analysis. The authors also included articles published between 2007 and 2018 which may introduce selection bias and affect the overall inferences. Nevertheless, our results have implications for the promotion of interventions to reduce tobacco use. These interventions should include approaches to progress school cohesion and involve family members as role models. Our findings can also be used to inspire authorities in the education sector to implement suitable actions to resolve the problems related to smoking and encourage religious education. It is highly recommended that further and detailed studies of smoking prevalence be conducted at regular intervals to help in guiding policy changes and interventions to reduce the prevalence of smoking.
Multicenter future studies are recommended to investigate the variation in smoking prevalence among various regions of Saudi Arabia.
In conclusion, this review highlights that the prevalence of smoking is relatively high among adolescents in Saudi Arabia ranging from 9.7% to 37% among secondary school students, 2.4% to 30.9% among college students, and 12.7% to 39.6% among adolescents age group without educational specifications. The social influence of friends, teachers or parents, low academic performance, having spare time, living away from home, and the desire to relieve stress were the most commonly reported risk factors for smoking. It is noteworthy that strong religious beliefs could reduce the risk of tobacco use. Further public health interventions are needed to increase the awareness of adolescents of the dangers and consequences of smoking, and thereby help them to quit smoking. Future healthcare policies should consider the variable definitions and wide-ranging estimates of smoking among different populations and regions reported in the published literature.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 18, 2019.
- Accepted August 8, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.