


Clinical Presentation
An 84-year-old female presented with a 2-day history of abdominal pain, vomiting, and constipation/obstipation. She had a prior history of abdomino-perineal resection for carcinoma of rectum 15 years ago. On examination, the abdomen was distended with increased bowel sounds. There was increased tenderness in the medial aspect of the thigh, no palpable inguinal mass, or any evidence of hernia. Clinical diagnosis of bowel obstruction, likely secondary to recurrence of carcinoma rectum or from adhesions due to prior surgery was considered. Further evaluation with plain radiograph and CT scan was requested to determine the cause of small bowel obstruction.
Questions
What is the likely diagnosis?
What are the findings on abdominal radiograph and CT scan?
What is the management?
Answers
Small obstruction due to right obturator hernia.
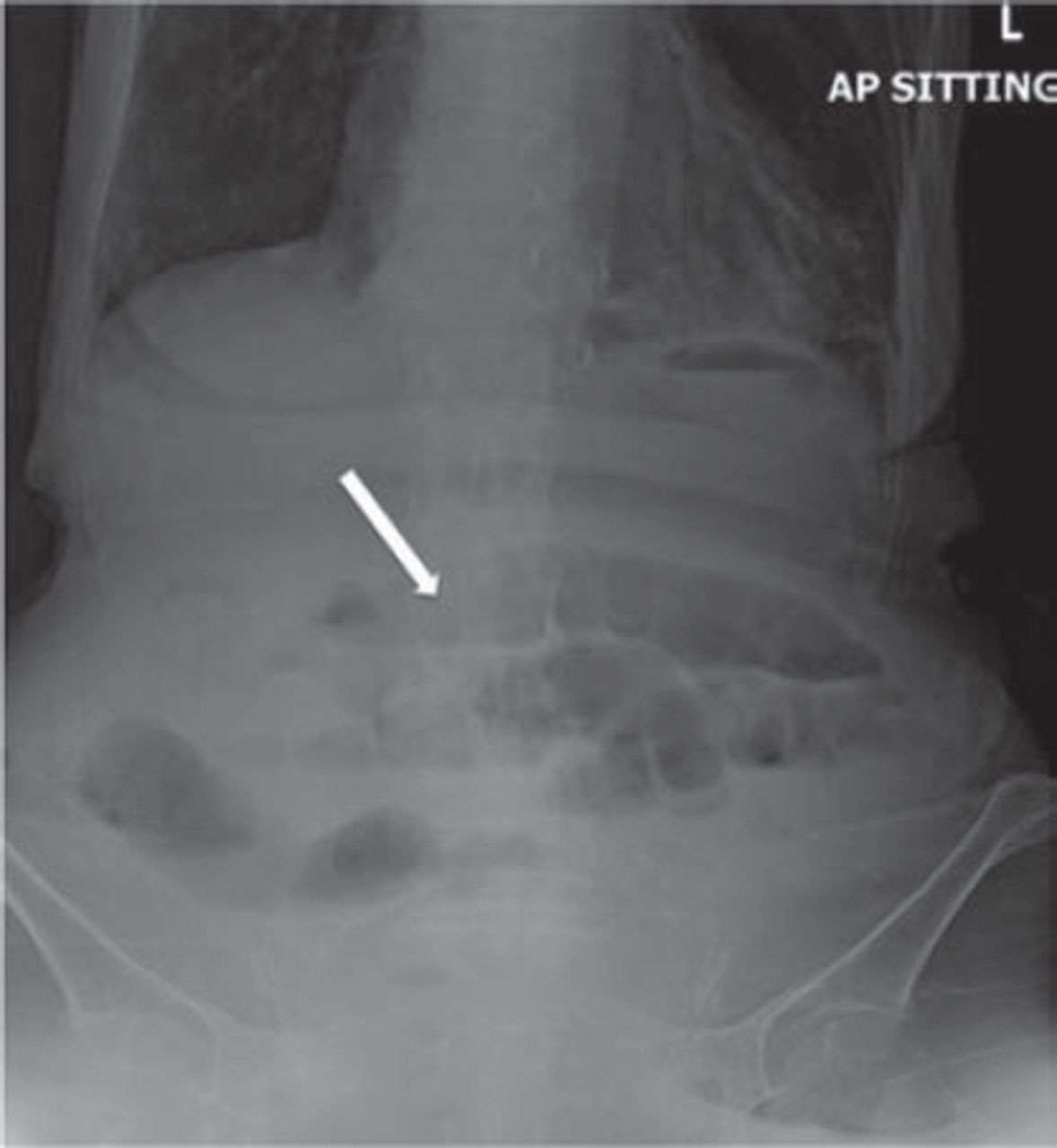
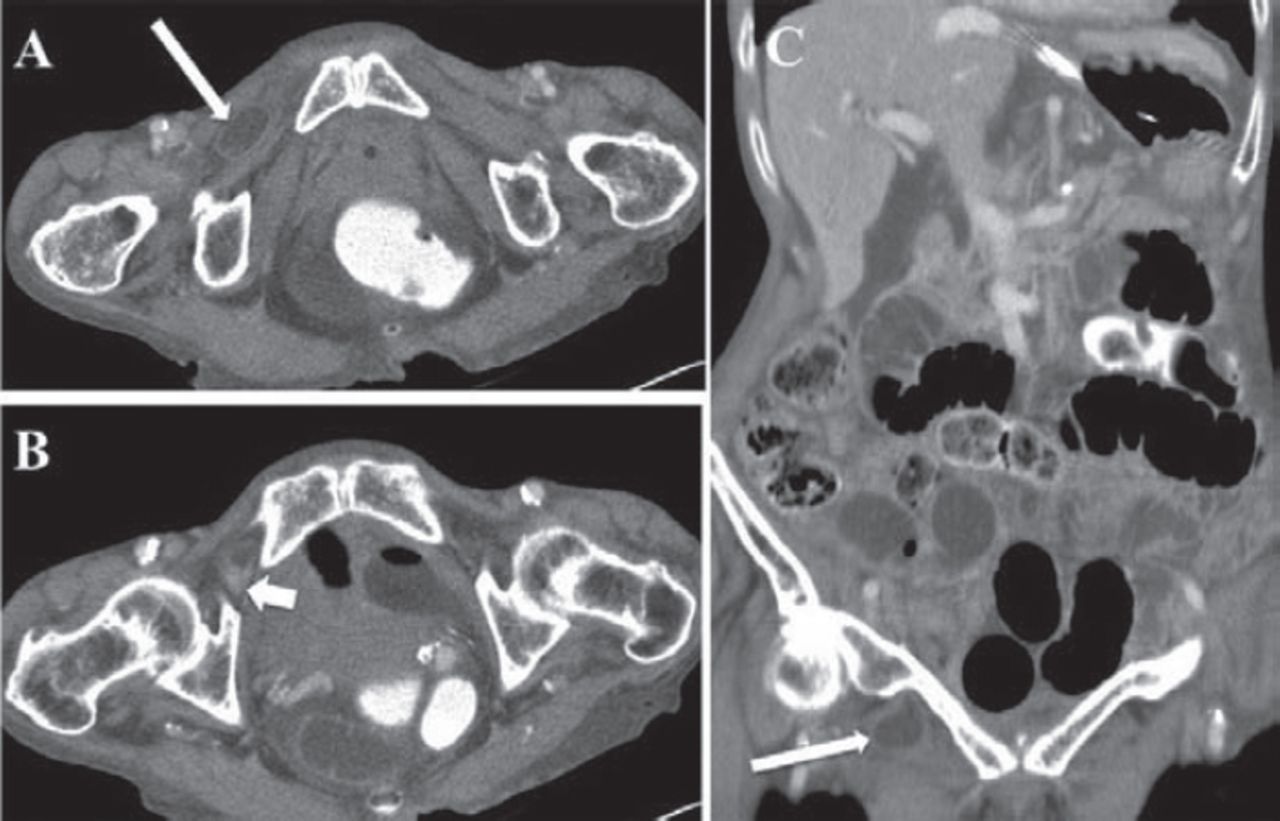
The radiograph of abdomen in sitting anteroposterior (AP) position showed air-fluid levels suggestive of small bowel obstruction (Figure 1). The intravenous contrast enhanced CT scan of the abdomen (Figure 2) demonstrated a distal ileal bowel loop between the right pectineus and obturator externus muscle in the region of obturator canal with transition point, suggestive of small obstruction due to obturator hernia. No CT evidence of small bowel incarceration was present.
Figure 1Plain radiograph of abdomen in sitting AP position. There is suggestion of air-fluid levels suggestive of bowel obstruction (arrow).
Figure 2Intravenous contrast enhanced A) axial and B) coronal and C) CT scan of the abdomen. The CT scan shows a small ileal bowel loop between the right pectineus and obturator externus muscle in the region of obturator canal (long arrow) suggestive of obturator hernia. The transition point (short arrow) of the small bowel obstruction was in the region of obturator foramen containing ileal loop
Emergency open laparotomy was performed that revealed a dilated small bowel with an obvious transition point at the distal ileum caught within the right obturator canal. The small bowel was viable and reduced from the hernia sac. The hernial defect was subsequently closed by sutures.


Discussion
An obturator hernia is a rare intra-abdominal hernia representing around 1% of all hernias, and 1.6% of small bowel obstructions.1 According to Bjork et al,2 the incidence was approximately 0.1% of all hernias repaired at the Mayo Clinic. They have the highest mortality rate of all abdominal wall hernias at between 13-40%. They are more common on the right side, approximately 3 times more than the left due to sigmoid colon overlying the obturator foramen on the left side. The obturator foramen is one of the strongest foramen in the body. It is most commonly seen in elderly women known as “Little old ladies hernia” (female:male ratio was 6:1). It occurs in multiparous, frail, and older women who have wider pelvis and large obturator canal diameter. Other risk factors include chronic constipation, ascites, chronic obstructive pulmonary disease, and sudden weight loss with a decrease in the amount of fat around the foramen.3 The obturator canal is a 2-3cm long tunnel, which begins in the pelvis and ends at the obturator foramen bounded superiorly and laterally by the pubic bone, and inferiorly by the obturator membrane and muscles. It is a fat filled canal containing the obturator nerve, artery, and vein. The clinical diagnosis of obturator hernia is very difficult. The hernia is not easily visible on inspection or clinically palpable. The bowel loop with the obturator canal can compress the nerve resulting in pain and tenderness along the medial thigh. Approximately 15-50% of patients may show positive Howship-Romberg sign, which represents ipsilateral medial thigh pain increased by adduction of the hip. This is due to compression of the obturator nerve within the hernial sac.4 The most common content of the obturator hernial sac is the ileum with most belonging to Richter’s type. There are 3 types of obturator hernias, between the pectineus and obturator externus muscles, which is the most common (as seen in our case), hernia between the superior and middle fasciculi of obturator externus muscle, and hernia between the external and internal obturator membranes.
The obturator hernia is definitely diagnosed on CT scan, which demonstrates the bowel loop within the obturator canal. Narrowing of the bowel segments at the hernial orifice identifies the transition point on CT scan. Signs of strangulation including intramural air, fluid within the hernial sac, lack of bowel wall enhancement are easily identified on CT, which prompts early surgical intervention. Uncomplicated hernias without signs of incarceration can be treated with minimally invasive laparoscopy assisted repair while exploratory laparotomy is indicated in complicated hernias. It can be repaired either by closing the defect by mesh, sutures, and patch or reducing the hernia without closing the defect. However, it is currently recommended to close the defect.5
Emergency physicians and surgeons should be aware of this rare condition, as a delay in diagnosis and surgical treatment will increase morbidity and mortality in elderly patients. Although clinically occult, radiological diagnosis by CT scan is relatively easy. Complications including incarceration are identified on CT, helping in surgical planning.
Student Corner
We invite students from a variety of medical disciplines to submit original contributions based on their supervised research.
The Student Corner of Saudi Med J aims to help students explore research opportunities and network with other peers and mentors in the same field.
Submission Guidelines
Submitted Abstracts should include the following:
Title should be descriptive
Author’s names and affiliation(specify college level/year, academic degree of Senior Author)
Abstract must be structured and not more than 300 words
The following are the typical headings:
Objectives (background, why the study was done, specific aims)
Methods (setting, date of study, design, subjects, intervention and analysis)
Results (findings, data and statistical tests) and
Conclusion (general interpretation of results)
General Information on Abstract Submission
Submitted Abstracts should be co-authored by a Senior Supervisor
Abstracts will be reviewed by Student’s Corner Section Editor
There is no fee to submit an Abstract
Ethical Approval should be provided
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42846.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.