


Abstract
Objectives: To evaluate continuous positive airway pressure (CPAP) compliance and define predictors of CPAP compliance among Saudi patients with obstructive sleep apnea (OSA) after applying an educational program.
Methods: This prospective cohort study included consecutive patients diagnosed to have OSA based on polysomnography between January 2012 and January 2014 in King Saud University, Riyadh, Kingdom of Saudi Arabia. All patients had educational sessions on OSA and CPAP therapy before sleep study, and formal hands-on training on CPAP machines on day one, day 7, and day 14 after diagnosis. The follow-up in the clinic was carried out at one, 4, and 10 months after initiating CPAP therapy. Continuous positive airway pressure compliance was assessed objectively. Logistic regression model was used to assess the predictors of CPAP adherence.
Results: The study comprised 156 patients with a mean age of 51.9±12.1 years, body mass index of 38.4±10.6 kg/m2, and apnea hypopnea index of 63.7±39.3 events/hour. All patients were using CPAP at month one, 89.7% at month 4, and 83% at month 10. The persistence of CPAP-related side effects and comorbid bronchial asthma remained as independent predictors of CPAP compliance at the end of the study.
Conclusion: With intensive education, support, and close monitoring, more than 80% of Saudi patients with OSA continued to use CPAP after 10 months of initiating CPAP therapy.
Continuous positive airway pressure (CPAP) is a standard, safe, and efficacious treatment for obstructive sleep apnea (OSA), a common disorder with established harm to quality of life and adverse consequences for cardiovascular health.1 Obstructive sleep apnea is characterized by recurrent partial (hypopnea) or complete (apnea) upper airway obstruction during sleep. These recurrent respiratory events usually cause intermittent hypoxemia and sleep fragmentation.2 Recent data demonstrated that the estimated prevalence of moderate to severe OSA ranges from 10-17% in middle-aged and elderly men.3 In Saudi Arabia, 3 out of 10 middle-aged Saudi men and 4 out of 10 middle-aged Saudi women are at high risk of having OSA.4,5 The mainstay medical treatment for OSA is CPAP therapy.6 Among various available therapeutic modalities for OSA, CPAP remains the most effective treatment.6 Continuous positive airway pressure is a machine that applies positive airway pressure to the upper air passages via a mask fitted on the mouth or nose to keep the throat open.6 Previous studies in Western countries showed that OSA patients on CPAP therapy use their machines on average from 4.5 to 5.5 hours per night with compliance rates ranging from 30-85%.7,8 Several studies have been conducted to define factors that influence, or predict CPAP use and adherence, and reported conflicting results.6 Moreover, several studies reported that race might influence CPAP adherence. For example, available data suggest lower CPAP adherence among African Americans than Caucasians.9 An earlier study that assessed CPAP compliance subjectively (self-reports) among Saudi patients with OSA after 3 months of initiation of CPAP therapy revealed an overall compliance rate of 39%.10 However, self-reports have been shown to overestimate CPAP use by approximately one hour/night when compared with objectively measured CPAP use.11 In general, there are very few data on objectively assessed long-term CPAP compliance in the literature. Moreover, there is a lack of previous study objectively addressing the rate of CPAP compliance, the predictors of good compliance, and the side effects of CPAP treatment in Saudi OSA patients. Therefore, we established in our center an educational program for patients with OSA and easily accessible medical support, and close follow-up of CPAP compliance. This study was conducted to evaluate CPAP compliance and to define predictors of CPAP compliance among Saudi patients with OSA after applying the new educational program.
Methods
Subjects
This prospective cohort study included consecutive patients (age >18 years) (range 21-83 years) who were diagnosed in the University Sleep Disorders Center (USDC) at King Saud University, Riyadh, Kingdom of Saudi Arabia to have OSA based on polysomnography (PSG) during a 2-year period (January 2012 to January 2014), and agreed to participate in the study. Prior to the sleep study, the patients were assessed by a sleep physician, where detailed history and physical exam were performed including demographic data, comorbidities (by history and from patients’ files), and medications. Exclusion criteria included patients with daytime hypercapnia (PaCO2 >45 mm Hg), congestive heart failure, neuromuscular diseases, and patients on home oxygen therapy. None of the studied patients was diagnosed to have OSA or used CPAP prior to the USDC visit. Additionally, none of the participants was on sedatives or drinks alcohol. Daytime sleepiness was assessed using the Epworth sleepiness scale (ESS), which is a validated accepted sleep questionnaire containing 8 items that assess the likelihood of dozing in a variety of daily living situations.12 The study was approved by the ethics committee in the College of Medicine, King Saud University and an informed consent was obtained from participants.
Study protocol
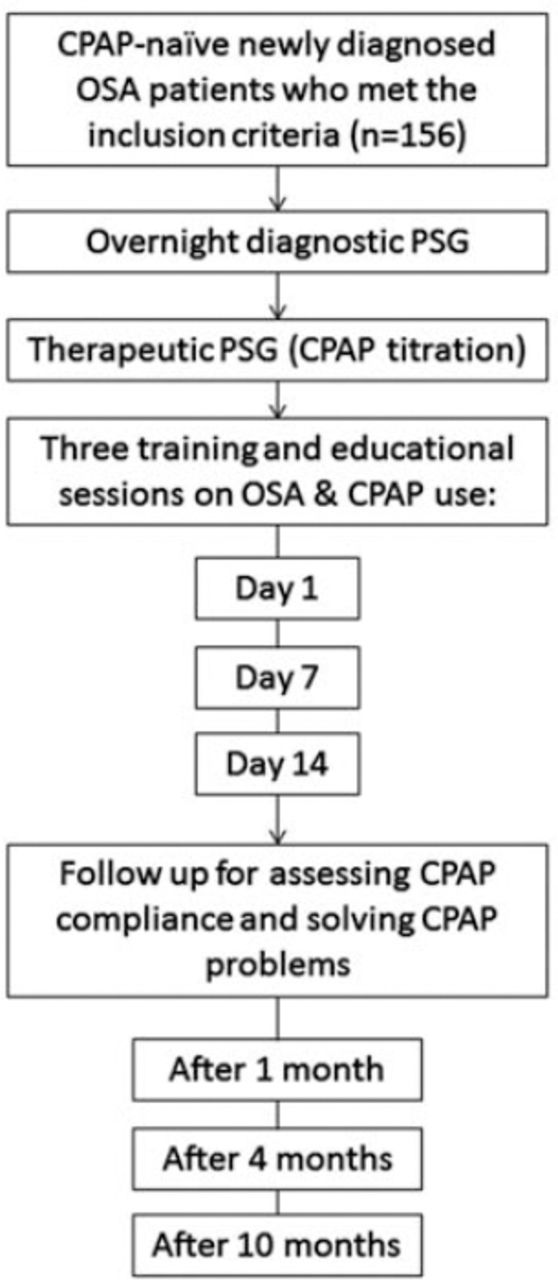
Figure 1 summarizes the study protocol. Patients underwent 2 level I attended in-lab sleep studies as described below. The first night was a diagnostic night and the second night was a therapeutic night where CPAP titration was performed.

Study protocol of patients who underwent 2 level I in-lab sleep studies. CPAP - ontinuous positive airway pressure, OSA - obstructive sleep apnea, PSG - polysomnography
Educational and training program
All patients received information by a health educationalist regarding the overnight sleep study and CPAP titration when they were given the appointment for sleep study. Selection of the best mask was carried out before starting the therapeutic study. After diagnosis, patients met a sleep physician who discussed the sleep study results, OSA complications and beneficial effects, and potential side effects of CPAP therapy. Then an educationalist explained how the CPAP works and its components. All patients received written educational material (in Arabic) on OSA and CPAP therapy. The educational points were reviewed with patients during subsequent treatment and follow-up visits by an educationalist and a sleep technologist. In the first 2 weeks after the therapeutic sleep study, the patient underwent 3 hands-on educational (training) sessions on operating the CPAP machines, on mask application and removal, humidifier, filters, and cleaning of the machine: 1)Session 1: on the day they received CPAP; 2) Session 2: after one week of using CPAP; 3) Session 3: after 2 weeks of using CPAP.
Polysomnography
Standard PSG recording was performed recording electroencephalogram (C3A2, C4A1, O1A2, O2A1, F3A2, F4A1); electro-oculogram; muscle tone (electromyogram of the chin and both legs); chest and abdominal wall movements (thoracic and abdominal belts); continuous finger pulse oximeter; airflow (thermistor and nasal prong pressure transducer); electrocardiogram; and snoring (microphone). The PSG was performed using Alice® 5 and Alice® 6 diagnostic equipment (Philips, Respironics Inc, Murrysville, Pennsylvania, USA). The scoring of PSG raw data (sleep stages and respiratory events) was performed manually, epoch (30 seconds) by epoch by certified sleep technologists in accordance with established criteria.13 Apnea was defined as a drop in the peak thermal sensor excursion of ≥90% of the baseline for ≥10 seconds. The event was scored as obstructive apnea if associated with continued respiratory effort and central apnea in the absence of inspiratory effort throughout the entire period of absent airflow. Hypopnea was defined as a reduction in nasal pressure signal of ≥50% that lasted ≥10 seconds, resulting in a ≥3% decrease in oxygen saturation from the pre-event baseline or an arousal. The apnea hypopnea index was calculated by dividing the number of apneas and hypopneas by total sleep time in hours and is expressed as events/hour. The desaturation index was calculated by dividing the number of desaturations (drop in oxygen ≥3%) by total sleep time and expressed as events per hour of sleep. The OSA was defined according to the International Classification of Sleep Disorders (ICSD 2005).14
Continuous positive airway pressure titration protocol
The CPAP titration was performed during the therapeutic night in accordance with the American Academy of Sleep Medicine guidelines.15 Continuous positive airway pressure was provided to the patient by the hospital if CPAP machine were available at the time of diagnosis. If not available in the hospital, patients were asked to buy the machine. The CPAP machines provided by the hospital were conventional CPAP. Bought CPAP machines included both conventional and auto-CPAP. All machines were provided with a built-in heated humidifier.
Definition of CPAP acceptance and good compliance
Continuous positive airway pressure was considered initially accepted if the patient completed the titration trial in the USDC under PSG recording and described his/her sleep on CPAP as being good.10 The American Thoracic Society (ATS) definition of CPAP compliance was adopted during the analysis of data.16 Continuous positive airway pressure users were considered to have good compliance to therapy if they used CPAP regularly for >4 hour/night for >70% of the recorded period; and to have partial compliance if they used CPAP >2 hour/night and have subjective improvement in OSA-related symptoms such as quality of life.16 Those who stopped using CPAP or did not meet the above criteria were labeled as non-users.16 The CPAP compliance was assessed by downloading mask-on time tracking data from CPAP machines to a computer through a card containing a microprocessor chip, which allows objective measurement of CPAP therapy compliance.6
The CPAP compliance follow-up protocol
Follow-up of patients in the clinic was carried out at one, 4, and 10 months after initiating CPAP therapy. During each follow-up visit, patients received training on their CPAP machines. Continuous positive airway pressure-related side effects and obstacles that prevent good compliance were documented during each visit by completing a data entry form under the supervision of an educationalist and a sleep technologist. This data entry form included commonly encountered side effects such as mask discomfort, intolerance and claustrophobia, nasal congestion or dryness, nasal bridge redness or ulceration, gastric distension, eye discomfort or irritation, air leak, air hunger, and noisy machine. Side effects related to CPAP therapy use were solved by a sleep technologist. The CPAP compliance was determined objectively during each visit by downloading machine-on time tracking data from the patient’s CPAP machine. In between follow-up visits, patients had direct access to USDC via telephone call during daytime working hours for troubleshooting, and convenient access to visit CPAP clinic if needed within 1-2 weeks.
Statistical analysis
Data were presented as mean ± standard deviation (SD) or number (%). Between groups, a comparison of categorical variables was performed using the chi-square test, while the comparison of continuous variables was performed using student t-test. To explore predictors of CPAP adherence, a univariate logistic regression model was used in a preliminary analysis; one explanatory variable was tested in the model at a time including baseline demographic, ESS and PSG data, and side effects measured during each follow-up visit. Subsequently, variables with significant p-values were further evaluated using a multivariate logistic regression model (Forward Wald Method). The p-value <0.05 was considered statistically significant. The multicollinearity between variables was assessed by the correlation matrix among variables included in the model, which showed no multicollinearity. Moreover, multicollinearity was also re-assessed by evaluating the standard error in the model. The IBM SPSS statistics, version 21.0 (IBM Corp., Armonk, NY, USA) was used for data management and analytical activities.
Results
Study population
During the study period, 201 patients were diagnosed to have OSA; however, 156 patients (n=86 men) agreed to participate in the study. There were no differences between the patients who agreed to participate and the patients who declined participation regarding age, gender distribution, body mass index (BMI), comorbidities, or apnea hypopnea index (AHI). The patient characteristics are summarized in Table 1. The mean age of the study group was 51.9 ± 12.1 years, BMI was 38.4 ± 10.6 kg/m2 and AHI was 63.7 ± 39.3 events/hour. Continuous positive airway pressure acceptance during the titration sleep study was 91%. Table 2 shows the baseline data of patients grouped according to their CPAP use after the 10 months. Mean age, AHI, BMI, ESS, CPAP pressure, and gender were not different among the 3 groups. At baseline, patients with good compliance spent more time in stage N2 sleep and less time in stages N3 sleep and REM sleep, which may reflect poorer sleep quality.
Demographic and sleep characteristics of all patients with obstructive sleep apnea at baseline.
Comparison between patients according to their CPAP compliance at 10 months.
Continuous positive airway pressure compliance
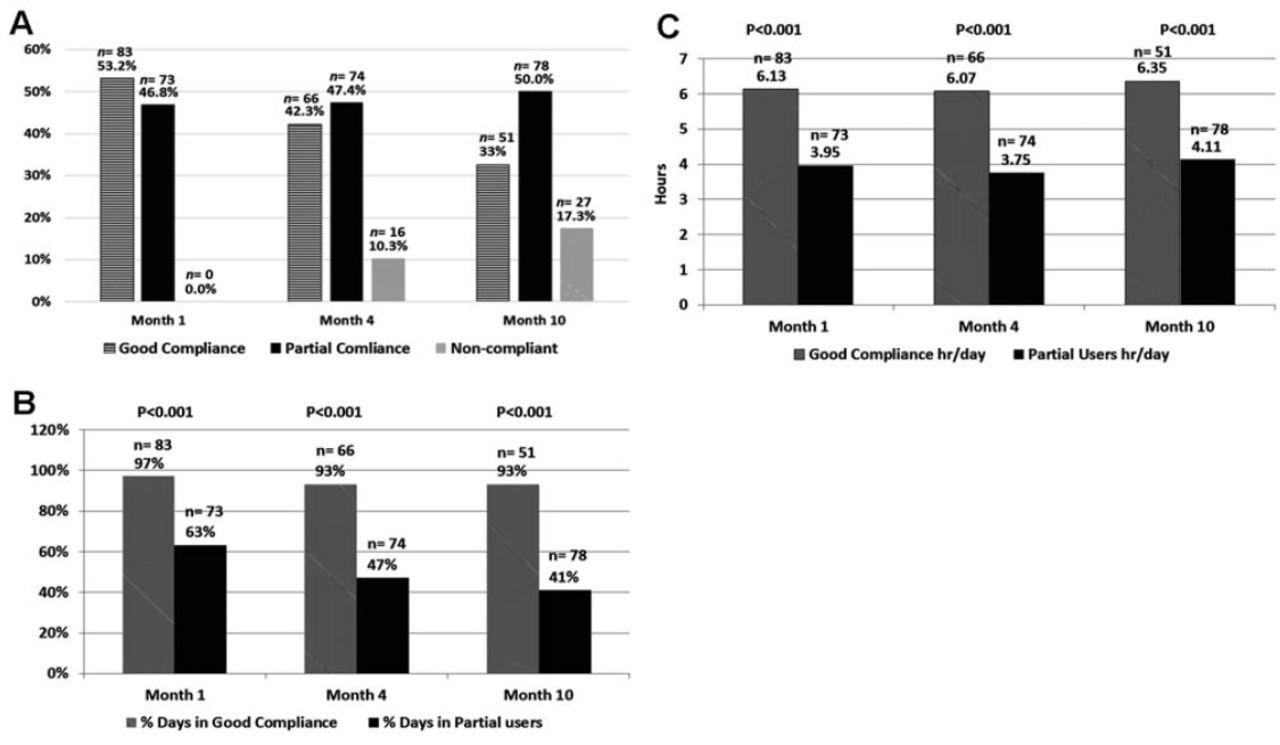
Figure 2A shows CPAP compliance at one, 4, and 10 months. The percentage of good compliers decreased over time (at one month 53.2%, at 4 months 42.3%, and at 10 months 33%). Nevertheless, >80% of the enrolled participants were still using CPAP at the end of the study. At the end of the study, 33% met the criteria for good compliance, and 50% met the criteria for partial compliance. Figure 2B shows the percentage of days during which CPAP was used, and Figure 2C shows the average hours of CPAP usage per day in good and partial compliers.
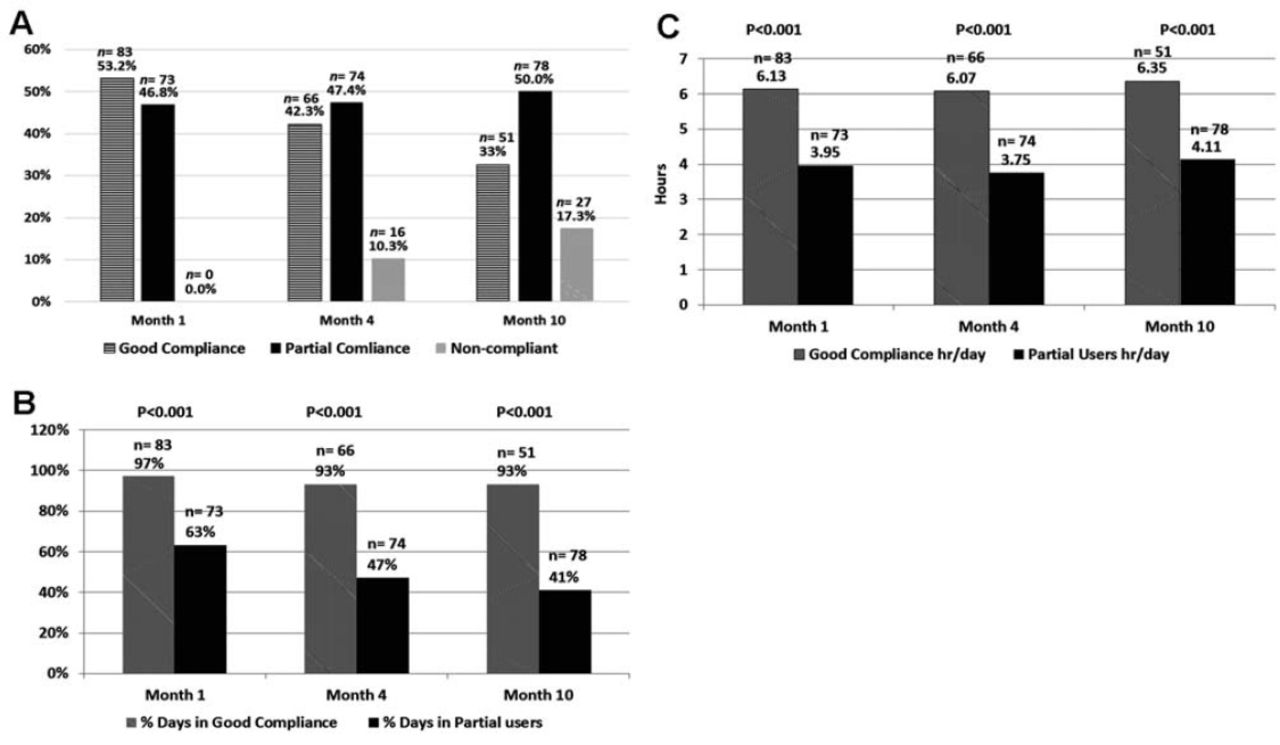
Continuous positive airway pressure (CPAP) compliance at one, 4 and 10 months. The comparisons revealed that: A) CPAP compliance (%) at one, 4, ad 10 months p-value was <0.05 based on Friedman analysis (over all group difference). When pair-wise comparisons were made between different pairs using paired sample Wilcoxon test, the difference was statistically different (p-value<0.05). B) Percentage of days during which CPAP was used. C) Average hours of CPAP usage (hour/day).
Predictors of good CPAP compliance
Table 3 shows the independent predictors of good CPAP compliance at months one, 4, and 10 using univariate and multivariate logistic regression analysis. During month one, “being employed”, “using auto-CPAP”, and “the presence of CPAP-related side effects” remained significant predictors of CPAP compliance in the multivariate regression model. At month 4, multivariate regression analysis indicated that arousal index and comorbid bronchial asthma remained significantly associated with the CPAP compliance At month 10, multivariate analysis revealed that stage N2 sleep, presence of CPAP-related side effects and comorbid bronchial asthma remained significantly associated with CPAP compliance.
Independent predictors of good continuous positive airway pressure (CPAP) compliance using univariate and multivariate logistic regression at months one, 4, and 10.
Continuous positive airway pressure-related side effects
Table 4 shows the CPAP-related side effects at one, 4, and 10 months in patients who were using CPAP. Mask discomfort and nose and mouth dryness were the most common side effects. Table 5 shows the reasons for abandoning CPAP use. Most patients stated a general dislike of CPAP without more specific details being given (48.1%).
Side effects of CPAP use among patients who were using CPAP at one, 4, and 10 months.
Reasons for patients with obstructive sleep apnea abandoning CPAP use (n=27).
Discussion
This study assessed CPAP compliance prospectively and objectively among Saudi OSA patients after applying an intensive educational and supportive program. The study shows that more than 80% are still using CPAP at the end of the study with average nightly use of >4 hour/night, which is higher than previously reported.10 An earlier study that assessed CPAP compliance (self-reports) after 3 months in Saudi patients with OSA revealed that only 39% of the patients were still using CPAP.10 A recent Cochrane meta-analysis17 that included 30 randomized parallel controlled trials assessed the effectiveness of educational, supportive, and behavioral strategies in encouraging CPAP adherence in CPAP-naïve patients with severe OSA. Compared with usual care, supportive ongoing interventions increased machine usage around 50 min per night, and increased the number of participants who used their machines for longer than 4 hour/night from 59% to 75%.17 Educational interventions increased machine usage around 35 min per night, and increased the number of participants who used their machines for longer than 4 hour/night from 57% to 70%. The increase in the proportion of CPAP users in the current study may reflect the importance of education and support on CPAP compliance. A randomized control trial is needed to determine the causal effect of the education and support protocol employed in this study on CPAP compliance. Several studies have attempted to use demographics or initial PSG results to predict subsequent CPAP compliance. However, conflicting data have been reported. In our study, age, gender, BMI, daytime sleepiness (as measured by the ESS), CPAP pressure, and OSA severity did not predict subsequent CPAP use. While our findings concur with some studies,18,19 others have reported CPAP compliance to correlate with daytime sleepiness and OSA severity reflected by AHI or oxygen desaturation index.20,21 A possible explanation for the lack of effect of OSA severity in our study is the fact that most of the patients referred to our sleep disorders center have severe OSA (AHI>30 events/hour) as our center is a tertiary referral center. Moreover, in a recent systematic review of CPAP adherence, the association between AHI and CPAP adherence was found to be weak when other factors were included in the analysis.22 Nevertheless, stages N2 and REM sleep appeared as predictors of CPAP compliance across the follow-up periods in our study. There have been no data available on sleep architecture and its potential to predict compliance to CPAP. We found that increased stage N2 sleep and decreased stage REM sleep were associated with better CPAP compliance. Increased stage N2 sleep and reduced stages REM and N3 sleep may reflect increased OSA severity. Stage N2 sleep has been shown to increase in percentage across mild and severe OSA; while REM sleep showed an inverse pattern.23 This pattern reflects worse sleep quality.23 It is likely that patients with more severe OSA as reflected by increased stage N2 sleep and reduced stage REM sleep have better CPAP compliance. Our results therefore agree with the findings of previous studies demonstrating that the severity of OSA correlates with CPAP compliance. On the other hand, studies have reported conflicting data with regards to the influence of daytime sleepiness on CPAP compliance. While some studies reported daytime sleepiness to be predictive of better CPAP adherence.24-26 Others did not show any influence of daytime sleepiness on CPAP adherence.20,22 Nevertheless, the effect of daytime sleepiness was found to be weak when other factors were included in the analysis.22 It is possible that other unmeasured daytime, symptoms affecting the patient’s quality of life may be more important determinants of CPAP adherence than daytime sleepiness measured by the ESS.
In the first month, “being employed”, “presence of CPAP side effects” (odds ratio [OR]: 0.08; confidence interval [CI]: 0.01 - 0.67) and “use of auto-CPAP” (OR: 2.85; CI: 1.23 - 6.62) remain as independent predictors of CPAP compliance in our cohort. Employment status has been reported to impact adherence to treatment in various disease settings.27 Data about the effect of auto-CPAP reported conflicting results. Two meta-analyses have assessed the differences between auto-CPAP and conventional CPAP in the treatment of OSA. Ayas et al28 reported that auto-CPAP and conventional CPAP were similar in adherence rates, elimination of respiratory events, and improvement of subjective sleepiness. In a recent meta-analysis that included 24 randomized controlled trials, Ip et al29 reported improved CPAP compliance by 11 minutes per night in the auto-CPAP group. Nevertheless, auto-titrating CPAP may enhance adherence in the subgroups of patients who have persistent side effects, those needing higher CPAP pressure and young patients.30,31 At 10 months, persistence of CPAP-related side effects (OR: 0.37; CI: 0.17 - 0.79) remained as an independent predictor of CPAP compliance. Despite the advancement in the technology of CPAP therapy, around 60% of patients experience CPAP-related side effects that may influence their long-term adherence.6 Mask discomfort and nose and mouth dryness remained the most common side effects across the study period. Our findings concur with previous studies, which reported that interface discomfort is the most common side effect encountered among CPAP users (reported in >50% of users).32 Nasal problems such as nasal congestion, dryness, and rhinorrhea are frequently encountered among CPAP users.32 Heated humidification has been developed to adjust inhaled air humidity and temperature in order to reduce inhaled air dryness and improve acceptance and hence adherence to CPAP.3 In our study, comorbid bronchial asthma has been identified as an independent predictor of lower CPAP compliance. Previous studies did not report asthma as a predictor of CPAP compliance. These findings needs confirmation by other studies as bronchial asthma has been reported to be highly prevalent among Saudi patients with OSA.33 Among patients who stopped using CPAP, a dislike with CPAP accounted for approximately 50% of the reasons for abandoning CPAP. Wolkove et al19 reported that a dislike or discomfort with CPAP was the reason for not using CPAP among 44% of OSA patients. Therefore, intensive education, adequate support, and early monitoring of adherence seems critical as the literature suggests that several side effects can occur during the first few weeks of CPAP use and may lead to discontinuation of the treatment.32
A limitation of this study is that it is applied in a single tertiary center and hence presented data cannot be extrapolated to other sleep disorders centers in Saudi Arabia. The fact that the study design is uncontrolled limits drawing solid conclusion on the effect of education and support approach on CPAP compliance.
In conclusion, this prospective study shows that with intensive education, support, and close monitoring, more than 80% of Saudi patients with OSA continue to use CPAP for after 10 months of initiating CPAP therapy. “the presence of CPAP-related side effects” was a persistent predictor of poor CPAP compliance. Therefore, establishment of education and support programs in local sleep disorders centers are needed to improve CPAP compliance among OSA patients. Additionally, close follow-up of patients on CPAP therapy particularly in the first few week of CPAP use is essential to resolve CPAP-related side effects and enhance CPAP compliance. Future studies should follow patients for longer periods to assess CPAP compliance.
Illustrations, Figures, Photographs
Four copies of all figures or photographs should be included with the submitted manuscript. Figures submitted electronically should be in JPEG or TIFF format with a 300 dpi minimum resolution and in grayscale or CMYK (not RGB). Printed submissions should be on high-contrast glossy paper, and must be unmounted and untrimmed, with a preferred size between 4 × 5 inches and 5 × 7 inches (10 × 13 cm and 13 × 18 cm). The figure number, name of first author and an arrow indicating “top” should be typed on a gummed label and affixed to the back of each illustration. If arrows are used these should appear in a different color to the background color. Titles and detailed explanations belong in the legends, which should be submitted on a separate sheet, and not on the illustrations themselves. Written informed consent for publication must accompany any photograph in which the subject can be identified. Written copyright permission, from the publishers, must accompany any illustration that has been previously published. Photographs will be accepted at the discretion of the Editorial Board.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This study was supported by a grant from the Strategic Technologies Program of the National Plan for Sciences and Technology and Innovation in Riyadh, Kingdom of Saudi Arabia.
- Received March 5, 2015.
- Accepted May 30, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.