


Abstract
Objectives: To study the incidence rate of lung cancer and its time trend in Basrah during 2005-2012.
Methods: This was a cancer registry-based retrospective study including all Basrah inhabitant patients diagnosed with primary lung cancer during the period from January 2005 to December 2012. The crude incidence rate was calculated in addition to the age standardized incidence rate (ASIR)/100,000 using the world standard population.
Results: Out of 746 registered cases of lung cancer in Basrah, 75.9% were males and 24.1% were females with a male: female gender ratio of 3.1:1. The crude incidence rate was 3.93/100,000 (5.89/100,000 for males and 1.93/100,000 for females). The ASIR was 8.25/100,000 (13.30/100,000 for males and 4.08/100,000 for females). The time trend showed a decrease in incidence rate in the last 2 years (2011 and 2012) compared with the preceding years.
Conclusion: The incidence rate of lung cancer in Basrah did not differ greatly from that reported for some Arab and neighboring countries. No definite time trend could be identified apart from a tendency for the incidence rate to decline in 2011 and 2012.
Primary lung cancer represents one of the major 5 incident malignancies and the leading cause of cancer-related deaths in Basrah and the rest Iraq.1-5 Evidence from local studies suggests that lung cancer is fatal in the absolute sense and in terms of the 5-year survival rate, which might be as low as 0%.4,6,7 Prognosis seems only modestly related to stage of cancer at diagnosis. Fatality, though reduced among patients with early-detected cancer,8 remains high among the overall mix of cases. This would leave primary prevention as the best alternative strategy on the long run. Evidence in the global literature is sufficient enough to discriminate smoking as the major cause of lung cancer.9-11 Thus, primary prevention should mainly but not exclusively concentrate on prevention of smoking and/or cessation of smoking. However, a reliable documentation of the extent of lung cancer among the population is essential for the planning and monitoring of control strategy. This paper attempts to present a profile on lung cancer in Basrah, Iraq over a decade time.
Methods
This was a retrospective cancer registry- based study including all Basrah inhabitant patients diagnosed with primary lung cancer during the period from January 2005 to December 2012.
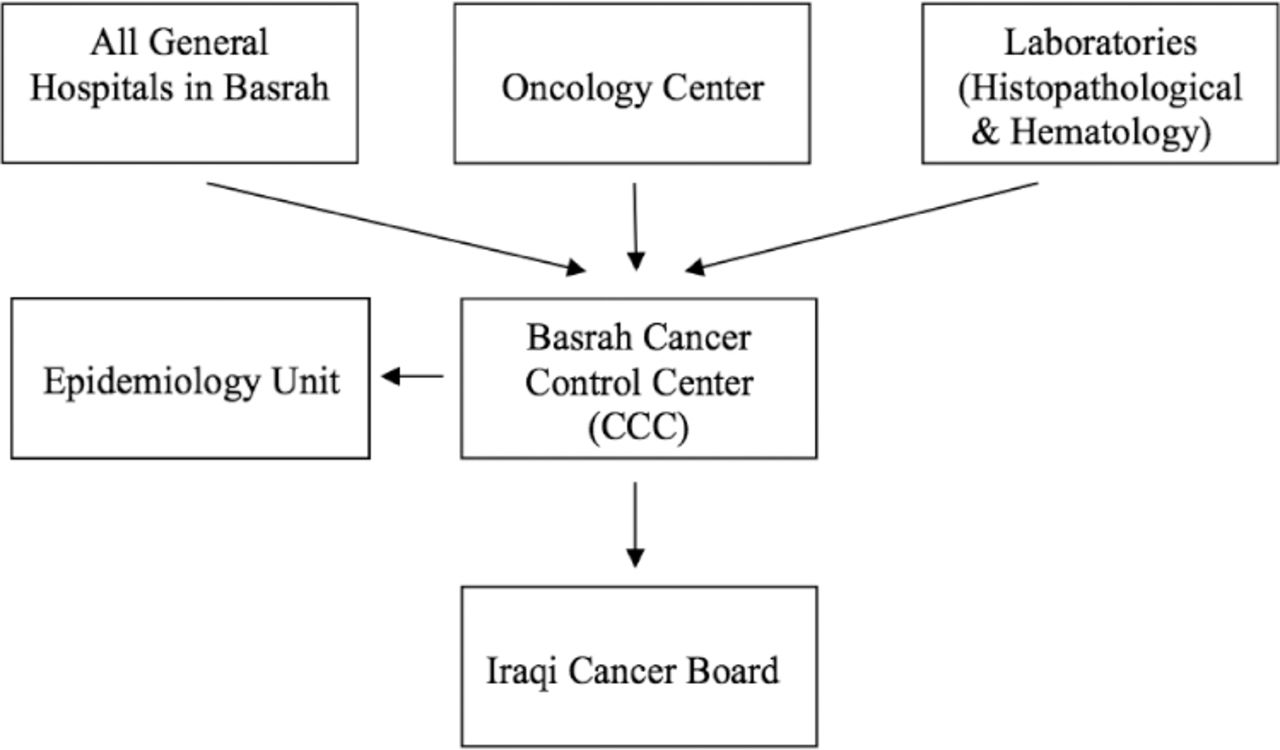
Usually, people with cancer are mainly identified and their cancer is diagnosed when they visit specialist doctors in private clinics, the consultancy clinics in major hospitals, and centers specialized to deal with cancer in Basrah governorate. Few cases may be detected in primary health care institutions as well. Some cases may receive diagnostic and therapeutic care outside Basrah, Iraq, but even these may be registered by cancer registration centers. In each of the major hospitals, a cancer registration unit exists. These units report registered cases to the Cancer Control Center (CCC) as the point of pooling of cases at Basrah governorate level. Cases which are treated in the specialized oncology centers are also reported to the CCC. Further major source of cases is a histopathological cancer registration, which was established at the Department of Pathology and Forensic Medicine, College of Medicine, University of Basrah to compile and register solid tumors. Childhood cancers are treated at the Children Specialized Hospital. All cases registered in all these registration units and centers are compiled and pooled in one epidemiological unit at the College of Medicine for checking and for epidemiological analysis (Figure 1). In each cancer case, the CCC may, therefore, receive single or multiple notifications (clinical, radiological, histopathological, hematological, immunochemical, and so forth). All the data are fitted on Can Reg 4 format and fed into the computerized database of the CCC. The system is robust to any duplication. In addition, further checking is made by the epidemiological unit at the Basrah College of Medicine using excel sheets on all reported cases.
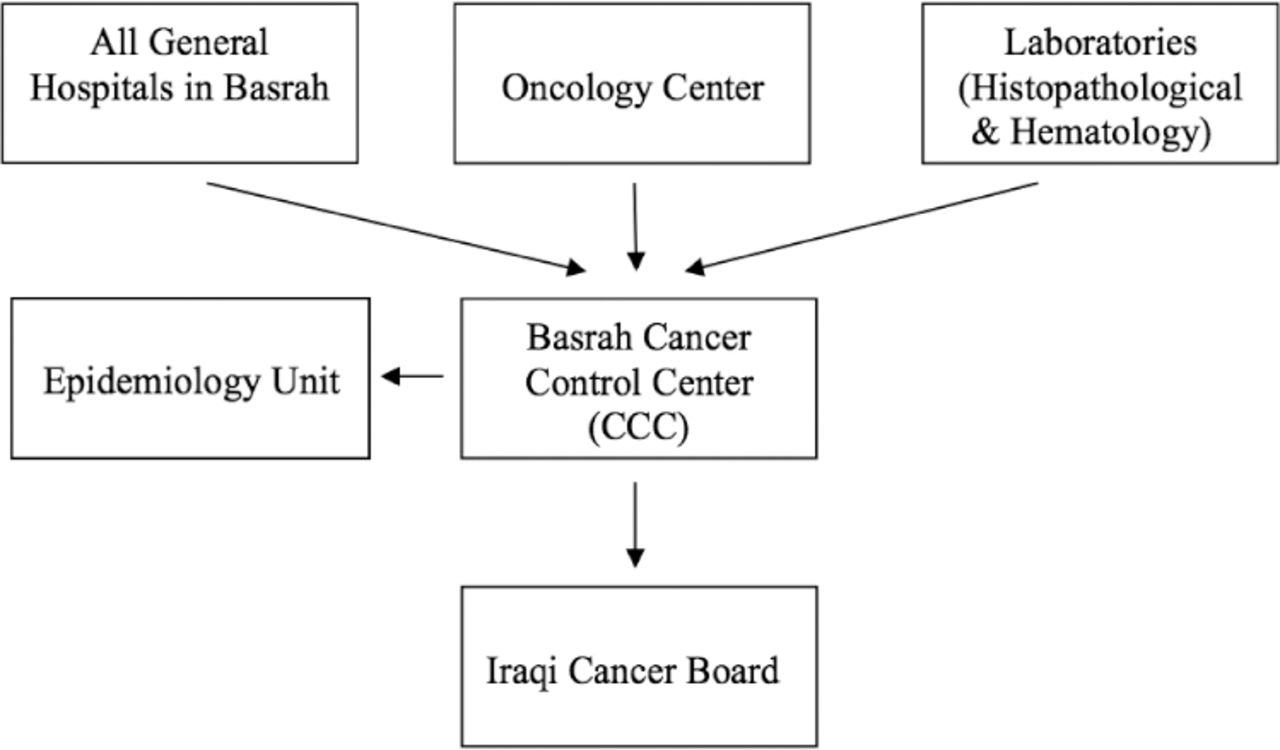
Flow chart showing cancer registration in Basrah, Iraq.
The cases which are registered in Basrah are drawn from the population of Basrah and adjacent governorates. From an epidemiological point of view, cases can be identified and classified according to age, gender, place of residence, cancer site, histopathological typing, year of diagnosis, and source where they were first identified.
Data on lung cancer cases from all these sources were used in this study. Excel files were obtained for each of the 8 years covered in the study (2005-2012). The data were thoroughly checked for errors and duplication using the Excel program. The final set of data verified to contain 1363 cases of lung cancer; 746 of them were from the inhabitants of Basrah governorate. The latter were used for statistical analysis in this paper. Cases from other governorates were excluded from analysis to avoid distortion of calculation of parameters for Basrah.
No screening program for lung cancer is in effect in Basrah. Diagnosis and treatment follows the normal practice of oncology. Figures on Basrah population were obtained from various sources, including Ministry of Health, Ministry of Planning and Developmental Collaboration,12 and local household surveys.13 It was possible to have total population estimates for each year by age and gender.
The data were imported into the Statistical Package for Social Sciences version 19 (IBM Corp., Armonk, NY, USA). Age specific and year specific incidence rates were calculated. The age standardized incidence rates (ASIR) were also calculated using World population as the standard population.14
This study was approved by the Ethical Committees of College of Medicine, Basrah University and Basrah General Health Directorate, Basrah, Iraq.
Results
During the period 2005-2012, a total of 746 cases of primary lung cancer were diagnosed in Basrah, 566 (75.9%) were male and 180 (24.1%) were female patients. The crude incidence rate of lung cancer was 3.93/100,000 and it was directly proportional with age in both genders. It was higher among males than in females (5.89/100,000 versus 1.93/100,000 with a male: female incidence gender ratio of 3.1:1). The age standardized incidence rate was 8.25/100,000 population for the total population (13.30/100,000 for males and 4.08/100,000 for females) (Table 1).
Age specific annual incidence rate (IR) (per 100,000) of lung cancer by gender: Basrah 2005-2012.
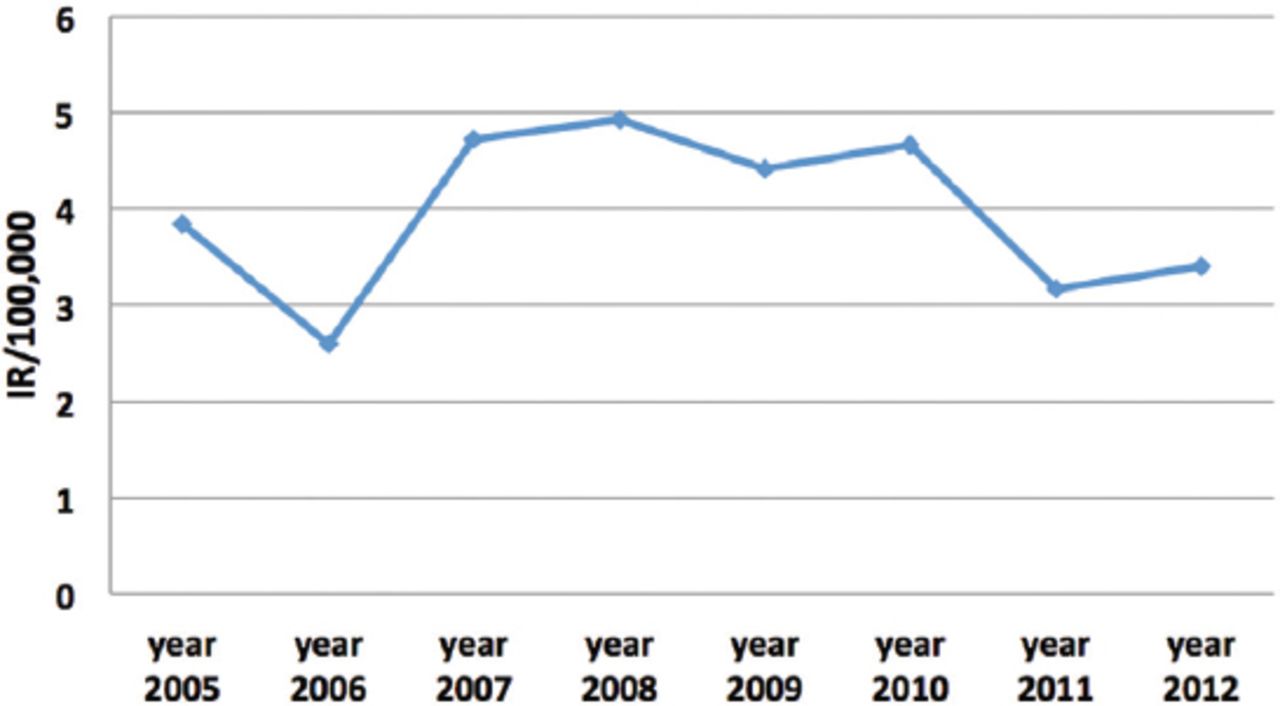
We have tried the Time Series Modeler procedure to perform exponential smoothing, Univariate Autoregressive Integrated Moving Average (ARIMA) models for time series. The output showed no obvious time trend. However, the last 2 years (2011 and 2012) showed lower incidence rates compared with the preceding years (Table 2 & Figure 2).
Incidence rate (IR) of lung cancer during 2005-2012(IR/100,000).
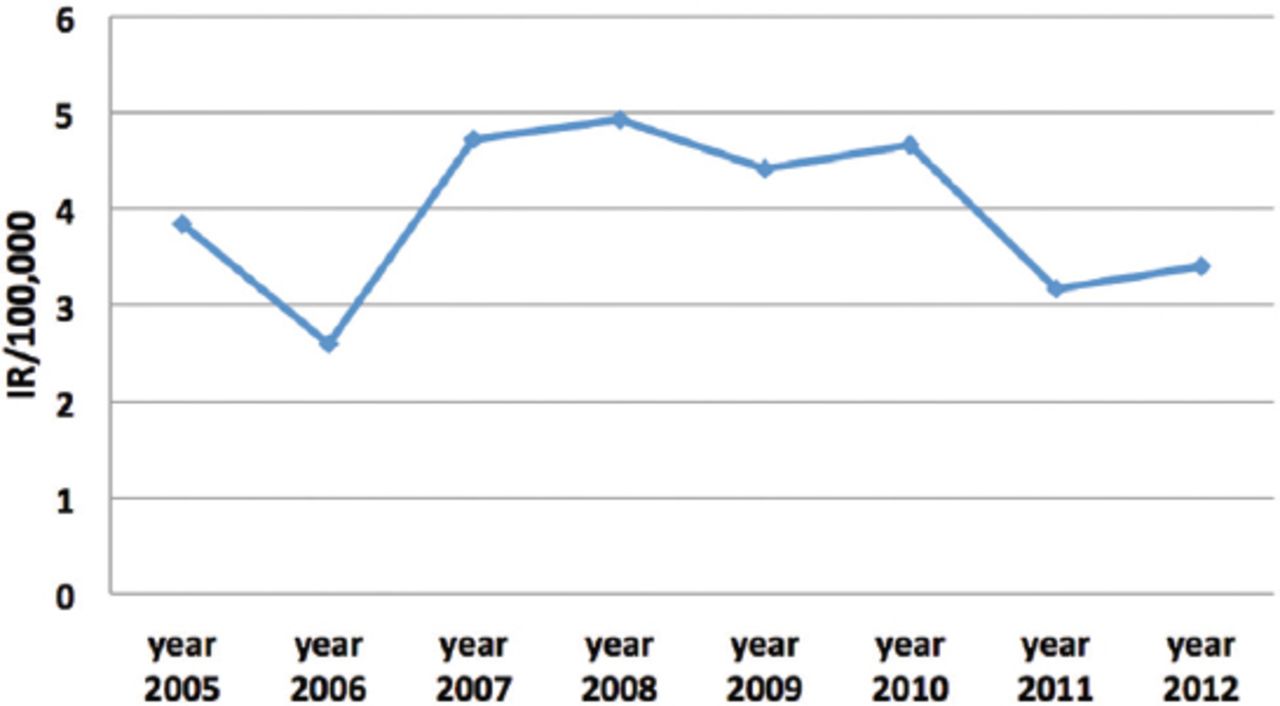
Incidence rates of lung cancer in Basrah during 2005-2012 (IR/100,000 in both genders).
Discussion
Lung cancer is the most common cancer worldwide in terms of incidence and fatality accounting for 12.7% of new cases of cancers and 18.2% of the total cancers’ death globally according to GLOBOCAN 2012.15 More than half of the incident cases occur in developing countries, where resources of treatment and prevention are scarce.16 It was reported that 68.1% of the Arab countries have lung cancer as one of the most frequent 5 types of cancer.17 In Iraq, it is the second most common site of cancer and the first most common site in males.18
In our study, lung cancer incidence among men exceeds that in women with a male: female incidence gender ratio of 3.1:1, a result which had been reported in most nations.19 In Serbia, the gender ratio (males to females) of lung cancer incidence was reported to be 4:1,20 In Ardabil, Iran21 4.6:1, Saudi Arabia 3.9:1, Kuwait 3.0:1, and the United Arab Emirate 2.8:1.16
The median ASIR of lung cancer in all the Arab countries collectively showed that the rates in females were lower than those in males. The ASIR for males was 13.44/100,000 versus 2.91/100,000 for females (male: female ratio 4.6:1).17 Such difference is partly due to low prevalence of smoking among women.22 According to the World Health Organization (2008) estimates, the prevalence of smoking among Iraqi men was 25.8% and 2.5% among women.23 Similarly, many other Arab countries showed higher prevalence of smoking in men than women. The prevalence of smoking among males and females was in; Saudi Arabia (28.7%, 4.5%),24 Kuwait (34.4, 1.9%),25 and Jordan (59.1%, 23.3%).26
The mean age of patients with lung cancer in this study was a 60.7 ± 13.5 years (61.9 ± 12.4 for males and 56.8 ± 15.9 for females without a significant gender difference), which is almost similar to that previously reported in Iraq.27 In USA,28 the mean age at which lung cancer is diagnosed is 70 years. As in many other countries,29-32 the incidence of lung cancer is rare in Basrah before the age of 40 years, with 93.2% of the patients aged 40 years and above.
In both genders, the incidence rate of cancer increased exponentially with age, but the increase of rates slightly slowed down more in men than in women in older age groups (65 years and more). This deceleration in incidence rate could reflect patterns of smoking initiation and quitting or cohort effect linked to variations in tobacco consumption.29,33 Those who initiate smoking earlier in life are most likely to develop lung cancer at younger ages,19 and the risk of developing lung cancer decreases among those who quit smoking early compared with those who continue to smoke.34 It was reported that the prevalence of smoking peaked 2 decades earlier among men than women.33,35 When younger birth cohorts aged, their risk of lung cancer development will be reduced, but such reduction will be more for men than women.34
Age as a risk factor for malignancies is well documented; it reflects intensity and long term exposure to risk factors such as lifestyle behaviors, particularly smoking.20 Smoking is the leading cause of lung cancer and it was reported that 85-90% of lung cancer patients had a history of current or passive smoking.36
The age standardized incidence rate of lung cancer in Basrah was double the crude incidence rate. This is due to the fact that more than 95% of the Iraqi population were under 65 years of age.12,13
The crude incidence rate of lung cancer in Basrah was 3.93/100,000 population (5.89/100,000 for males and 1.93/100,000 for females), while the age standardized incidence rate was 8.25/100,000 population (13.30/100,000 for males and 4.08/100,000 for females). Such incidence rate is comparable to what was reported previously for Iraq (ASIR was 14.6/100,000 for males and 3.6/100,000 for females),15 and in Mosul, Iraq (crude incidence rate for lung cancer was 5.23/100,000 and the age-standardized incidence rate was 12.67/100,000 for male population in 2010).37
Also, it is comparable with that reported in some Arab and neighboring countries. In Qatar,31 it was 8.95/100,000 (15.2 per 100,000 for males; 3.95 per 100,000 for females), Iran, East Azerbaijan38 (16.6 for males and 4.2 for females). It is higher than that reported for Oman39 (7.7/100,000) for males), Bahrain40 (6.2/100,000, 10.4/100,000 for males and 2.6/100,000 for females), Saudi Arabia17 (7.2/100,000 for males and 3.0/100,000 for females, and Syria17 (9.9/100,000 for males and 2.1/100,000 for females), but it is lower than that reported for Jordan42 (17.6/100,000 for males and 5.1/100,000 for females), and Lebanon42 (31.8/100,000 for males and 13.7/100,000 for females). The ASIR of lung cancer in some Arab countries is shown in Table 3. In Arab countries, including Iraq, the incidence rate of lung cancer is lower than that in Europe and United States.17 (GLOBOCAN estimates ASIR of lung cancer in USA for males 48.5/100,000 and 35.5/100,000 for females).15 Such geographical variation in incidence rate of lung cancer could be attributed to many factors: variation in cancer registry and quality of data, prevalence of risk factors particularly smoking and air pollution, means of diagnosis, genetic predisposition, and socio-cultural factors that alter lifestyle behaviors.
Age standardized incidence rate (ASIR) of lung cancer and prevalence of smoking among some Arab countries.
No exact time trend for lung cancer in Basrah can be drawn from the results of this study, but the incidence rates in the last 2 years (2011 and 2012) showed a decline in comparison with the previous years, a trend which is similar to that reported in Ninawa, Iraq.37 No explanation for such decrease was found; probably an alteration in the prevalence of risk factors, such as smoking could be one of the reasons. However, such possibility needs further thorough investigation. Under reporting cannot be excluded. Although intensive local efforts to improve cancer registration were made, official registration is still unable to cover all incident cancer cases.43 Such incompleteness is likely to affect estimates of various cancers, including lung cancer, a point which represents a potential limitation of the present study.
In conclusion, the figures presented in this article represent the best epidemiological parameters on lung cancer in Basrah. The incidence rate of lung cancer in Basrah does not vary greatly from that reported in Iraq and some Arab and neighboring countries. Although no particular time trend for the incidence rate of lung cancer in Basrah can be drawn from this study, a slight decrease in incidence rate of lung cancer Basrah in the last 2 years of the study was noticed. Such trend needs further investigation and confirmation. Further research and improved cancer registration is highly recommended.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received May 31, 2016.
- Accepted August 13, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.