


Stomach perforation by ingested fish bone resulting in hepatic abscess is very rare with few case reports in the literature. They present with nonspecific features of an acute abdomen and with less severe clinical features than those perforations present in other parts of the gastrointestinal tract (GIT). The clinical diagnosis is challenging without a definitive history of fish bone ingestion. The main stay of diagnosis is CT scan of the abdomen carried out for evaluation of acute abdomen. We hereby report a rare case of large hepatic abscess caused by fish bone perforating the lesser curvature of the stomach with gastrohepatic fistula.
A 69-year-old male presented with history of high-grade fever and abdominal pain for 5 days. On examination, tenderness was present in the right upper quadrant without jaundice. Laboratory data revealed leukocytosis (14×109/L [normal range [NR]: 11×109/L]). The liver function test revealed elevated total serum bilirubin (36 umol/L [NR: 2-18 umol/L]) and abnormal liver enzymes with increased elevation of alkaline phosphatase (131 U/L [NR: 30-120 U/L]), alanine transaminase (41 U/L [NR: 10-40 U/L]) and aspartate transaminase (55 U/L [NR: 14-20 U/L]). The total serum protein (57 G/L [NR: 64-83 G/L]) and serum albumin (23 G/L [NR: 35-50 G/L]) were decreased.
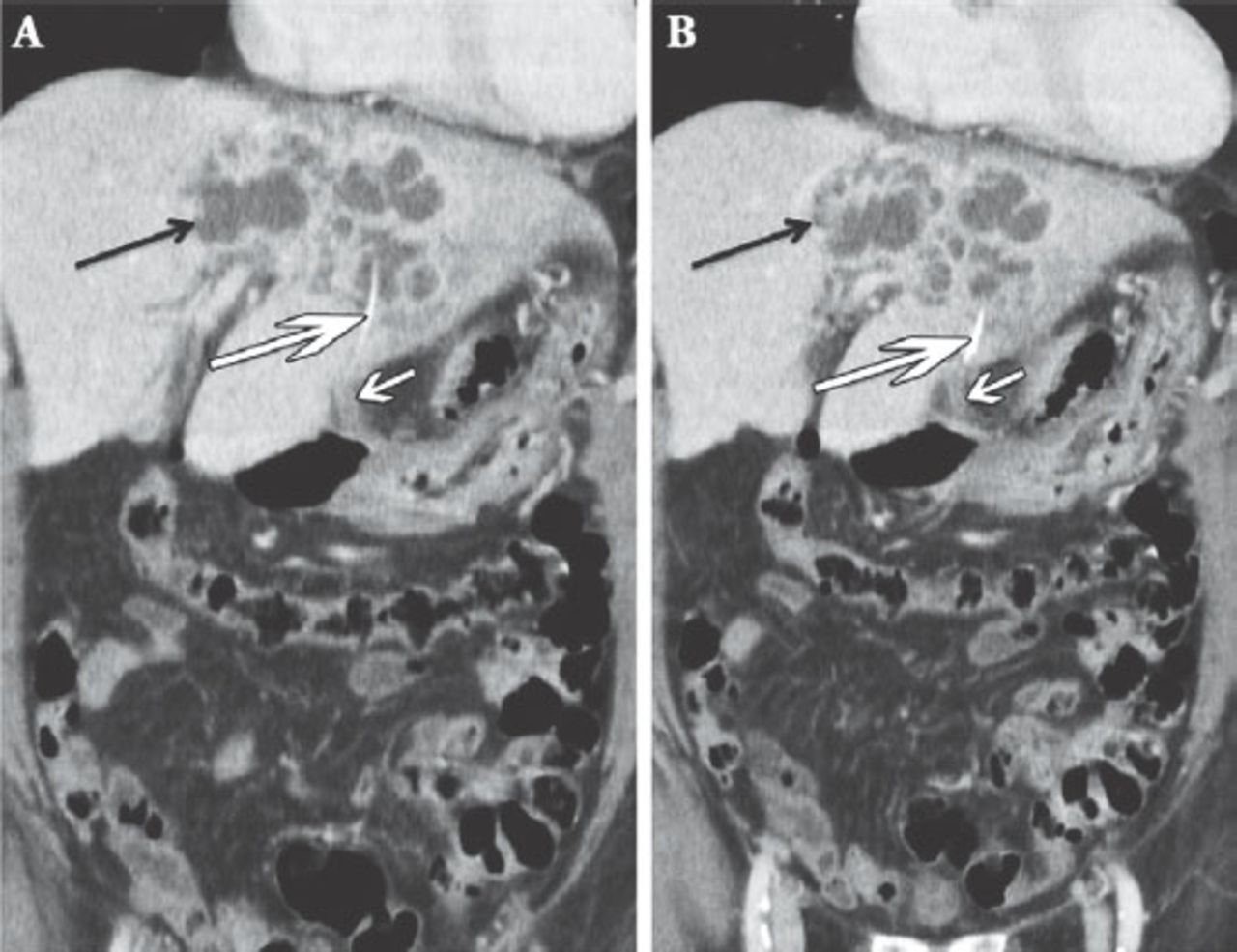
Clinical diagnosis of intra-abdominal sepsis with cholangitis was carried out, and further evaluation with a CT scan of the abdomen was requested. It revealed a multiloculated rim enhancing fluid collection in segments II, III, and IVa (Figure 1) measuring 9.4 × 6.1 × 5.3 cm in size. In addition, a linear radio-density was present in the left lobe of liver extending from the inferior subcapsular region into the collection. Also, there was a short tract bridging the affected liver surface superiorly and the lesser curvature of the stomach inferiorly. Imaging diagnosis of large liver abscess secondary to a foreign body, likely a fish bone perforating the lesser curvature of the stomach and migrating into the liver with bridging fistulous tract between the stomach and liver was made. There was no dilatation of the intra or extrahepatic biliary ducts. The findings were confirmed by open laparotomy; wedge resection of segment II/III abscess with Cavitron ultrasonic surgical aspirator and diathermy were performed. The gastrohepatic fistula was resected. The tiny perforation of the lesser curvature of the stomach was repaired with 2 layers of Vicryl sutures, and the fish bone measuring 1.4 cm was removed. He had a history of ischemic heart disease and developed fast atrial fibrillation on the first postoperative day. He was started on intravenous amiodarone and subsequently converted to sinus rhythm. The fluid culture of abscess returned growing Klebsiella, Proteus vulgaris, Citrobacter freundii, and Alpha hemolytic streptococcus. He was started on intravenous ceftriaxone and metronidazole for one week. At the time of discharge on the eighth postoperative day, he was stable and was put on oral levofloxacin for 2 weeks. He was readmitted after one year from discharge with small bowel obstruction due to extensive adhesion of a small segment of jejunum and transverse colon on the undersurface of the previous incision. Open surgical laparotomy, adhesiolysis, and wedge resection of small bowel were subsequently performed.
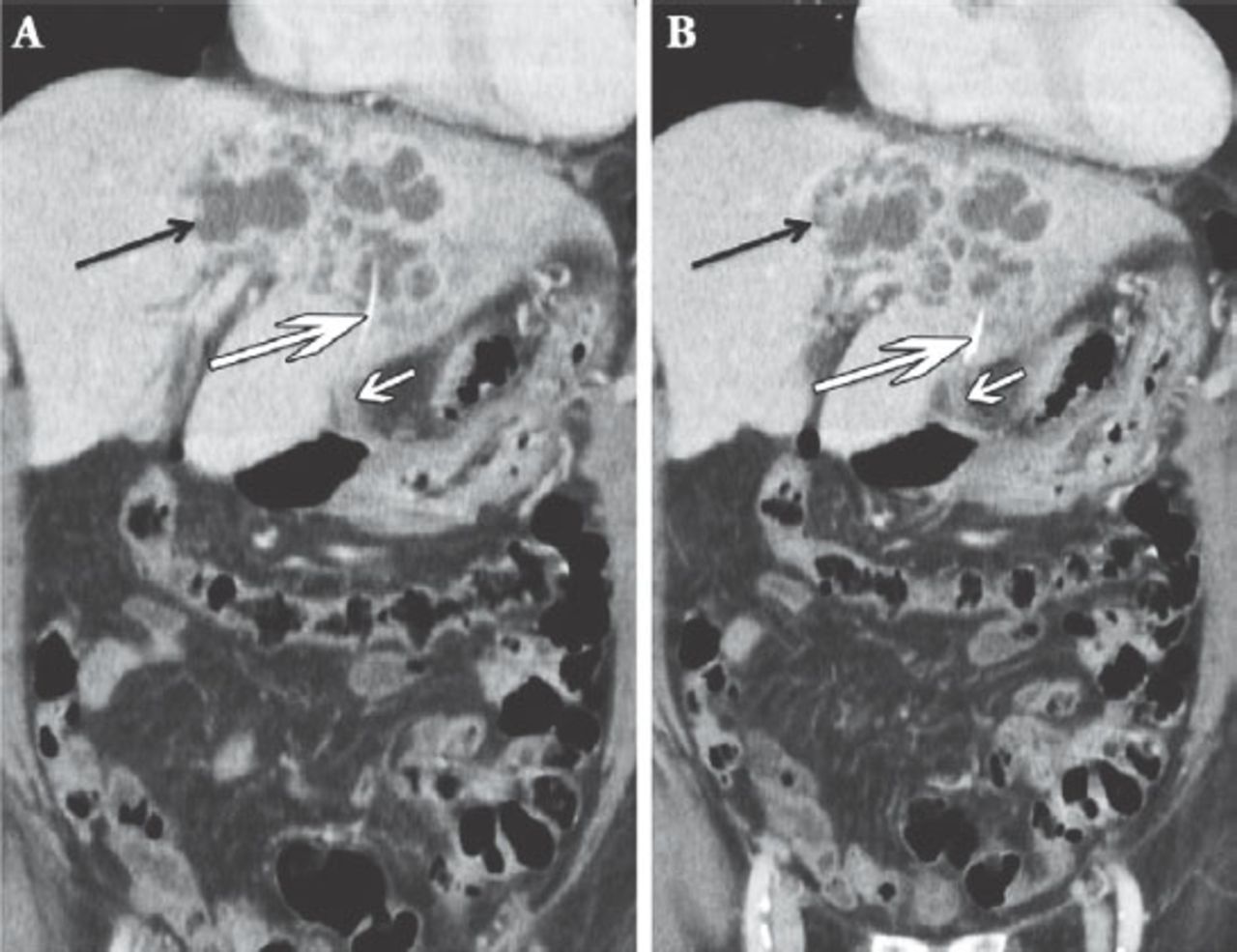
Coronal intravenous contrast enhanced CT scan reveals multiloculated abscess in segments II, III, and IVa (black arrow in A and B). In addition, a linear radio-density is present in the left lobe of liver suggestive of fish bone (long white arrow in A and B). Also, there is a short tract bridging the liver surface and the lesser curvature of the stomach suggestive of a gastrohepatic fistula (short white arrow in A and B).
Fish bone is one of the most commonly ingested foreign bodies. Some studies report they represent up to 80-90% of the foreign bodies ingested.1 The other commonly ingested foreign bodies include chicken bone, toothpick, needles, pens, and dental plates.2 Most of them pass spontaneously without symptoms.1 Foreign bodies usually get impacted at the oesophageal sphincters, pyloric canal, duodenum, ileocaecal valve, and anus where there is expected normal extrinsic impression or anatomical narrowing. Perforations are more common in the oesophagus causing pneumo-mediastinum, retropharyngeal abscess, mediastinal abscess, and bleeding. Perforations and complications beyond the esophagus are rare.3 Such patients present with nonspecific acute abdomen mimicking common pathologies making the diagnosis challenging without definitive history of fish bone ingestion.
Gastrointestinal perforation by an ingested fish bone resulting in hepatic abscess is very rare. In these cases, the site of perforation is usually in the stomach or duodenum with the abscess most commonly developing in the left hepatic lobe, because of its proximity. In the stomach, the site of perforation is usually seen along the lesser curvature because of the anatomical acute angularity. They may be partially embedded in the stomach wall with associated perigastric inflammatory changes or can be complicated with perigastric abscess formation. Rarely, the fish bone may penetrate into the adjacent hepatic parenchyma and cause abscess.4 A gastrohepatic fistula may be formed. The perforations of stomach and duodenum present with less severe clinical features as opposed to perforations in other parts of the GIT. The classic clinical features of hepatic abscess like fever, abdominal pain, and jaundice is usually not seen. Most patients have vague symptoms such as anorexia, and vomiting with leukocytosis with deranged liver function test. Computed tomography scan is the imaging modality of choice, which is carried out to investigate the acute abdomen, and fish bone is incidentally detected. The multiplanar capability easily detects the fish bone, which appears as linear hyperdensity. It can even detect very small and radiographically lucent fish bones. Pneumoperitoneum is less commonly seen because perforation by fish bone is gradual and by pressure necrosis, which may be sealed by surrounding, inflammatory changes.1 The abscess is seen as a rim enhancing collection with or without multiloculations. Microorganisms found in the abscess cultures are the common bacterial flora seen in the oropharynx.5
Small abscess less than 5 cm may be treated with antibiotics. Larger abscess with multiloculations usually are treated with surgery, draining of the abscess, and removal of the foreign body. Some cases of percutaneous or endoscopic removal are also described in the literature.
In conclusion, the patients with accidental fish bone ingestion complications present with nonspecific features of acute abdomen. The clinical diagnosis is challenging without a definitive history of fish bone ingestion. A CT scan with its multiplanar capability is highly valuable to diagnose and accurately localize the ingested fish bone, which can direct accurate timely treatment. In addition, the CT can also provide a comprehensive evaluation of the complications of fish bone ingestion including hepatic abscess.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 24, 2015.
- Accepted May 11, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Related Articles
Cited By...
- No citing articles found.