


Abstract
Objectives To assess the knowledge of Jordanian dentists toward phase down of dental amalgam as recommended by the Minamata Convention, and their training and competency in placing posterior composites.
Methods This study was conducted through structured questionnaire interviews with randomly selected cohort of dentists in Jordan between March 2015 and June 2015. Out of 230 dentists who were invited, 196 (85.2%) agreed to participate. Dentists were asked if they know about the Minamata Convention. They were also asked about their training in placement of posterior composite.
Results Out of the 196 interviewed, only 13.8% know about Minamata Convention and 17% had an undergraduate training in favor of placing composites in posterior teeth. Approximately 50% of those dentists were not trained in using rubber dam when placing posterior composites, while only 38.3% had training in sectional matrix placement. Undergraduate training did not influence (p=0.00) the dentists’ decision to remove old amalgam based on patient’s demands. Only 28.1% were of the opinion of discontinuing the use of amalgam due to its alleged health and environmental hazards. There was no general agreement on the type of composite, liner, and bonding strategy when placing posterior composites.
Conclusion Dentists are not well informed on the Minamata Convention and the phase down of amalgam. Training in posterior composite placement should be given more room in undergraduate curriculum and continuous dental education.
The Minamata Convention,1 drafted by the United Nations Environment Programme in October 2013 and signed by over 100 countries, has obliged countries to minimize the anthropogenic emission of mercury and its products.2,3 The fourth article of this convention identified dental amalgam to be one of the mercury products whose use should be tried to phase down by countries.1 The decision to “phase down” and not to “phase out” of use of dental amalgam by 2020 compared to other mercury-containing products was made to allow for a smooth transition toward amalgam-free dentistry.2,4 The convention identified the use of cost-effective and clinically durable mercury-free materials as a measure to reduce the use of amalgam. It also encouraged dental schools to educate and train dental professionals and students on the use of mercury-free dental restorations. The minimal invasive approach in restorative dentistry has become the standard of care for management of carious lesions.5,6 Preventive and ultraconservative cavity preparations are arguably the logical first line of treatment that restorative dentists should opt for. This paradigm shift has come after many years of unnecessary destruction of sound tooth structure to place amalgam restorations, which rely mainly on macro mechanical retentions.7-9 This is clearly reflected in dental literature and in the dental industry as well. Training of placement of posterior composite restorations began to dominate the operative curriculum in a wide range of international dental schools.10,11 Amalgam is no longer the first choice among instructors, students, or patients.12 Time spent to teach amalgam will continue to fall, and perhaps it will be on preclinical basis, or cease to exist in the next decade.7 Even in a post-amalgam era, dentists would still need to adhere to national and international guidelines of mercury hygiene13 while removing old amalgam fillings or preparing existing restorations to act as the foundation restorations for crowns and fixed partial dentures. Amalgam use has been criticized in the dental literature due to its appearance, environmental hazard, and alleged toxicity.14 Little criticism has been spared for the biological price of amalgam that the healthy tooth structure has to suffer.15 The perceived short longevity16 of composite restorations has been the main factor to slow the transition into amalgam-free practices and training at the dental schools. The rapid development in the production of composite materials based on nanotechnology coupled with better understanding of the bonding mechanisms to both enamel and dentine will probably enhance the longevity of posterior composite restorations and possibly improve their antibacterial effects.17 Most Jordanian dentists do not strictly follow the mercury hygiene and amalgam waste management guidelines.18 Therefore, to encourage amalgam-free practices, there was a need to assess the knowledge of Jordanian dentists toward phase down of amalgam as recommended by the Minamata Convention and to assess their training and competency in placing posterior composites.
Methods
The Faculty of Dentistry Research and Ethics Committee (FDREC) at the University of Jordan, Amman, Jordan has reviewed and approved this study. A random sample of 230 dentists was generated from the Jordanian Dentists Register to investigate their awareness of the Minamata Convention and their opinions and training toward placing posterior composite. The inclusion criteria for interviewed dentists included being a full time dentist, placing direct restorations on daily basis, and willing to participate in study and to give their consent. Dentists, who work outside Jordan, or do not regularly place direct restorations or their practice limited to orthodontics or oral surgery, for example, were excluded from this study. Data was collected through field visits to the dentists’ clinics/workplaces between March and June 2015. The purpose of the study was explained to each dentist, and his/her consent to participate in the study was obtained. Demographic and professional characteristics of the dentists were collected. The dentists were asked if they know about the Minamata Convention and if this convention would affect their practice. They were asked about their undergraduate training in composite placement in posterior teeth, use of rubber dam, and sectional matrices. The dentists were also asked if they had any graduate or continuous education training in posterior composite placement. The reasons why they might abandon using amalgam were also investigated. They were also asked if they would remove amalgam fillings even though those fillings are deemed satisfactory. They were also asked regarding the type of composite they prefer to use in posterior teeth. Type of liner and bonding strategy they prefer were also investigated. They were asked regarding their opinions on the advantages and disadvantages of using composite in posterior teeth.
Statistical analysis was performed using the Statistical Package for Social Sciences for Windows version 16.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were generated, and Chi-square and Fisher’s exact tests were used to examine differences between groups. Differences at the 5% level were accepted as significant.
Results
Out of the 230 dentists selected, 196 (85.2%) agreed to participate in the study. Slightly less than two-thirds (64.8%) of dentists surveyed were males and more than 85% were <40 years old. More than 59% of the dentists received their primary dental degree from Jordan and 24.5% from other Arab countries. The rest obtained their degrees from Russia and eastern and western European and North American countries. Only 27 (13.8%) of all the dentists surveyed know about Minamata Convention. The majority of those (85.2%) agreed that the Minamata Conventions’ implication would not adversely affect their daily practices and thought that this would improve the services they provide for their patients. The country of primary dental degree did not affect this opinion (p=0.00).
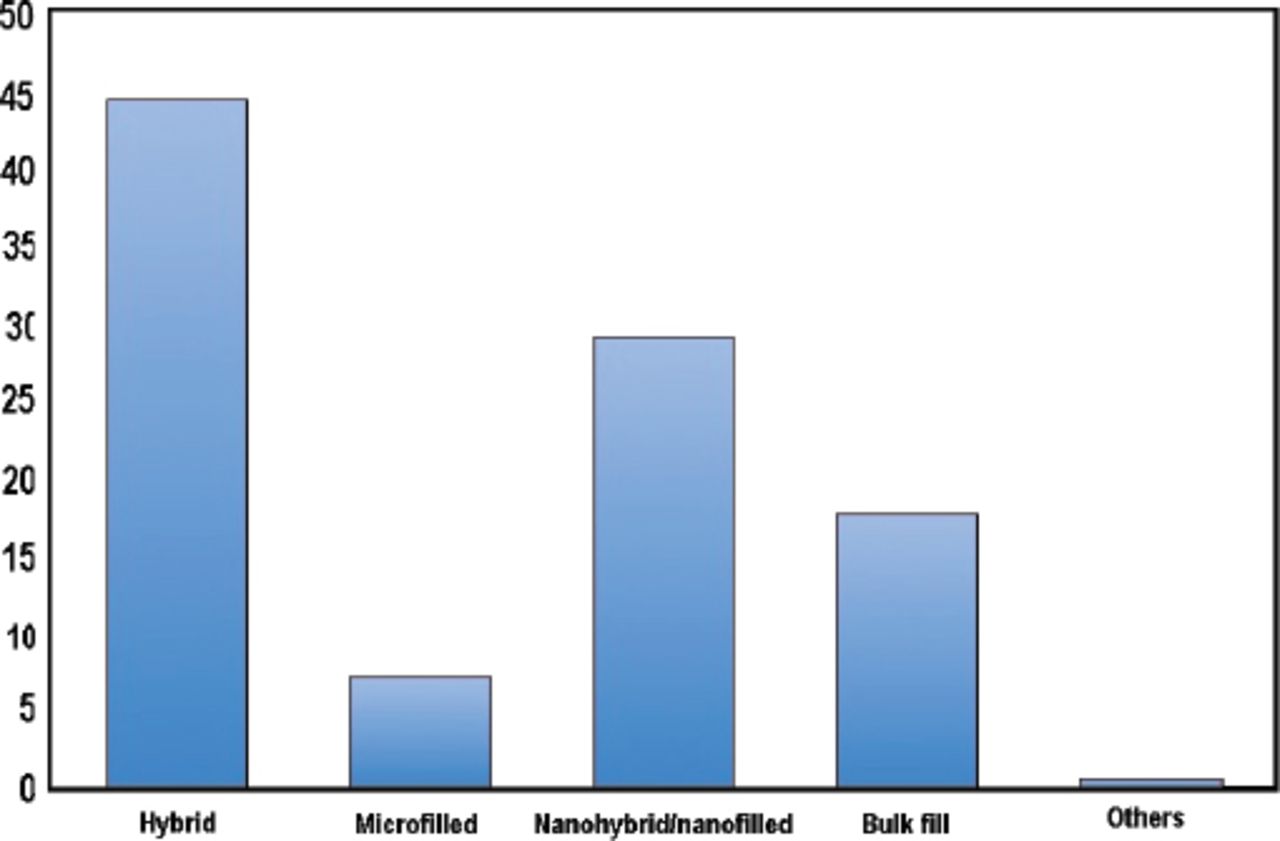
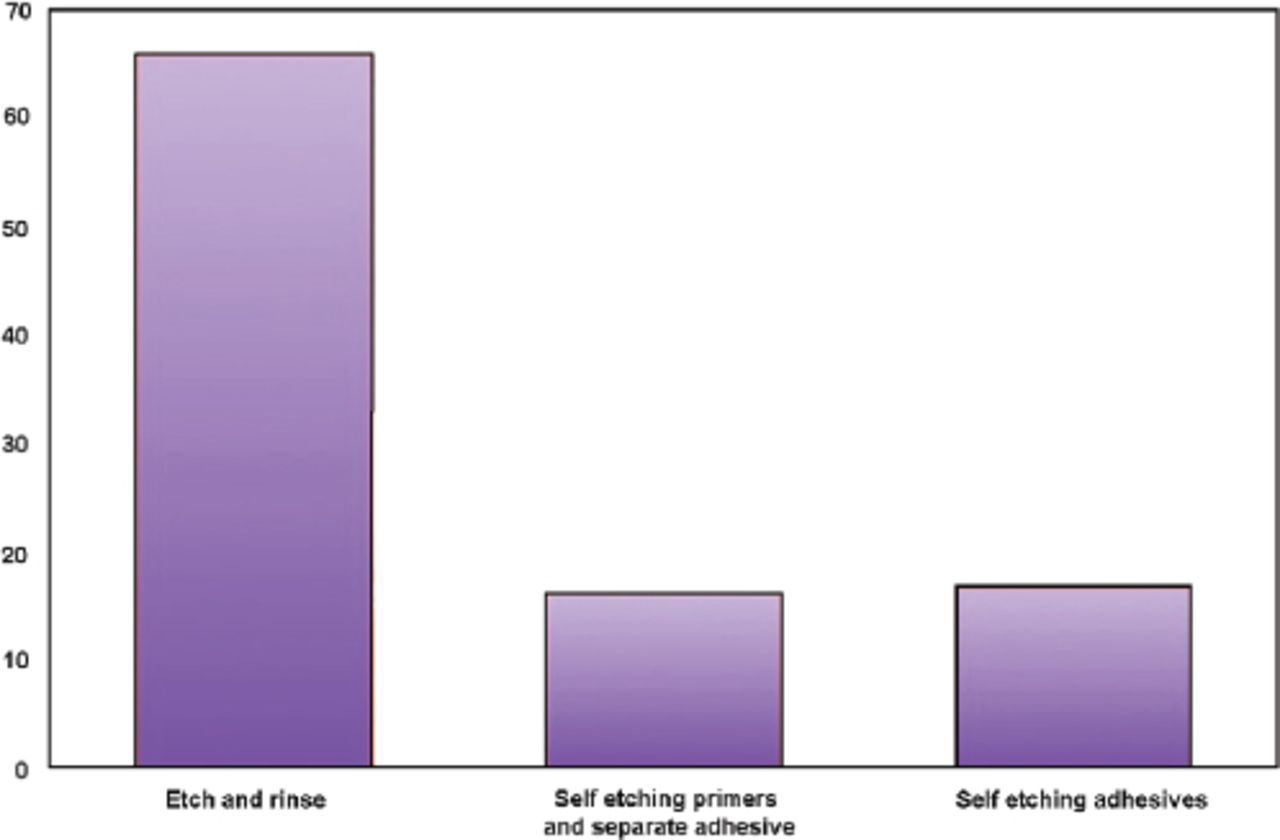
Most dentists had an undergraduate training in favor of placing amalgam when restoring posterior cavities. The country of primary dental degree did not have a significant influence on changing this paradigm (p=0.00). Almost half of the overall dentists had undergraduate training in placement of rubber dam when restoring posterior teeth with composite. Furthermore, only 38.3% had undergraduate training in placement of sectional matrices. More dentists in the younger age groups, less than 40 years, would have had training in aspects related to placement of posterior composite (p=0.00) (Table 1). Less than 45% of dentists opted for postgraduate continuous education courses aiming to improve their skills in posterior composite placement. Two-thirds of the dentists agreed that the use of amalgam in posterior teeth could be totally abandoned. The main reasons for such an opinion were the need to remove sound tooth structure and the appearance of amalgam restorations. Surprisingly, only 28.1% thought that possible health or environmental hazards are the main motive to stop using dental amalgam. Approximately 94.8% of all dentists would only replace amalgam fillings, which are otherwise satisfactory, in posterior teeth with composite fillings once required by patients, while the rest would prompt their patients to consent removal of amalgam fillings always. Micro-hybrid composites were the most popular composites used by the dentists followed by nanohybrids and bulk-fill composites (Figure 1). The dentists preferred to use resin-modified glass ionomer as a liner in deep posterior cavities under composites. Self-cured calcium hydroxide and flowable composites ranked second and third in the liner choices lists. Etch-and-rinse bonding strategy was employed by nearly two-thirds of dentists. The rest were equally divided between self-etching primers with separate adhesives and self-etching adhesives (Figure 2). Appearance was cited as the main advantage of composite by 85.7% of dentists. Only 20.9% thought composites had better longevity than amalgam restorations, and 9.7% thought composites to be easy to apply. More than two-thirds agreed that composites provide a more conservative alternative to amalgam. Postoperative sensitivity was cited as the main disadvantage of composite fillings in posterior teeth, while 40% of dentists thought it was more challenging to place composites compared to amalgam in posterior teeth. The latter was mainly attributed to inherent sensitivity of composite placement techniques to moisture.
Percentage of dentists who had undergraduate training in aspects related to placement of posterior composite.

Dentists’ preference of composite type used for posterior teeth.

Preference of bonding strategy by dentists included in the study.
Discussion
With the introduction of Minamata Convention, room for amalgam in dentistry is further squeezed. Although the convention identified the need for a transitional period of amalgam phase down, patient demands and the paradigm shift toward minimally invasive dentistry would probably dethrone amalgam, once considered the king of restorative materials. The mainstream dental workforces played a major role in placing amalgam under a gradual reduction “phase down” and not a total ban or “phase out” conditions by the convention.2
Most dental schools in USA and Europe have already made their transition into a “composite focused” preclinical and clinical teaching in operative dentistry.10,11 Although few European countries have already banned dental amalgam, other countries including USA and UK have taken a rather more “reluctant” approach toward the discontinuation of dental amalgam.11 A recent study showed that 47% of restorations placed by undergraduates in USA were amalgam.12 Moreover, 75% of direct restorations placed in molar teeth by general dental practitioners in England and Wales are amalgam.19
Traditionally, resin composites were viewed as a less durable alternative to dental amalgam;20 however, recent studies have shown comparable longevity even after extended years of services.21 This can be attributed to the improved understanding of bonding mechanisms and alleviation of shrinkage stress. Of equal importance is that resin composite is no longer considered as “white amalgam” while preparing cavities and thus more tooth structure is spared.9 This might be challenged by a more recent Cochrane systematic review, which found a low-quality evidence to suggest that composite restorations are at a higher risk of failure and secondary caries.16 The pooled data of this systematic review, based on 7 trials, were all considered at high risk of bias, which might render those findings inconclusive. Amalgam is still considered to be cheaper and less time consuming and technique sensitive during placement in comparison to resin composites. This might leave patients with socioeconomic hardships with less options should amalgam become unavailable to their dentists.2
It can be seen from this study that only a minority of dentists in Jordan know about the Minamata Convention and its recommendations regarding the use of dental amalgam. This might be true for other countries that already signed the convention, thus jeopardizing any effective implementation of the convention. The convention identified a major role for dental schools to provide a preventive-driven training that will reduce the use of amalgam and favor alternatives, including resin composites, over amalgam.1 An Australian focus group study22 has shown that dentists are reluctant to abandon amalgam completely. It was noted that there was a general sense of apathy and resignation among interviewed Australian dentists when asked about the phase down of amalgam.22
Most people will submit to their comfort zones, and dental practitioners are not an exception; they have learnt about dental amalgam, a product in the dental market for more than 150 years. Changing this into composite will require motivation from the dental team, especially from those who have been in practice for more than a few years.10 This study has shown that dentists who have been in practice for more than 15 years were not trained in placing posterior composite. Continuous education might give an answer to provide a satisfactory transition into an amalgam-free dentistry.23 The study also showed that even dentists who belong to young age group are reluctant to embrace the necessary techniques and clinical procedures required when placing posterior composites.18 Previous recommendations were made to allow more room in undergraduate curriculum for teaching posterior composite placement.18 This is now a more pressing issue with the implementation of the Minamata Convention.
A composite-focused learning in undergraduate and postgraduate curricula is challenging when compared to amalgam. When restoring cavities with amalgam, a dentist has to take a few decisions that affect the final outcomes. In contrast, when restoring similar cavities with composite, the treatment algorithms are almost infinite. The tooth preparation method, the etching method, duration, concentration, the bonding techniques,24,25 and the type and method of placement of composite filling,26 all play significant roles in the overall success of the restoration. Using rubber dam isolation and sectional matrices are both viewed as important steps27 when restoring teeth with resin composites, yet they were not incorporated in the undergraduate training of the majority of dentists who participated in this study. Only 10% of surveyed dentists in UK used metal sectional matrix when placing posterior composite although they had been instructed on using them during their undergraduate study. Furthermore, some dental schools are still teaching outdated techniques such as using transparent plastic matrices when restoring proximo-occlusal cavities.11,23 Similar results were noted in this study, in particular with older age group, who were less trained with techniques related to posterior composite placements.
Moving into composite-focused practices is almost certain to happen. To provide a better service to their patients, dentists will need to “amalgamate” their knowledge with best practices available and new advances in materials and techniques. The rapid development of bonding and composite products might render the practicing dentists clueless toward providing the best care for their patients. Evidence-based practice was advocated to prepare dentists and students;11 however, it is yet to answer many questions when related to placing direct restorations.28,29 This might prove to be difficult for Jordanian dentists due to the heterogeneity of products and techniques that are mainly based on commercial data.
In conclusion, taking into consideration the limitations of this study, Jordanian dentists are not well informed about Minamata Convention and the phase down of amalgam. Although they agree with the convention recommendations and the advantages and shortcomings of composite restorations, they are in need for further training in posterior composite placement during their undergraduate study and continuing dental education sessions. The implementation of the proposed changes in undergraduate dental curriculum based on the results of this study might be limited due to financial reasons. Amalgam-free practices will mandate further investment in personnel and equipment.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 22, 2016.
- Accepted October 13, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.