


Abstract
Objectives: To assess health care services provided to type 1 and type 2 diabetic patients and diabetes health care expenditure in the Kingdom of Saudi Arabia (KSA).
Methods: This study was part of a nationwide, household, population based cross-sectional survey conducted at the University Diabetes Center, College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia between January 2007 and December 2009 covering 13 administrative regions of the Kingdom. Using patients’ interview questionnaires, health care services data were collected by trained staff.
Results: A total of 5,983 diabetic patients were chosen to assess health care services and expenditure. Approximately 92.2% of health services were governmental and the remaining 7.8% were in private services. The mean annual number of visits to physicians was 6.5±3.9 and laboratories was 5.1±3.9. Diabetic patients required one admission every 3 years with a mean admission duration of 13.3±28.3 days. General practitioners managed 85.9% of diabetic cases alone, or shared with internists and/or endocrinologists. Health care expenditure was governmental in 90% of cases, while it was personal in 7.7% or based on insurance payment in 2.3%.
Conclusion: Health services and its expenditure provided to diabetic citizens in Saudi Arabia are mainly governmental. Empowerment of the role of both the private sector and health insurance system is badly needed, aside from implementing proper management guidelines to deliver good services at different levels.
The health care system (HCS) in the Kingdom of Saudi Arabia (KSA) is growing at an annual rate of 2% to meet the increasing demand for health care services caused by increased population growth, and a surge in chronic non-communicable diseases.1 This has resulted in an increase in the total health care budget by more than 2 times; from 30 billion Saudi Riyals (SR) (US$8 billion) in 2008 to approximately SR69 billion (US$18.4 billion US dollars) in the year 2011 with a cumulative allocation of SR113 billion (U$30.13 billion) in 2010 and 2011; which accounted for 3.7% of the estimated country’s gross domestic product (GDP), which is one of the highest among Gulf Cooperation Council (GCC) countries.2 The Saudi health care system, which is ranked 26th among 190 countries by the World Health Organization (WHO),3 has a lower percentage of average expenditure in relation to the country’s GDP than many developed and developing countries.4 The government HCS in KSA is structured to deliver free health care services to Saudi citizens through various public hospitals and primary health care centers (PHCCs) including government health sectors, such as the Ministry of Health (MOH), Military Health Services and University Health Institutions. In addition to this, the private health care sector, through its clinics and hospitals, provided 31.1% of the total health care services in KSA in 2013.5 The real challenge facing the Kingdom’s HSC is the increased demands for hospital beds and medical personnel to meet international standards.6 The population ratio of physician and nurses in the Kingdom is lower than the global ratio being 9.4 physicians and 21 nurses per 10,000 of population versus 13 physicians and 28 nurses globally.7 This explains the current imbalance between the growth in HCS and the real medical needs of Saudi citizens.
Diabetes mellitus, being the most prevalent chronic non-communicable disease in the Kingdom, has a significant effect on the country’s HCS and overall economy.8,9 This is proved by the fact that 25.4% of Saudi citizens older than 30 years of age have diabetes, which implies that there are approximately 1.5 million Saudi citizens suffering from this chronic disease.10 This is aside from the fact that more than 70% of known diabetic patients in the Middle Eastern countries have poorly controlled diabetes,11 associated with high rates of chronic complications that place greater pressure on health services and expenditure, where in 2013, it was estimated that the Middle East and North Africa (MENA) region spent US$13.6 billion on diabetes care with the spending per person with diabetes, where the spending in Saudi Arabia was US$934, which is far below other GCC such as United Arab Emirates (US$2,228), Qatar (US$2,199), and Kuwait (US$1,886),12 although we strongly believe that these figures are underestimated.
Diabetic patients are currently managed at all health care levels, from primary to secondary and tertiary levels by general practitioners (GPs), internists, and endocrinologists.13 Since diabetes care involves many medical disciplines, such as ophthalmology, cardiology, nephrology and so forth, specialized diabetes clinics, and diabetes centers are needed to function as liaising bodies. Although health care needs for diabetic patients’ management at a global level have witnessed a clear shift to the primary from secondary and tertiary health care levels,14 diabetic patients in the Kingdom are still receiving services at secondary or even tertiary levels. Since there are no studies so far that have looked into the health care services provided to diabetic patients in KSA, the current study, as a part of the Saudi Abnormal Glucose Metabolism and Diabetes Impact (SAUDI-DM) survey,10 has investigated the current status of health care services provided to diabetic patients. This study aimed to assess the medical system providing care to diabetic patients, and methods of payment through a randomly selected cohort of diabetic patients at a country level.
Methods
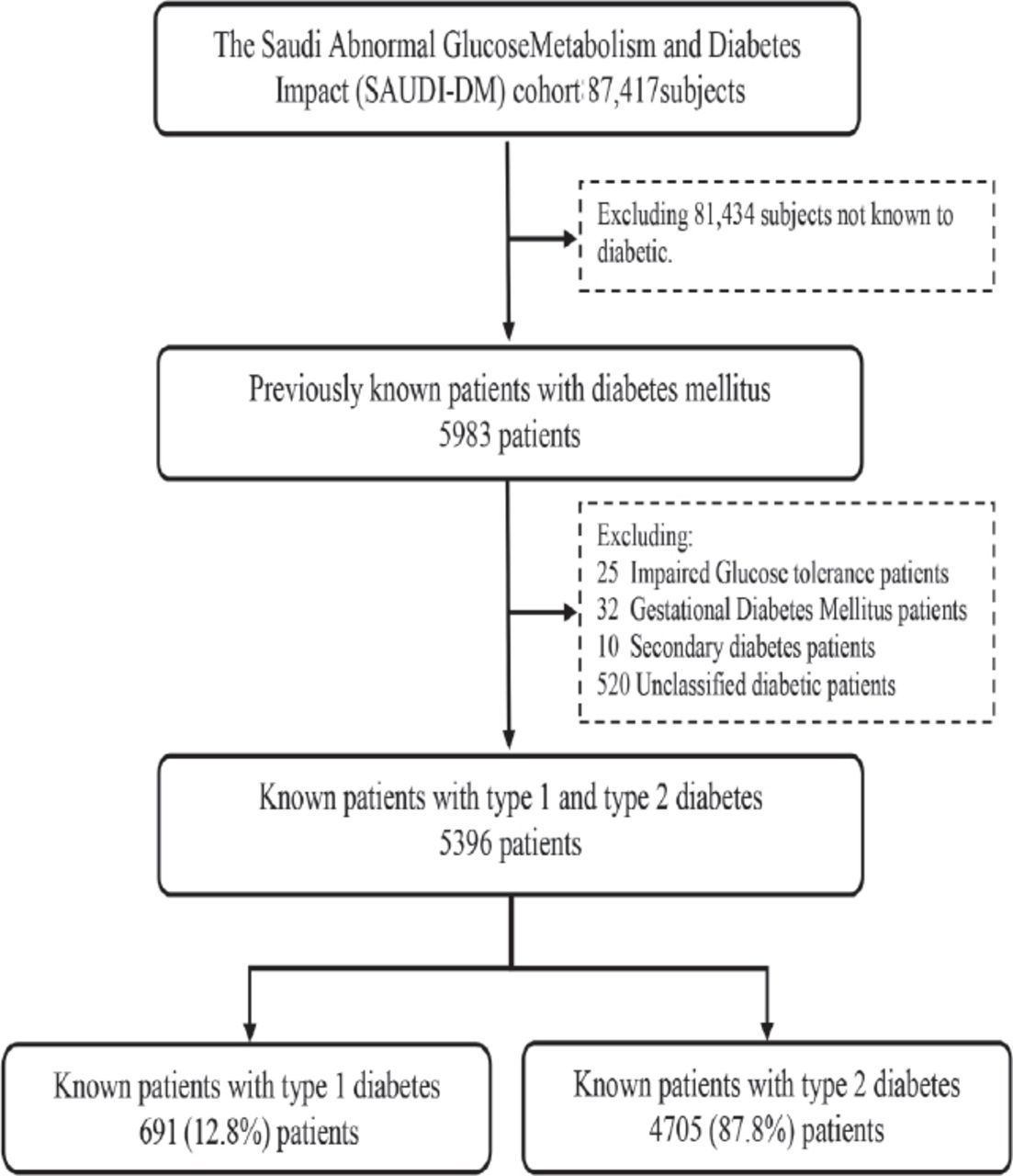
This study is a part of a nationwide, household, randomly selected population based cross-sectional survey covering 13 administrative regions of KSA. A total of 87,417 Saudi nationals participated in this survey conducted at the University Diabetes Center, College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia from January 2007 to December 2009.10 During the research team visit to houses, any diabetic patients who agreed to participate and signed the consent form were recruited regardless of gender, age, and type of diabetes. Previously known diabetic patients that were recruited by this survey totaling 5,983 patients were chosen to assess the health care services provided to diabetic patients in KSA. Since the aim of this study was to assess the health services provided to type 1 and type 2 diabetic patients, 587 diabetic patients were excluded, including 25 patients with impaired glucose tolerance (IGT), 32 with gestational diabetes mellitus (GDM), and 10 patients with secondary diabetes. Another 520 patients were also excluded, since the type of diabetes was unspecified. The remaining 5396 patients formed the eligible study cohort that was used in the current analysis, and further subdivided into 691 (12.8%) type 1 diabetic patients and 4705 (87.2%) type 2 diabetic patients, as shown in Figure 1.

Flow chart of diabetic patients recruited by the Saudi Abnormal Glucose Metabolism and Diabetes Impact (SAUDI-DM) Study cohort.
Demographic data including age, gender, area of residence classified as urban and rural, and educational level classified as illiterate, less than high school and more than high school were collected through a direct interview. The social history of each patient including marital and job status, in addition to the monthly income, were recorded. Relevant clinical data including diabetes duration and type of management classified as insulin, oral anti-diabetic medications or both were included in the pre-designed and pre-tested survey questionnaire.
Data related to health services provided to each patient were collected, including identifying health care sector classified into government and private sectors, and health facilities classified into PHCCs, private clinics, and public or private hospitals. Patients who were receiving health care services from more than one health care facility were identified. Part of this survey was also to identify the medical specialty involved in managing diabetic patients at different levels of care. Patients were asked to identify the medical specialty involved in the management of their diabetes, including GPs, internists and endocrinologists, and to report if they were managed by more than one.
Diabetes related health expenditures in this survey were classified into 6 groups. The first group was related to the outpatients doctors’ visits, whether in PHCCs or hospitals, while the second group was related to laboratory or x-ray department visits for any investigations related to diabetes. The third group of expenditure included the medications related to diabetes management or its complications. The fourth group included hospital admission numbers, and the duration of any admissions related to diabetes or its complications since patients’ diagnosis. Since diabetes expenditure extends beyond hospital services, home glucose assessment using glucose meters and their accessories were included in the expenditure as the fifth group of expenditure. Any other expenditures not included in the previous 5 groups and related to diabetes were classified as others, such as insulin injection tools and alcohol swabs, in addition to nutrition and educational consultations representing the sixth group.
Payment methods were classified into governmental, when the patient received the full services in one of the public facilities regardless of health sector, and personal payments, when these services were paid out from the patients’ pocket. The third mode of payment was classified as insurance for those patients who were receiving their medical care through insurance companies.
This study was approved by the Institutional Review Board (IRB) at the College of Medicine, King Saud University, Riyadh, KSA. The study was conducted according to the ethical standards and the Helsinki Declaration. All adult participating subjects provided direct consent, while children and adolescents who were participating in this study consented through their legal guardian.
Statistical analysis
The design of this manuscript follows the Strengthening Reporting of Observational Study in Epidemiology (STROBE) guidelines. Statistical analysis was performed by the IBM SPSS Statistics for Windows version 21 (IBM Corp, Armonk, NY, USA). Frequencies and percentages were used to represent the data, and plotted as a 100% stacked column chart. The mean ± standard deviation (±SD) values were used to report for continuous variables.
Results
The mean age of the total studied cohort was 55.7±15.0 years, where type 1 had a mean age of 44.8±21.1 and type 2 had 56.2±13.3 years. The overall mean for the duration of diabetes was 8.7±6.5 years, which was longer for type 1 diabetes at 10.4±7.3 years, versus 8.5±6.3 years for type 2 diabetic patients.
Table 1 summarizes the frequency of general and clinical demographic data of the studied cohort, where 77.1% of the total sample was older than 45 years. Type 1 diabetic patients were younger, since 46.9% of this group was younger than 45 years versus 19.4% in type 2 diabetic patients. Males were more frequently present among type 2 diabetic patients (55.3%) compared with type 1 diabetic (51.5%). Approximately two-third of the total type 1 and type 2 diabetic patients were living in urban areas. Illiteracy was observed among 41.4% of the total studied cohort, with only 19.9% having an educational level higher than high school. There were more single type 1 diabetic (27.3%) compared with type 2 diabetic patients (3%), while 28.7% were employed and 32.7% were housewives. When observing their monthly income, 46.5% of the total patients had an income of <4000 SR, while 33.9% had an income ranging between 4000 and 8000 SR, and only 19.6% had an income of >8000 SR. Most patients (41.7%) had diabetes duration of 5-10 years, and it was found to be longer for type 2 diabetic patients (Table 1). Patients’ management showed that insulin use accounted for 21.3%, while 73.8% were managed with oral agents, and 4.9% used both insulin and oral agents. As expected, 92.3% of type 1 diabetic patients were using insulin alone, while 7.7% used sensitizers with insulin. On the contrary, only 9.5% of type 2 diabetic patients were managed with insulin alone, and the rest were treated with oral agents (86%), or by oral agents and insulin (4.5%).
The general and clinical demographic characteristics of the studied cohort.
Most patients (40.3%) were followed up by PHCCs, which was higher among type 2 diabetic patients (41.4%) than in type 1 (33%). Patients were followed up at both PHCCs (39.8%) and public hospitals simultaneously, which was also found to be higher among type 1 diabetic (43.4%) than type 2 diabetic patients (39.2%). Studied patients were followed up at either private hospitals (6.1%) or clinics (1.7%). The mean number of annual doctors’ visits for all patients was 6.5±3.9 visits, which was slightly higher in type 1 diabetic when compared with type 2 patients. Only 8.5% of patients had reported a single visit to the doctor annually, while 35.9% had 2-5 visits and 44.4% had 6-10 visits per year. Patients reporting more than 10 visits per year accounted for 11.2%. The mean frequency of annual patients’ laboratory visits was 5.1±3.9 visits, which was higher among type 2 diabetic patients. Approximately 56.4% of the total cohort had reportedly <5 laboratory visits per year, which was found to be more frequent in type 1 diabetic patients. The mean frequency for hospital admissions was 3.3±2.2 admissions since the diagnosis of diabetes, and was found to be higher among type 2 diabetic patients when compared with type 1 diabetic patients. Of the total studied cohort, 51.7% had 2-5 hospital admissions. The mean hospital admissions duration was 13.3±28.3 days, with no significant difference between type 1 and type 2 diabetic patients. In the total cohort, 56.7% had a duration of admission of less than 7 days and it was found to be more frequent among type 2 diabetic patients at 57.9% than type 1 diabetic patients at 52.8%. The frequency of patients who had a duration of admission of more than 30 days was 8.6% in the total cohort, which was similar in both types of diabetes, as provided in Table 2.
Health care facilities and annual services provided to both type 1 and type 2 diabetic patients.
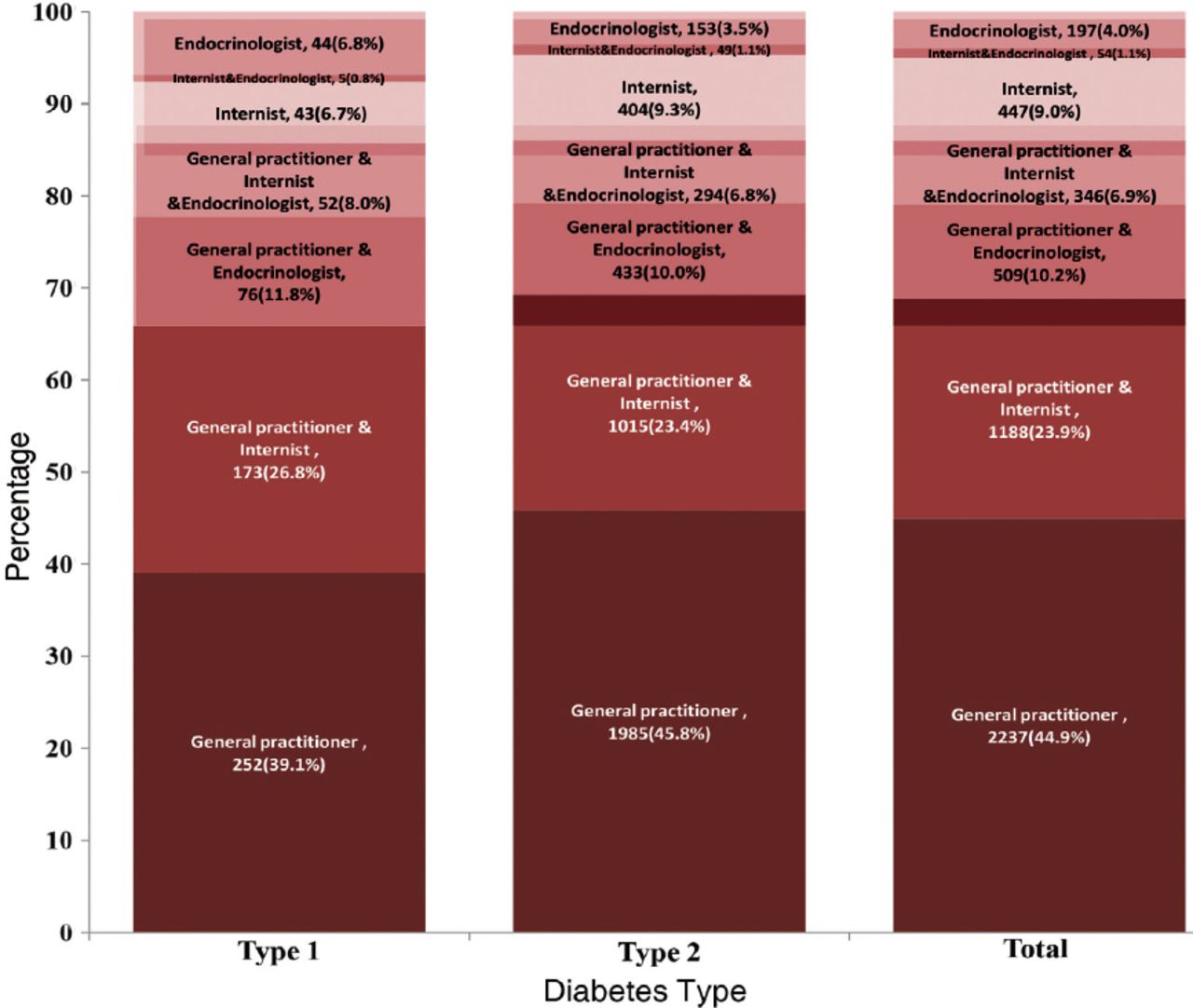
Figure 2 summarizes the 100% stacked column chart for the distribution of the physicians providing diabetic patients with medical care. Herein, the GPs were involved in managing most patients (>85%), either alone (44.9%), or with other specialties (41%). This observation was found to be the same for both type 1 and type 2 diabetic patients. However, more type 2 diabetic patients were followed up by GPs alone, or by internists alone than type 1 diabetic patients (45.8% and 9.3% versus 39.1% and 6.7%). Additionally, a higher percentage of type 1 diabetic patients were followed up by both GPs (26.8%) and internists (6.8%) at the same time, or by endocrinologists alone (23.4%) compared with type 2 diabetic patients (3.5%). The proportions of diabetic patients being followed up by both internists and endocrinologists simultaneously were relatively small, and did not exceed 1.1%, while the role of internists alone in managing type 2 diabetic patients being more frequent than in type 1.

Percentage distribution of health care providers to type 1 and type 2 diabetic patients.
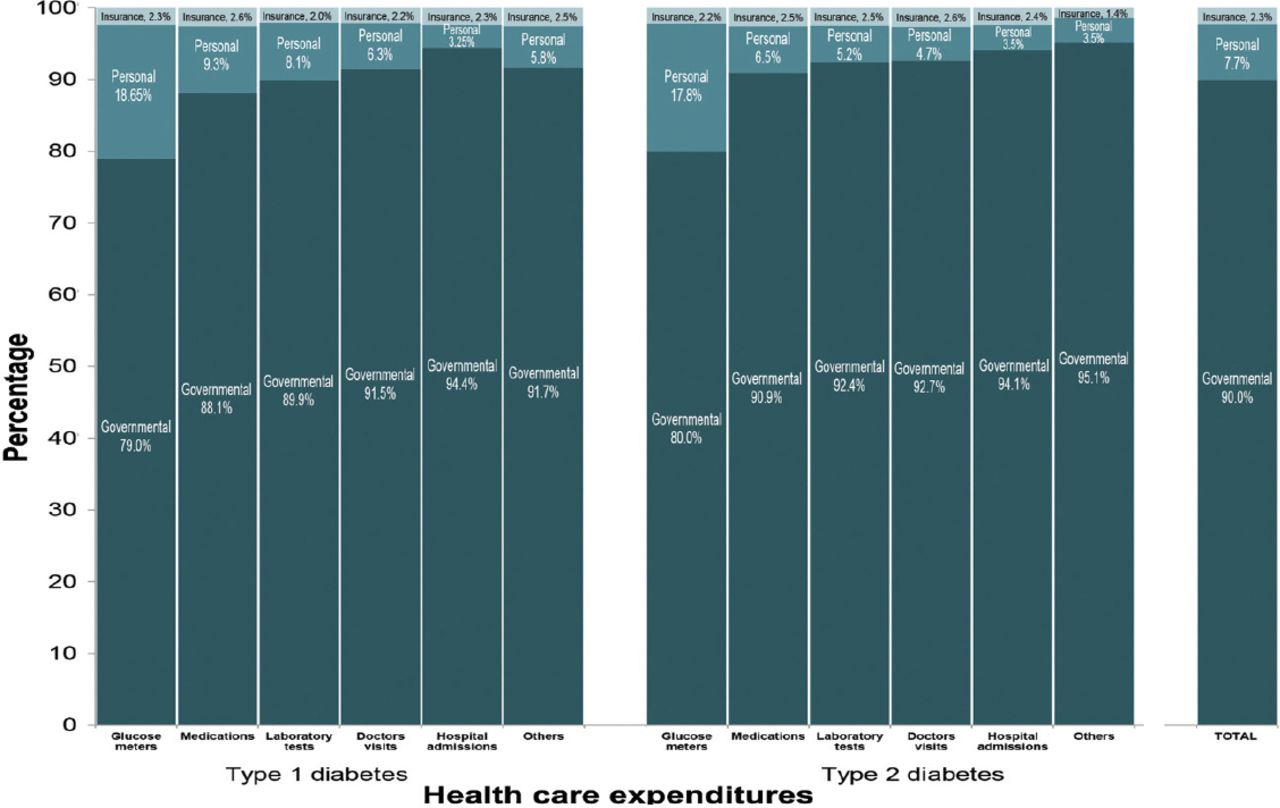
With respect to the mode of payment for medical services, most services provided to the diabetic patients (90%) were government services, whilst the personal payment contributed to only 7.7% and insurance 2.3% only. A higher percentage of governmental mode of payment was also observed in both diabetes types, where it ranged from 79-94.4% for glucose meters and hospitals admissions among type 1 diabetic patient versus 80-95.1% for glucose meters and other services for type 2 diabetic patients. The percentage of the personal payment for all types of services did not exceed 10% in both type 1 and type 2 diabetic patients, except for glucose meters, wherein 18.7% was for type 1 diabetic patients and 17.8% was for type 2 diabetic patients. Health insurance did not play a major role in health expenditure for both diabetes types, wherein it accounted only for 2-2.6% of the total health expenditure among type 1 and 1.4-2.6% for type 2 patients (Figure 3).
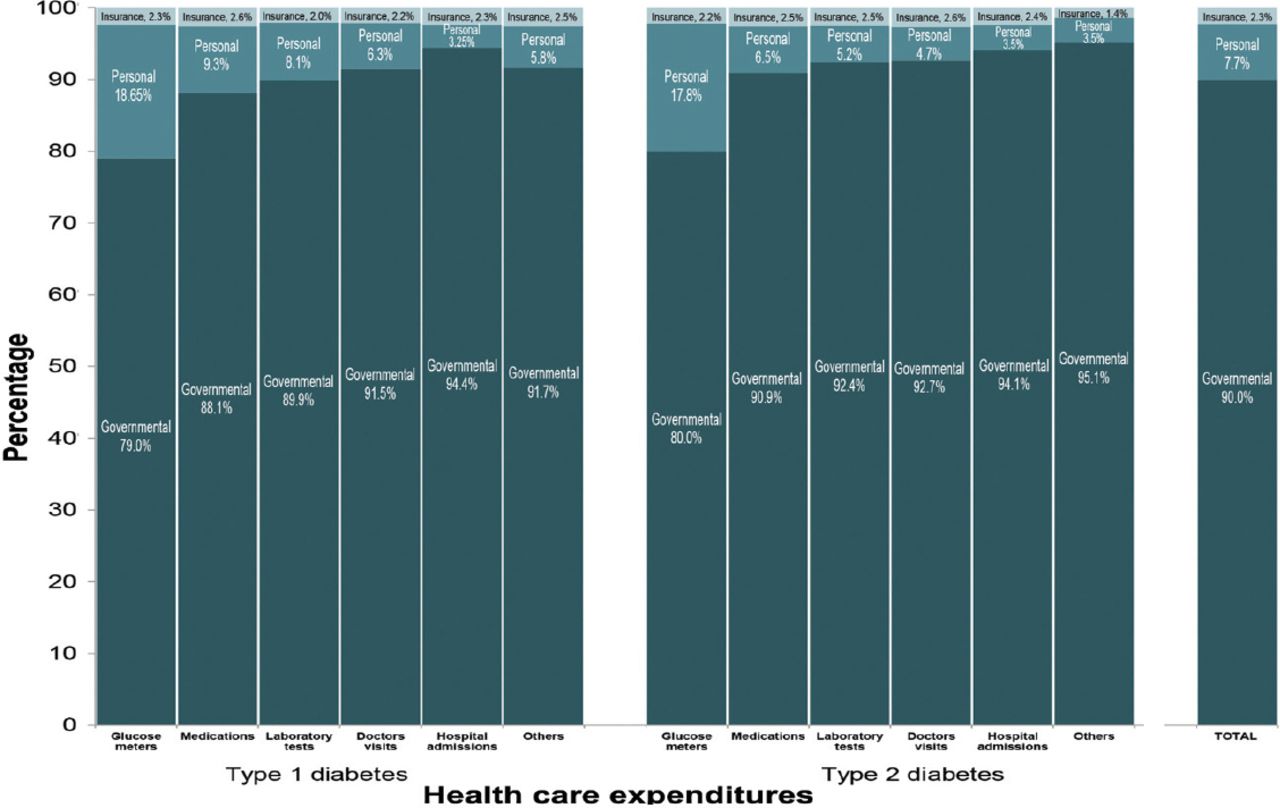
Health care expenditures among patients with type 1 and type 2 diabetes of different health care services.
Discussion
Type 1 and type 2 diabetic patients contributed to 99% of the total diabetic cohort recruited by this epidemiological survey, thereby showing the real impact of diabetes on the health system and economy, since other types are either rare, such as secondary diabetes, or temporary like GDM or has a minimal effect on health services like IGT. Our studied diabetic cohort is representative of the normal Saudi diabetic patients distribution reported from the Saudi national diabetes registry in terms of age, gender, and type of diabetes14 and type 1 to type 2 ratio in the studied cohort correlates with what is known internationally.15
More than 90% of diabetic patients from this survey utilized government health services, which is higher than the regular Saudi citizens, as reported by Al Malki et al3 at 79.8%. This could be explained by the fact that diabetic patients preferred the public health care services due to their wide availability and free services, especially when suffering from a chronic disease, such as diabetes that requires several and frequent services. Primary health care centers provided services to more than 80% of diabetic patients, either alone or with other health care facilities, which could be the result of the policy adopted by the MOH to move health care services for non-communicable diseases from secondary and tertiary levels to primary level,3 in addition to their easy accessibility in both urban and rural areas. Since PHCCs had shown good success in managing communicable diseases, their role in managing non-communicable diseases will have the same success if they are well-equipped and proper diabetes management guidelines are adopted. It should be mentioned that diabetic patients during the course of their disease are in need of specialized medical care including ophthalmology, cardiology, and others, thereby warranting a good referral system. Adopting new technologies would help the GPs in PHCCs to adhere to patients’ management guidelines, and would improve the quality of health care and outcomes as scientifically proven in both developed and developing countries.16,17 This as a result, will have an impact in reducing the burden on public hospitals, as more than 50% of the studied diabetic patients are being managed partially or completely by public hospitals.
In this study, diabetic patients are found to be using out-patients services more than 6 times for doctors’ visits, and 5 times for laboratory services annually, which is close to international standards. However, health care facilities providing these services are below the international standards, which could explain the long waiting list for outpatients and inpatients services provided to Saudi diabetic patients.18 The average doctors’ visit is one visit every 2 months, which is similar to what has been reported in the US,19 but more than what Al-Maskari et al20 reported from the United Arab Emirates.
This survey clearly indicates that both type 1 and type 2 diabetic patients required 3 admissions during their disease time, and since the mean diabetes duration was approximately 8 years, it is expected that Saudi diabetic patients would require at least one admission every 3 years, which is similar to the UK general practice research data base study.21 This is considered to be a high admission rate for a country with high diabetes prevalence, which is most likely related to diabetes complications. Additionally, the long hospital stay exacerbates the situation, especially when this study also shows that the mean duration for admission is more than 13 days. High admission frequency and long hospital stays for diabetic patients poses a significant burden on the Kingdom’s HCS and economy. Implementing secondary prevention programs will reduce the rate of diabetes complications and will help to reduce the frequencies of inpatients and outpatients visits and their related direct and indirect costs.22
General practitioners were the most frequent physicians involved in diabetic patients’ management, and were the only physicians involved in 50% of the cases, while in another 40%, they shared with either an internist or an endocrinologist, or both. This clearly indicates that GPs are the major players in diabetes management in KSA, which is not the case in the US, where GPs manage only approximately 50% of diabetic patients.13 Studies from developed countries have shown that physicians at PHCCs have poor adherence to guidelines for diabetes management, which is also the case here in KSA,22 especially when they are the first line of contact and the more frequently visited physicians by diabetic patients.23 This observation mandates extensive training to increase physicians’ adherence to diabetes management guidelines that would enhance the quality of medical care, as proven by many quality improvement programs.24 Approximately 40% of diabetic patients in this study were treated by internists either alone or with GPs or endocrinologists, which is similar to what has been reported from US.13 Since internists are mostly assigned to secondary and tertiary health care levels with better access to other disciplines, they are in a better position to manage diabetic patients than the GPs. Therefore, it is recommended that the policymakers in KSA should increase the internists’ role in diabetes management. Another 11.3% of diabetic patients received diabetes medical care by the endocrinologists along with either GPs or internists. This indicates that a small percentage of diabetic patients is managed by specialized physicians, which is below the international standards,22 and may indicate a lower number of endocrinologists or a defective patients’ referral system. The role of different physicians in diabetes management has to be empowered by adopting efficient diabetes management programs that would accordingly distribute diabetic patients to the medical specialty levels of GPs, internists, and endocrinologists, especially when more than 50% of patients are poorly controlled, and 30% have diabetes duration of more than 10 years.
The Kingdom of Saudi Arabia is one of the countries that provides free health care service to its citizens.16,18 In this study, approximately 90% of diabetic patients received their health care through governmental institutions, which is significantly higher than what some developing and developed countries are providing to their citizens.25,26 Although this governmental coverage has provided diabetes care at a much larger scale, it has also clearly compromised its quality, as indicated by poor glycemic control and higher rates of diabetes complications.27 On the contrary, health insurance covers only 2% of the total medical services provided to diabetic patients in KSA. This coverage is significantly lower when compared with developed countries and some developing countries.26,28 There is an urgent need to provide health insurance a greater share of the expenses of the governmental health expenditure in KSA. This will result in a positive impact on the quality of health services and overall economy in this rapidly growing population, with increased demand for health care services.
When looking at different services provided to both type 1 and type 2 diabetic patients, governmental expenditure covered most of those services at a variable rate, although approaching 90% with expenditure including hospital admissions, doctors’ visits, laboratory tests, and medications. Contrary to this, personal payment was the highest for glucose meters and its accessories, approximately 20%, which could be the result of the fact that not all government health care facilities provide free glucose meters to diabetic patients, or an improvement in patients’ education, leading to an increased adherence to home glucose monitoring. Policy makers should empower the role of medical insurance providers to transform the Kingdom’s purely public payor system to an insured HCS involving the private sector, and as a result, boosting health care services in KSA.
This study draws its strength from being part of a large epidemiological household country wide cross-sectional survey. Health services data were gathered by a well-trained medical team through direct interviews. Another strength of this study lies in its being community based, rather than hospital based, which provides a real picture of health services countrywide and eliminates any bias. Our study was limited by the nature of the undetailed questions targeting health services focusing on the main services and medical specialties related to diabetes, in addition to being subjective and relying on the patients’ ability to recall information. In addition, there was no correlation between the type of health care provider and clinical outcomes; however, assessing the quality of care provided to the patient was not one of the objectives of this study. Although this study is a country specific, the results may be generalized at a regional level, especially in the GCC countries, where diabetes prevalence is rapidly increasing and the government sectors in these countries are burdened by the majority of healthcare expenses.
In conclusions, most health care services provided to Saudi citizens with diabetes in KSA is free of charge, and provided by different government health care sectors, wherein most services were received in either PHCCs, public hospitals, or both. The private sector has a minor share of diabetes care in KSA, and should be adequately encouraged to face the huge demands in the provision of diabetes health care services. A well planned transformation from governmental to private sector will improve the health care quality, and will have a positive impact on the patients’ health and the overall economy. It is also clear from this study that health insurance contributes to a very small percentage of the Kingdoms’ health care expenditure. Thus, adopting a new strategy of imposing medical insurance will help to provide good health care service delivery to diabetic patients in different health sectors and administrative health regions.
It is also clear from this study that GPs provide health care to most diabetic patients, and henceforth, adopting policies to empower their setup and adopting diabetes management programs will have an impact on the quality of care. Since diabetes is a disease that involves different disciplines in its management, the adoption of a good patient referral system would lead to good primary, and secondary prevention outcomes.
Related Articles
Adherence to the American Diabetes Association standards of care among patients with type 2 diabetes in primary care in Saudi Arabia. Saudi Med J 2015; 36: 221-227.
Measuring adherence rate to quality indicators for diabetes care identified by primary health care in Bahrain. Saudi Med J 2014; 35: 975-980.
Systematic review of quality of care in Saudi Arabia. A forecast of a high quality health care. Saudi Med J 2014; 35: 802-809.
Acknowledgment
The authors would like to acknowledge the team of the Saudi Abnormal Glucose Metabolism and Diabetes Impact study, the staff at the University Diabetes Center for their contribution to the study, and the staff of the primary care centers from the Ministry of Health involved in this study.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This study was funded by the University Diabetes Center, King Saud University, Ministry of Health, and the Tawuniya Company for Health Insurance, Riyadh, Kingdom of Saudi Arabia.
- Received June 11, 2015.
- Accepted August 30, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.