


Abstract
Objectives: To determine the efficacy of preemptive hydromorphone for laparoscopic radical gastrectomy.
Methods: The present prospective and double-blinded study was performed in the The First Hospital, Jilin University, Changchun, China, between July 2017 and April 2018. Fifty patients scheduled for laparoscopic radical, gastrectomy were equally randomized into 2 groups, which were administrated different drugs 10 minutes before surgery. Group P (the preemptive hydromorphone group) was administrated 2 mg hydromorphone (2 mL), and Group C (the control group) was administrated 2 mL normal saline intravenously. A standardized general anesthesia were conducted. Blood pressure and heart rate, postoperative morphine consumption, pain intensity, sedation status, and side effects were recorded.
Results: Group C had larger intraoperative hemodynamic changes, higher postoperative visual analogue scale score, more morphine consumption and lower overall satisfaction degree than Group P. No difference was found between the 2 groups in sedation status and adverse effects.
Conclusion: Preoperative 2 mg hydromorphone could reduce intraoperative changes of blood pressure and heart rate, postoperative pain intensity, and morphine consumption without an increase of adverse effects.
Administrating analgesics before the surgical procedure is called preemptive analgesia, which can decrease central pain sensitization, leading to a reduction in deleterious body reaction to the surgical stimuli and acute pain intensity.1-5 Compared with morphine, hydromorphone may be the ideal intravenous opioid for preemptive analgesia because it is approximately 7 times more potent and has a faster onset, due to its increased lipophilia.6,7 According to previous studies,2,4,5 preemptive opioid decrease hemodynamic changes, pain intensity and morphine consumption without increased side effects. To the best of our knowledge, no comprehensive data have been found with regard to efficacy of preoperative hydromorphone, so we design this prospective, double-blinded, randomized and parallel clinical research to evaluate it.
Methods
A total of 50 patients arranged for laparoscopic radical, gastrectomy for gastric carcinoma were admitted to the study, after we obtained institutional ethical approval (No. 2017-348) and written informed consent from all of the patients. They were equally randomized into 2 groups which received different drugs 10 min before surgery. Group P (preemptive hydromorphone group) was given intravenous 2 mg (2 ml) hydromorphone (Hydromorphone, Yichang Humanwell Pharmaceutical CO LTD, Yichang, China). Group C (control group) was given intravenous 2 ml normal saline. Patients with history of neurological or mental illness, ASA (American Society of Anesthesiologists) more than II, body mass index >30 kg/m2, with liver or renal dysfunctions, pregnancy, who had allergic reaction to the study medicine and were unable to comprehend verbal instruction were excluded. Randomization was conducted with a sequence of numbers generated from the computer program and sealed envelops. A researcher who was not involved in management and assessment of the patients recruited patients and assigned participants to different groups. No other researchers, anesthesiologists, surgeons or patients knew the grouping situation.
Total intravenous general anesthesia was conducted. Intravenous 0.05 mg fentanyl and 4 mg ondansetron were given just before closure of skin incision. After being extubated, all participants received patient-controlled intravenous analgesia (PCIA) by PCIA pumps (ZZB-I, Nantong Apon Medical Appliance CO LTD, Rudong, China), and then were transferred to the postanesthetic care unit. Patient-controlled intravenous analgesia was set at a bolus of 0.015 mg·kg-1 morphine (morphine hydrochloride, Shenyang NO.1 Pharmaceutical CO., LTD, Shenyang, China) on the demand mode with 10 min time-lock.
Blood pressure and heart rate (HR), postoperative visual analogue scale (VAS), cumulative morphine consumption, Ramsay sedation scale (RSS) and adverse reaction were put on record. Pain degree was evaluated with a 11-point VAS (0 indicates no pain and 10 expresses that the worst pain a person had ever experienced). Sedation status was assessed using RSS (1- anxious and agitated; 2- cooperative and tranquil; 3- drowsy but responded to command; 4- asleep but responds to tactile stimulation; 5- asleep and no response). Ramsay sedation scale 5 was regarded as over sedation. If a patient experienced oxygen saturation less than 90%, supplemental oxygen rate was increased, and then he was aroused if sleeping and was asked to take several deep breaths.
Side effects were evaluated and recorded with “yes” or “no” for 48 hours. Patients’ satisfaction degree was assessed with poor, moderate, good and excellent at the completion of the clinical trial.
Decreased postoperative analgesic consumption was the primary outcome of our study. As the sample size was calculated on the base of 20% to 33% decrease in postoperative opioid consumption in previous studies.3-5 Power analysis indicated that 20 patients were required per group with mean difference of 30%, 2-sided α of 5% and β of 20%. For possible dropouts, 25 patients in each group were needed. The secondary outcomes are HR, blood pressure, and side effects.
Statistical analysis was conducted with SPSS 17 (Chicago: SPSS Inc. IL, USA). Patients’ and surgical characteristics, morphine consumption and hemodynamic data between the 2 groups were analyzed using One-Way Variance Analysis. Mean blood pressure (MBP) and HR within the same group were compared with Variance Analysis with repeated measurements. Mann-Whitney U test was performed to analyze VAS scores. Side effects were analyzed with Fisher’s exact test. Patients’ satisfaction degree between the 2 groups was analyzed with chi-square test. P value less than 0.05 was regarded as statistical significance.
Results
No participants were excluded from the study. No differences were detected in demographic and surgical characteristics between Group P and Group C (Table 1).
Demographic and surgical characteristics.
Mean blood pressure and HR changed significantly within Group C. Group C had higher MBP at 5 min after pneumoperitoneum than that in Group P, and higher HR at 5 min and 10 min after pneumoperitoneum than those in Group P (Table 2).
Mean blood pressure (MBP) and heart rate (HR) at different time points.
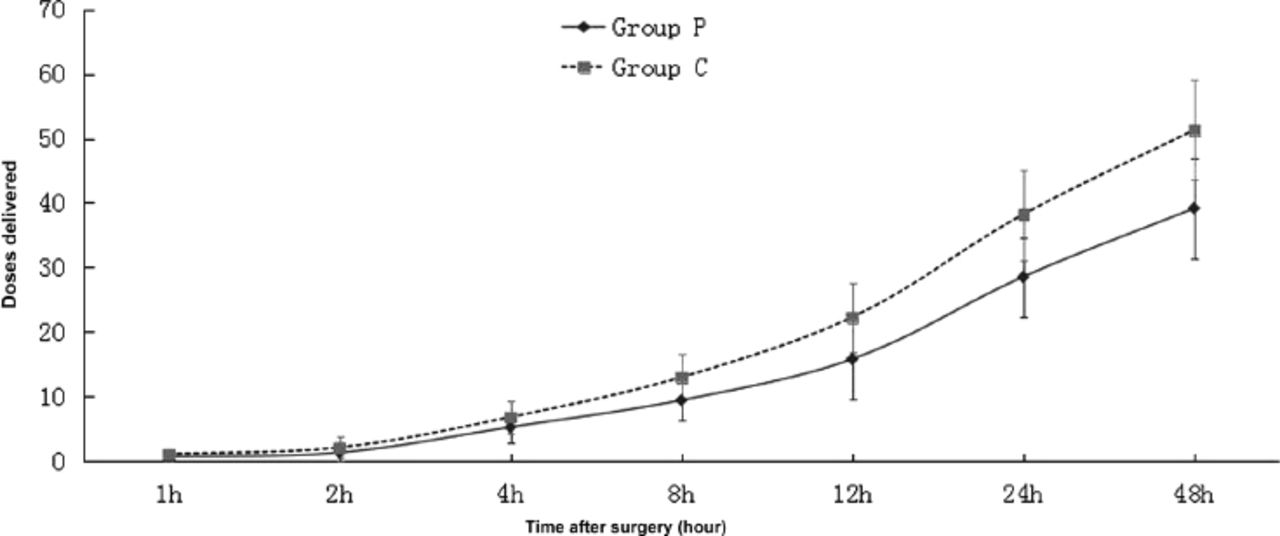
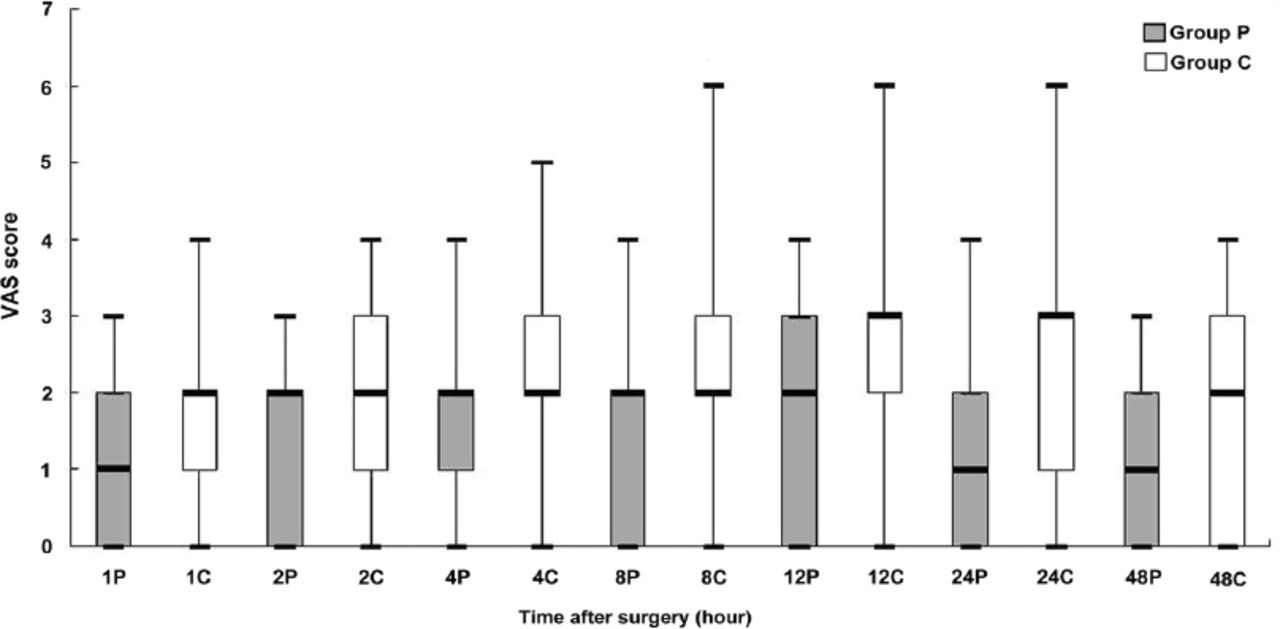
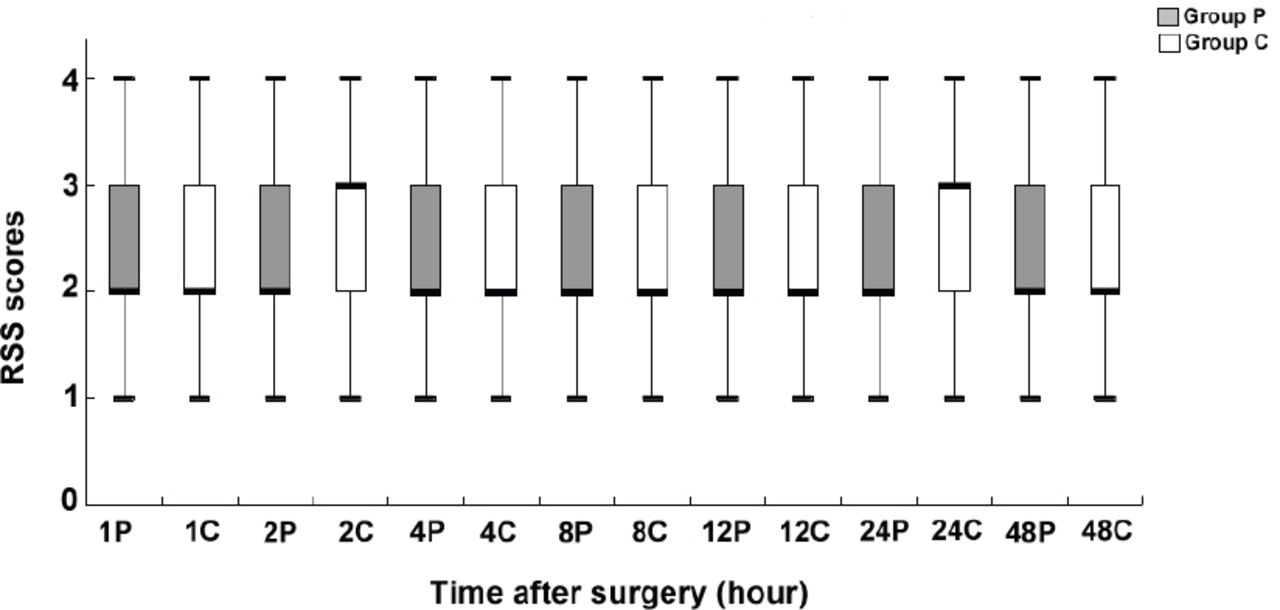
Group C received more boluses of morphine for PCIA and had higher VAS scores than Group P (Figures 1 & 2). There were no difference detected in RSS score between Group P and Group C (Figure 3).

Morphine consumption at each time point. P-values at the same time point between the two groups are displayed as following: 1h, p=0.0229; 2h, p=0.0455; 4h, p=0.0161; 8h, p=0.0025; 12h, p=0.0006; 24h, p<0.0001; 48h, p<0.0001. Group P - preemptive hydromorphone group, Group C - control group.
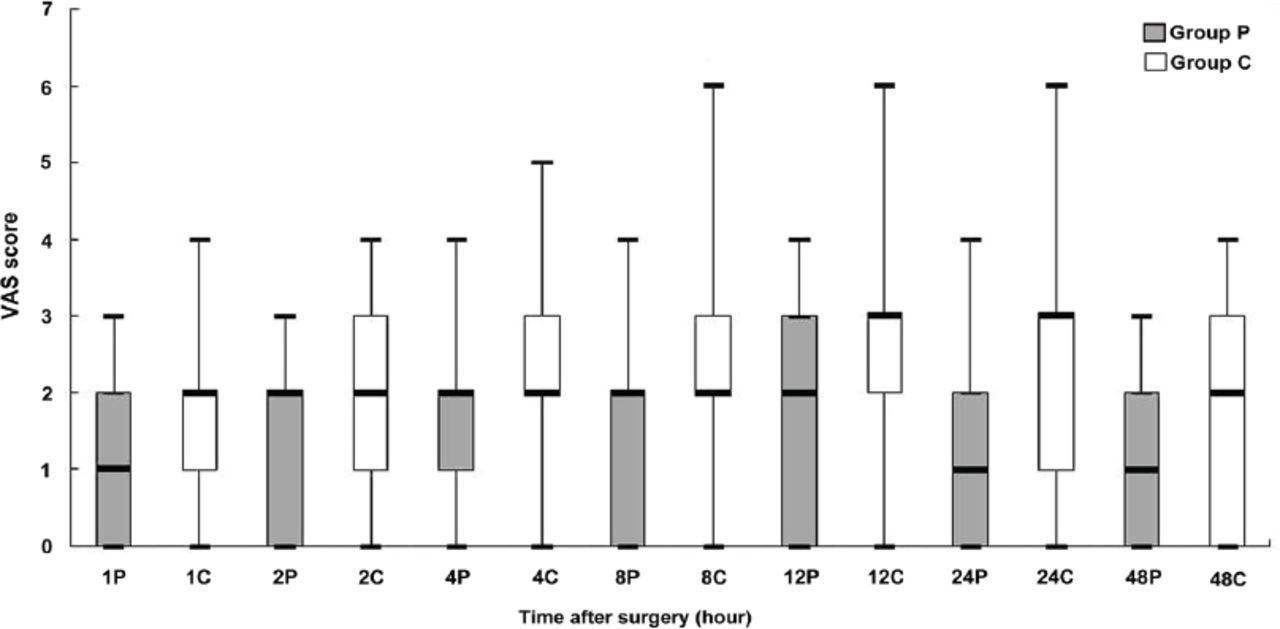
Postoperative visual analogue scale (VAS) score at rest at each time point. The result is displayed in median. The top and bottom of boxes illustrate 75th and 25th percentiles and the error bars maximum and minimum. P-values at the same time point between the 2 groups are displayed as follows: 1h, p=0.015; 2h, p=0.039; 4h, p=0.027; 8h, p=0.026; 12h, p=0.028; 24h, p=0.017; 48h, p=0.019. Group P- preemptive hydromorphone group, Group C- control group
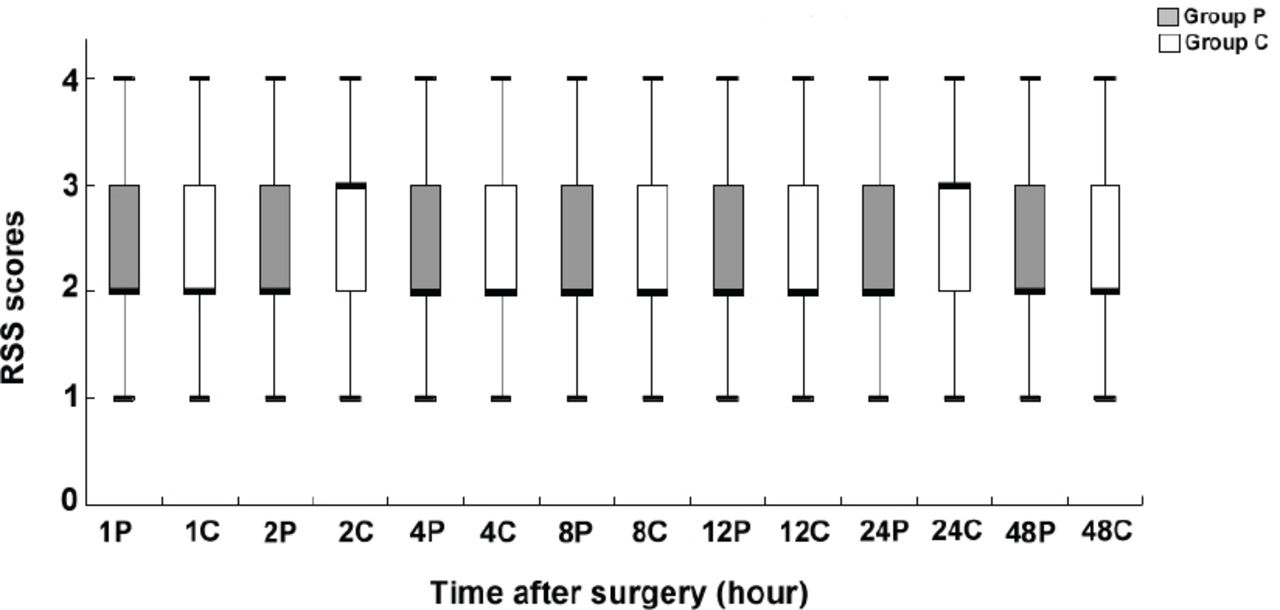
Postoperative Ramsay sedation scale (RSS) score at each time point. The result is displayed in median. The top and bottom of boxes illustrate 75th and 25th percentiles and the error bars maximum and minimum. Group P - preemptive hydromorphone group, Group C - control group. P-values of RSS between the 2 groups range from 0.34 to 0.97.
The incidences of nausea, vomiting, dizziness, pruritis and decreased oxygen saturation (oxygen saturation less than 90%) were similar between Group P and Group C (Table 3). Three patients experienced decreased oxygen saturation. They responded promptly to increased oxygen rate and arousing, and needed no further intervention to maintain their oxygen saturation at 95% or higher. No respiratory depression and over sedation were observed.
Incidences of nausea, vomiting, dizziness, pruritis and decreased oxygen saturation (oxygen saturation less than 90%) were similar between Group P and Group C.
Table 4 showed that Group C had lower satisfaction degree than Group P.
Patients’ satisfaction degree was assessed with poor, moderate, good and excellent at the completion of the clinical trial between Group P and Group C.
Discussion
Preemptive analgesia is analgesic intervention before surgery. It may attenuate or block central pain sensitization caused by surgical stimuli, and then reduce intraoperative stress reaction and postoperative pain.1-5 Hydromorphone, a semisynthetic mu-opioid-receptor agonist, may be more suitable for preemptive analgesia via the intravenous route than morphine, because it is approximately 7 times more potent and has a faster onset compared with morphine, due to its increased lipophilia.6 In addition, hydromorphone is an accepted alternative to morphine because it does not cause release of histamine after intravenous administration and has a lower incidence of pruritis than morphine.6-8 Although there is an argument about preemptive analgesia,9-11 a growing number of studies show that analgesic interventions before surgical stimuli reduce stress reaction, postoperative pain intensity and analgesic consumption.1-5 The result of the current research also supports this opinion, because the hemodynamic changes associated with surgical stimuli, the postoperative pain intensity and morphine consumption can be consequently decreased by preoperative intravenous hydromorphone.
Hemodynamic data are analyzed as body’s response to surgical stimuli during surgery. Patients in the control group have higher MBP and HR. It is implied that patients in the control group respond more strongly to surgical stimuli. It may result from preemptive analgesia of hydromorphone that the preemptive hydromorphone group has lower MBP and HR after pneumoperitoneum than the control group.
Many drugs can provide preemptive analgesia, including opioids,2-5 but there is a concern that the incidence of side effects associated with opioids will increase, because of the synergistic effect of preemptive opioid with intraoperative and postoperative opioids. In this study, the occurrence of side effects associated with opioids is not high in the preemptive hydromorphone group. It may attribute to the decreased postoperative morphine consumption in the preemptive hydromorphone group.
Over sedation is a common adverse effect of opioids, especially after general anesthesia.12 Sedation status is assessed using RSS score in this study. No difference is detected in RSS scores between Group P and C. It implies that preoperative hydromorphone does not affect sedation status which may result from decreased postoperative morphine consumption.
A study by Chang et al13 shows that one third patients who receive 2 mg intravenous hydromorphone develop decreased oxygen saturation in the emergency department. But in our study, no serious side effects including central nervous system depression (over sedation) or respiratory depression are observed. The reason may be that the adverse effects of preoperative hydromorphone are covered by following anesthesia.
Although hydromorphone has demonstrated evidence of preemptive analgesic benefit, there are limitations about our study. More studies need to be carried out to evaluate the effect of preemptive hydromorphone on hemodynamics. We failed to follow up to assess if chronic pain has been reduced by preoperative hydromorphone. We will focus on the long-term effect of preoperative hydromorphone and how to reduce postoperative side effects in the future research.
In conclusion, this study suggests that preoperative 2 mg hydromorphone can influence hemodynamic changes and decrease pain intensity and morphine consumption for PCIA in patients undergoing laparoscopic radical, gastrectomy without increased side effects.
Acknowledgment
We would like to thank the Information Engineering Research Institute, Changchun, China for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 23, 2018.
- Accepted August 13, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.