


Abstract
Objectives: To estimate the prevalence of post- amputation pain among lower-limb amputees and its burden on their lives.
Methods: A retrospective patients record review of lower limb amputation surgeries was carried out at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, between 2008-2019. e collected data included: patients demographics, surgical operations, chronic pain characteristics, functional impairment, and treatment.
Results: A total of 645 lower-limb amputations carried out on 509 patients, 104 (20.4%) patients had more than one amputation surgery carried out, and 40 (7.9%) patients having bilateral amputations. The estimated prevalence of chronic post-amputation pain among the lower-limb amputees was approximately 61.5%. Persistent postoperative neuropathic pain was the most common type of pain following amputation, followed by residual limb pain, then phantom limb pain. The most common cause of amputation was diabetes and its related complications (76%). The mean age at surgery was 57.46±12.02 years. Although diabetes was a common comorbid illness (95.6%), it had no correlation with the development of chronic post-amputation pain. However, peripheral vascular disease had a strong association (p=0.009), especially with the development of phantom limb pain (54.5%; p=0.016). The most common reason for functional impairment among the amputees was disability (52.7%), while only 6.6% said it was secondary to pain.
Conclusion: Post-amputation pain is one of the major consequences of amputation. Pain was poorly managed among these patients. Special considerations should be obtained to manage these patients’ pain and reduce their suffering.
Amputation has been known since the dawn of mankind. Post-amputation pain (PAP) is one of the major consequences of amputation that challenge pain physicians.1 Limb amputation is only carried out when no other possible treatment option will save a patient’s life. Limb amputations are carried out for various reasons, ranging from vascular diseases, serious infections, tumors, and traumas to congenital malformations. A meta-analysis showed that more than 50% of amputations were due to diabetes or vascular etiologies. Vascular insufficiency amputees have a 27-44% risk of contralateral limb amputation after 4 years.2-5
Diabetic patients are more exposed to complications that might lead to lower extremity amputation than are nondiabetic individuals. With the prevalence of type 2 diabetes in Saudi Arabia ranging from 18.2% in the Eastern province to 31.6% in the Central region, the rate of amputation increases significantly.6
Limb amputation can lead to painful and non-painful conditions. The painful consequences can be classified as phantom sensation, phantom limb pain (PLP), and residual limb pain (RLP; previously known as stump pain).5,7 Phantom pain is the perception of unpleasant sensations in the nerve distribution of the missing body part. It has been reported to occur in 47-79% of post-amputation patients.7-14 Residual limb (stump) pain is pain localized in the residual body part following amputation. Recent studies have reported an incidence of RLP of 32-93% with long-duration follow-up.7-11,14-16
There are many hypotheses on the development of PAP among amputees, but most of them fail to refer a certain mechanism or factor. However, many experts believed that there are 3 major mechanisms that might cause these phenomena: the peripheral mechanism, the central neural mechanism, and the psychogenic mechanism.17
The aims of this study were to estimate the incidence of post-amputation pain among individuals who have had lower-limb amputation surgeries in a sample of local residents; determine the effect of sociodemographic factors, habits, and illnesses on the development and the severity of PAP; find any correlation between preoperative pain and the development of PAP; and identify the characteristics of such pain.
Methods
The medical records of 509 patients who underwent lower-limb amputation in the period between January 2008 and December 2019 were identified from the hospital information system after the approval of the Ethics and Research Committee at King Abdulaziz University Hospital, Jeddah, Saudi Arabia (Reference no 85-19) on February, 2019. Data related to amputation, phantom limb sensation, and post-amputation pain were recorded. The study was carried out in accordance with the principles stated in the Declaration of Helsinki.
All adult patients who underwent lower-limb amputations and were aged 18 years or older at the time of surgery were included in the study. Perioperative variables were recorded, including demographic data, associated medical diseases (comorbidities), body mass index (BMI), surgical data, reason for amputation, level and side of amputation, intraoperative nerve ligation, type of anesthesia used, pre- and post-amputation pain, used medications, physical therapy consultation, and referral to other specialties.
We carried out a phone call interview with each subject to assess the occurrence of phantom limb or pain, persistent postoperative pain, residual limb pain, and any neuropathic pain. One of the research team completed a 6-page questionnaire adapted and modi ed from Kooijman et al18 phantom pain questionnaire, Wartan et al8 phantom pain sensation 4-page amputee questionnaire, and a modified DN4 questionnaire.19 The physical examination part of each questionnaire was not included in the interviews. Each patient’s agreement to complete the questionnaire was considered a consent to participate in the study. Patients were excluded from the study if they refused to participate in the study.
The study questionnaire covered various aspect of the patient’s life: sociodemographic data, functional assessment, smoking habits, the presence of pain and its duration before the amputation, the complaint of residual limb pain, phantom limb pain, or persistent postoperative pain, the characteristics and the severity of pain, and its effect on daily activities, treatment options, and surgical data.
On an 11-point numerical scale, pain was assessed by asking the patient to rate the severity of their pain, where 0 was no pain and 10 was the worst imaginable pain. Participants were also asked if they had ever consulted a physician regarding their pain, treatment modalities they had received, their satisfaction with the treatments provided, and how they cope with their pain.
Statistical analysis
Data was entered into a Microsoft Office Excel spreadsheet. Statistical analysis was carried out using Statistical Package for Social Sciences for Windows, version 22 (IBM Corp., Armonk, NY, USA). Numerical variables were presented as mean and standard deviation, or frequency and percentage. The Chi-square test was used to test the independence of row and column variables, without indicating the strength or direction of the relationship. Pearson Chi-square and likelihood-ratio Chi-square, Fisher’s exact test, and Yates’ corrected Chi-square were computed for 2x2 tables. The prevalences of post-amputation pain syndromes among all lower-limb amputees were calculated. The numbers of specific pain-syndrome patients were divided by the total number of amputees and then multiplied by 100 to find the percentage. P-value of <0.05 were considered significant.
Results
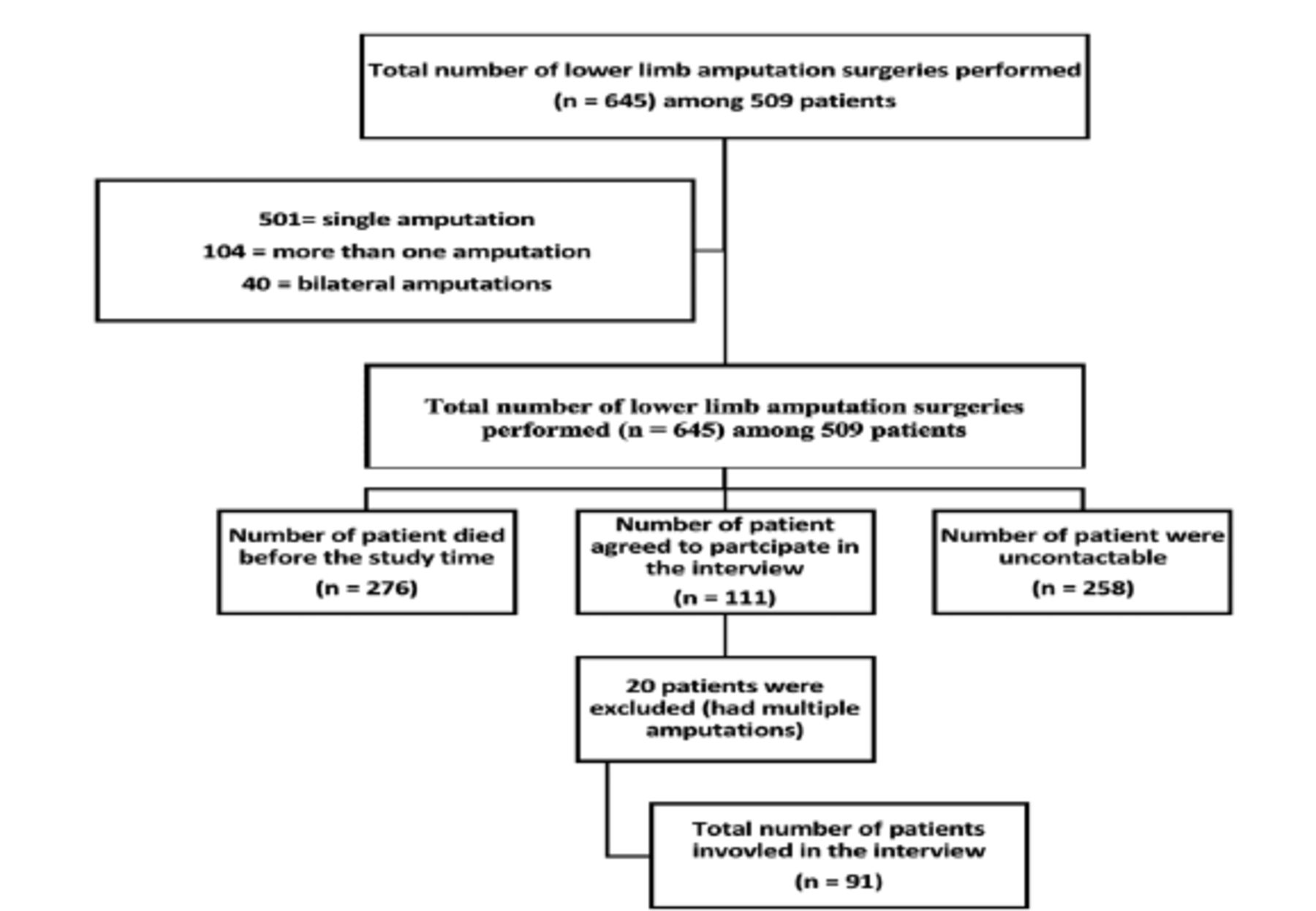
A total of 645 lower-limb amputation surgeries were carried out at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, including: 2 (0.3%) hip disarticulations, 271 (42%) above-knee amputations (AKA), 230 (35.7%) below-knee amputations (BKA), 21 (3.3%) foot amputations, 33 (5.1%) forefoot amputations, and 88 (13.6%) toe amputations from January 2008 until December 2019. Of the 509 patients who underwent the 645 amputation surgeries, 104 (20.4%) patients had more than one amputation surgery, and 40 (7.9%) had bilateral amputations. e most likely reason for amputation was related to diabetes complications and diabetic foot (76%).
Each one of the 645 amputation surgeries was considered as an individual patient. The mean age at surgery was 57.46±12.02 years, and 458 (71%) patients were male. There were 198 surgeries carried out on Saudis (30.7%) and 447 on non-Saudis (69.3%; Table 1).
- Patients demographic data (N=509).
At the time of the interview, 276 patients had died, 258 patients were uncontactable, and 111 patients were alive and agreed to participate in the study. There were 20 patients subsequently excluded from the final analysis because they had multiple amputation surgeries carried out on the same limb. The final level of amputation was included in the research. A total of 91 cases were finally included in the study (Figure 1).
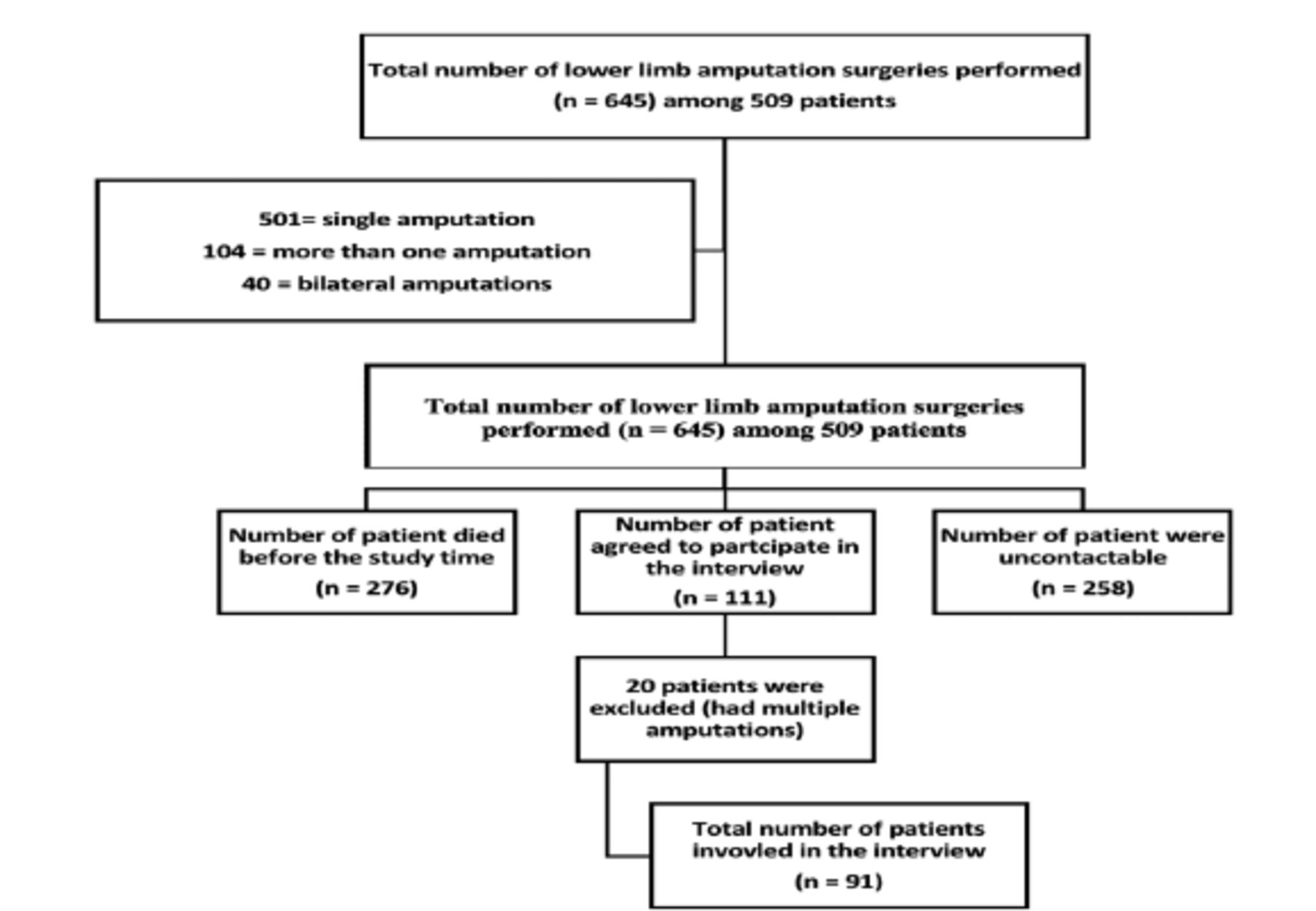
- STORB flow chart of participants.
The patients’ age range was 34-85 years, with a mean age of 57.46±12.022 year. Of those, 56 (61.5%) patients were suffering from post-amputation pain, 22 (24.2%) experienced PLP, 28 (30.8%) experienced RLP, and 33 (36.3%) had symptoms suggestive of persistent postoperative neuropathic pain. A total of 35 (38.5%) were pain free, 14 (15.4%) had phantom pain without RLP, and 8 (8.8%) had both PLP and RLP concomitantly. There was no significant association found between PLP and RLP ( χ 2=0.418; p=0.518).
Patient’s age was significantly associated with the development of chronic post-amputation pain (p=0.03), with the highest incidence in the group aged 61-70 years (35.7%), while the young adult group (31-40 years) developed one or more types of chronic post-amputation pain (14.3%). There was no relation between the occurrence of post-amputation pain and gender, nationality, marital status, BMI, or educational level. However, there was a positive association between patient’s complaints of comorbid diseases and the development of chronic post-amputation pain. Diabetes (95.6%), though it was a common comorbid illness, did not have a statistically significant relation with the development of chronic post-amputation pain. Only 32 out of 61 diabetic patients developed post-amputation pain, despite 67% of the 91 patients having their amputation due to diabetes complications and diabetic foot. Peripheral vascular disease (PVD) had a statistically significant association with the development of post-amputation pain (p=0.009), particularly PLP (54.5%; p=0.016; Table 2).
- Post amputation pain in relation to demographic, surgical, and comorbidity data (N=509).
The number of people who were still employed after the amputation was 12 (13.2%). Of the rest, 8 (8.8%) were homemakers, and the rest were retired (23.1%), unable to work (45.1%), or unemployed but seeking jobs (9.9%). Most of them (52.7%) blamed their functional impairment on the disability resulting from amputation, while 6.6% said it was secondary to pain. The remaining 40.7% denied any functional impairment.
The overall ambulatory rate was 45%, including 18.7% utilizing a prosthesis, and 15.4% depending on walking aids. There were 50 (54.9%) bound to a wheelchair or bed. Surprisingly, 6 of the 12 bed-bound patients were of normal weight. There was no significant association between BMI and ambulatory status.
In all, 40.9% of PLP patients and 25% of RLP patients were referred to Physical therapy and Rehabilitation Department after their amputation. Such referral had no significant effect on the development or chronicity of post-amputation pain (p=0.15).
Most of the amputation patients (71.4%) experienced RLP with a duration of less than a year. Among them, 46.4% described the pain as moderate, and 50% stated that they experienced RLP a few times a day. Approximately 75% related its worsening to activity. Half of the patients (50%) were able to sleep comfortably and 35.7% were awakened from their sleep by RLP. On the other hand, 14.3% could not sleep because of the pain. Approximately 50% stated that RLP limited their ability to work, while 25% said it affected their leisure activities. Only 7.1% needed a caregiver, and 78.6% received treatment with equivocal satisfaction.
Residual limb pain was significantly associated with smoking, but it was unrelated to comorbid conditions, indications for amputation, intraoperative nerve ligation, or prosthesis use (Tables 3&4).
- Residual limb pain characteristics (N=509).
- Residual limb pain in relation to comorbidities and amputation.
Regarding phantom pain, 13.3% started to have PLP within therst 24 hours after the surgery, 27.3% of patients developed PLP within one week after the amputation, and an equal number within 3 months of the amputation. There were 18.2% who developed PLP one year after the amputation.
Most patients (59.1%) reported that their PLP was constant over time. Meanwhile, 36.4% reported that the pain decreased greatly. Only 4.5% had more pain as time passed, 31.8% experienced phantom pain a few times a week, and 13.6% suffered constant PLP. Approximately 50% reported pain lasting for seconds, while 40.9% said it would last for hours. There was no difference in terms of severity, with 36.4% experiencing severe phantom pain. For 27.3% the phantom pain originated from multiple sites; 45.5% of times at the toes followed by the legs (40.9%), and less frequently from other sites.
Most patients (45.5%) reported no limitation in activity due to PLP, while 18.2% reported the need for a caregiver. Approximately 50% of PLP sufferers could sleep comfortably, and 31.8% reported inability to sleep. Among PLP sufferers, 45.5% had received medical treatment for PLP, and 60% were satisfied with the treatment. No significant association was found between PLP and perioperative factors, ambulatory status, or prosthesis use (Tables 5&6).
- Phantom limb pain characteristics.
- Phantom limb pain in relation to comorbidities, and amputation
Of all patients suffering from PLP, RLP, or persistent postoperative neuropathic pain, only 24 (42.9%) received medical treatment for pain management, 30.4% consulted their surgeons regarding their pain, and 2 underwent re-amputation of the amputation stump. Only 4 (7.1%) consulted a pain specialist, and 3 had lumbar sympathetic block, with one patient proceeding with lumbar sympathectomy with pulsed radio frequency. Only one patient received local anesthetic with steroid injection at the stump and another one received an infusion of intravenous lidocaine. Of the patients suffering from PLP, 55.6% had no coping method, and among of those with RLP, 42.9% had none. Reliance on analgesics was reported by 22.2% of those with PLP and 28.6% of those with RLP. None had tried tranquilizers or alcohol. Of the 24 who received medical treatment for phantom or RLP, 70.8% used acetaminophen, 37.5% used anticonvulsant drugs,
29.2% used non-steroidal anti-inflammatory drugs (NSAIDs), and 12.5% used antidepressants or opioids. Tramadol was not prescribed to any patient.
Discussion
The main finding of our study was the high frequency (61.5%) of post-amputation pain among lower-limb amputees. This is similar to the findings. of other studies in which it ranged from 47-79%.4,7,8 Persistent neuropathic pain was the most common type (15.4%), followed by phantom pain (11%), and RLP (9.9%). The prevalences of all types of PAP pain were much lower than those reported among Western populations.3,4,8-12,17,20 In this study, the most common cause of functional impairment was disability (52.7%) while only 6.6% considered PAP as a cause. Besides, 45% were mobile with a prosthesis or walking aid. This is opposite to the finding of Karns Schreuder et al21 who reported that lower-limb pain had a negative impact on the quality of life, particularly among post-amputation patients who have undergone prosthesis placement, while Davie-Smith et al22 in a systemic review found that the ability to walk with a prosthesis had a positive impact on quality of life. However, trans-femoral amputation has led to difficulty in using a prosthesis and in walking.
The average age of our patients was 57±12 years, similar to previously published data from both the United States (50.3±13.3 years) and Singapore (62 years), while young and middle age were common age categories for amputation in other studies.7,9-11,23 Gallagher et al11 have reported that old age was associated with higher prevalence of severe PAP, while we could not find any correlation with age in our study. Although smoking was considered in many epidemiological studies to be a risk factor for amputation, a relation to amputation was not found in our study.24-26 Surprisingly, our study showed that smokers experienced less RLP when compared with non-smokers. The small sample size and the lack of information regarding the duration of smoking might have contributed to this finding. Further studies are needed to assess the relationship between smoking and the risk of amputation in Saudi Arabia. Most of our patients were males, but we could not detect any significant association between PAP and gender. Similarly, nationality, educational level, and obesity have no relation to the incidence of PAP. AlNozha et al27 epidemiological survey of 16917 Saudi patients revealed that diabetes was the most common among males than females, and this might help to explain the higher number of males in our sample. Further studies are needed to clarify these findings.
Peripheral vascular disease was associated with a high rate of amputation and PAP in this study. Finch et al28 reported the same finding in their study, where 30% of the PAP was the result of vascular insufficiency. Diabetes and PVD are coexisting morbidities of old age, which might contribute to this sequel.
Diabetic complications were the main reason for lower-limb amputation in our study. This is similar to the findings of previously published studies, in which diabetes and peripheral arterial disease were present in 75.6%, while tumor and trauma were the main indications for lower-limb amputation among Caucasian patients.7-14,16,29 Similar to the findings of Gallagher et al11 in which AKA was associated with a higher incidence of PAP but the increase was not statistically significant. In our study, we found that preoperative pain had no correlation with the incidence of PAP, contrary to the findings of many other studies.14,30-33 The retrospective design of our study and its reliance on patient’s memory might have led to this finding. Further studies are needed to test for this correlation among the local population.
The majority of those who had experienced RLP complained of pain for a period shorter than a year, and 46.4% had moderately severe pain. Approximately 50% were able to sleep comfortably, while the remaining 50% complained of lack of sleep. Post-amputation pain and the impaired quality of life might lead to this disturbance of sleep, according to the findings of Yin et al.34
Although not perfectly illustrated due to the limited sample size, we do believe that an increase in the verbal analogue scale score for phantom pain was more commonly associated with amputations carried out above the level of the knee and those below the level of the ankle, as shown in prior studies in which PLP was more likely to occur with proximal amputations than with distal amputations.34-38 Proximal amputations are associated with more risk of delayed wound healing, infection, and development of stump pain.39
Managing PAP is a challenging situation, as many mechanisms were involved in the development of PAP.40 ere are many groups of medications recommended to treat PAP, paracetamol and NSAIDs are not commonly used among them.1 The high use of these medications might be related to the limited knowledge of the treating surgeons about the available medications, or the unfamiliarity of these surgeons regarding the proper treatment of neuropathic component of pain. Further studies are needed to assess the reasons behind improper treatment of PAP. Although pain clinics are specialized and experienced in dealing with such medical problems, the number of patients suffering from chronic PAP who have reported to the pain clinic was as low as 3.6% among our patients. The complexity of PAP necessitates an interdisciplinary team that includes a pain specialist to look after the patients. The unfamiliarity of the treating doctors with pain specialty might contribute to the current situation. Further clinical trials are needed to assess the role of pain medicine in treating PAP.
Study limitations
The small number of patients agreed to participate in the interview as it might lead to enormously biased result (high nonresponse bias). In addition, the retrospective nature of the study and the reliance on patient’s memories are other limitations of our study. Although our study provides good amount of information regarding PAP among the Saudi population, but we cannot generalize the results on other centers or cultures.
In conclusion, despite the small sample size, PAP is a major consequence of amputation with a significant impairment of the patient’s life. Prospective well- designed studies are needed to prevent the need for amputation and control PAP.
Acknowledgment
The authors gratefully acknowledge San Francisco Edit (www.sfedit.net) for English language editng.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 4, 2021.
- Accepted December 7, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.