


Abstract
Objectives: To measure the self-awareness of hemoglobin A1c (HbA1c) prevalence among type 2 diabetic Saudi patients and its association with glycemic control, thereby identifying those factors that might affect their glycemic control.
Methods: This multicenter study was carried out in outpatients’ diabetes clinics in tertiary hospitals in Riyadh, Qassim, and Jeddah, Saudi Arabia. The data was collected using questionnaires. The subject’s self-awareness on the HbA1c test was assessed based on the combined score of 4 questions. The latest HbA1c result before the time of data collection was obtained from medical records. Data was analyzed using bivariate and multivariate statistical methods.
Results: The prevalence of HbA1c self-awareness was approximately 44.5%. A total of 4 participants characteristics (glycemic control, education level, monthly income and number of follow-up visits) were associated with awareness of HbA1c. Whereas for better glycemic control; type of treatment, duration of diabetes, and self-awareness of HbA1c were independently statistically significantly associated.
Conclusion: There is a positive association between HbA1c self-awareness and glycemic control. Glycemic control was good among those who were educated on the meaning of the test, their levels, and their target goal. Awareness among health care providers regarding the role of the patient’s education regarding their condition might help in providing the patient with optimal care. Further studies with different experimental designs are needed to study this association, which will contribute to the development of a structured educational program.
Type 2 diabetes mellitus (DM) is one of the most common chronic non-communicable diseases. Diabetes mellitus is characterized by hyperglycemia due to the inadequate production of insulin or the lack of capability of the body’s cells to respond to insulin, a condition known as insulin resistance.1 Its prevalence has increased globally, which has added to the burden on healthcare resources. According to the International Diabetes Federation, the worldwide prevalence of diabetes was 463 million in 2019 and is expected to rise to 578 million adults with diabetes by 2030, and 700 million by 2045.2 Locally, it was estimated that 23.7% of Saudi adults have been diagnosed with diabetes.3 Maintaining good glycemic control is considered the primary goal of diabetes management.4 Good glycemic control carries the benefits of improving a patient’s quality of life and preventing or delaying its harmful complications.5 These complications include microvascular (nephropathy, neuropathy, and retinopathy) and macrovascular (cardiovascular and cerebrovascular disease) complications.6 The hemoglobin A1C (HbA1c) test is one of the most important biomarkers for assessing glycemic control and has been approved by the World Health Organization (WHO) for diagnosing diabetes and monitoring glycemic control.7-9 The HbA1c test carries the advantages of being measured at any time without the requirement for fasting. Another advantage is that the HbA1c test can be used to reflect the average blood glucose level over the previous 3 months, which makes it the best option for the long-term management of type 2 DM.8 Suboptimal control of HbA1c can lead to the development of harmful acute or chronic complications and an increase in the risk of developing cardiovascular disease by 2-3 times and end-stage renal disease by 10 times in patients with DM when compared with those who do not have DM.10 Diabetic peripheral neuropathy can affect from 16-66% of all people with DM while more than one-third of these can be affected by diabetic retinopathy.2,11 These problems can be attributed to many causes, such as patients who remain undiagnosed for years due to lack of symptoms. Several studies have shown a high proportion of patients who have poor glycemic control worldwide despite the great efforts that have been made to control their diabetes and manage their modifiable risk factors.12-15 Although many studies have aimed to evaluate the factors associated with good glycemic control, there is a lack of studies that evaluate the unusual factors related to suboptimal control, such as patients’ self-awareness of their own glucose levels and HbA1c as a part of self-care behavior.16 Although much research has shown favorable effects of structured education concerning HbA1c and glycemic control, only few Saudi studies have been carried out to address the relationship between the extent of self-awareness of HbA1c and glycemic control. An important gap in the local literature exists and needs to be addressed, especially because Saudi Arabia represents a different culture and healthcare system than what is found in other countries, and it has a high prevalence of DM. The main objective of this study was to measure the prevalence of HbA1c self-awareness and its association with participants’ glycemic control.
Methods
This study was a cross-sectional survey using an interview questionnaire to investigate the prevalence of HbA1c self-awareness among Saudi patients with type 2 DM; the accuracy of reported HbA1c, their association with glycemic control, and the factors that might be related to glycemic control. The study was carried out in the outpatient’s diabetes clinics at tertiary hospitals in Riyadh, Qassim, and Jeddah, Saudi Arabia.
The inclusion criteria consisted of either male or female patients between the ages of 18-75 years who had been diagnosed with type 2 DM at least one year ago and who underwent regular follow-up visits for diabetes care. We excluded patients with a past history of bariatric surgery and renal insufficiency (creatinine level >1.5 mg/dl), known underlying illnesses (such as malignancy or hemoglobinopathies), received a blood transfusion within the past 30 days, or were pregnant. Also, the participants were excluded if for any reason they could not communicate verbally.
Patients were approached using a simple time random interval technique.17 A total of 3 different days every week were chosen. During the early morning of each of these days, we visited the outpatient diabetes clinics and obtained the sample frame of all patients who met our inclusion criteria. A random sample was then selected from the sample frame. The informed consent forms were obtained from the patients before the administration of the questionnaire, and all patients’ information were handled with strict confidentiality. Trained data collectors were assigned to collect the data at each center, and all were following the same process. The data was collected through face-to-face interviews from March until April 2018.
The Institutional Review Board approval No.: E-18-3084 was obtained before the beginning of this study. Participants were informed on the study objectives, and their permission to enroll in the study was requested. Written consents were obtained from the participants. The confidentiality of their information was assured.
The data was collected with an interview based on a questionnaire. The interview questionnaire was developed based on an extensive literature review and experts’ opinions.18-21 The questionnaire was composed of 2 main sections: the first section assessed the patient’s background information (age, gender, nationality, highest educational level, location, monthly income, current occupation, marital and smoking statuses, duration of DM, and type of DM treatment) and the second part addressed HbA1c (medication compliance, frequency of hospital visits, patient awareness of HbA1c, and education on the test and A1c target by a healthcare provider). The most recent HbA1c, weight, and height were gathered by the data collector from the patient’s file. Patients’ self-awareness of HbA1c was assessed based on a score of 4 questions. Patients were asked if they had heard or were aware of the term HbA1c. Those who answered yes proceeded to answer 3 other questions on HbA1c, including: what HbA1c means, their target HbA1c goal, and whether they could correctly identify their current HbA1c value. Participants were categorized as having good HbA1c self-awareness if they could answer 3 out of 4 questions on HbA1c correctly while those who did not hear of the test before or scored less than 3 out of 4 were categorized as not having a good awareness of the test.19 The reported HbA1c was considered accurate if the value was within ±0.5% of the recorded HbA1c. Good glycemic control was defined as having an HbA1c of <7%. The questionnaire was initially developed in English. A total of 2 accredited translators were assigned to translate the questionnaire into Arabic and then translate it back into English. Both the original and final English versions were reviewed, and any disagreements between them were solved by the principal author and the translators.21 To perform the above process of face and content validity and reliability (using test and re-test method) of the final Arabic version, a pilot study was carried out and it included 60 patients with type 2 DM. For most of the variables, good correlation was observed which indicated that the Arabic version instrument was reliable in obtaining the responses. The pilot study’s participants were not included in the main study. Using the following single proportion formula, assuming that alpha is equal to 1.96 for a 95% confidence interval (CI) level, a precision is equal to 4%, and a HbA1c self-awareness prevalence of 50%, the calculated sample size was 600 subjects.
Where Z = Z value, p = the prevalence, and d = precision.
Statistical analysis
Data was analyzed using Statistical Package for the Social Sciences, version 26.0 (IBM Corp., Armonk, NY, USA) and MedCalc® Statistical Software, version 20.015 (MedCalc Software Ltd, Ostend, Belgium). Descriptive statistics (mean, standard deviation [SD]), frequencies, and percentages) were used to describe the quantitative and categorical variables. Karl Pearson and Spearman’s correlation coefficients were used to assess the reliability of an instrument using test and retest method of observations from a pilot study. Bland and Altman plot analysis was used to quantify the bias between the patient reported and actual HbA1c values. Student’s paired t-test and independent samples t-test were used to compare the mean values of quantitative variable (HbA1c). Pearson’s Chi-square test and unadjusted odds ratio (OR) were used to observe and measure an association between the categorical study variables and binary outcome variables (awareness of HbA1c and glycemic control). Multivariate analysis (step wise binary logistic regression) was carried out to obtain adjusted ORs and to obtain the independently associated variables of HbA1c awareness and glycemic control. A p-value of ≤0.05 and 95% CIs were used to report the statistical significance and precision of results.
Results
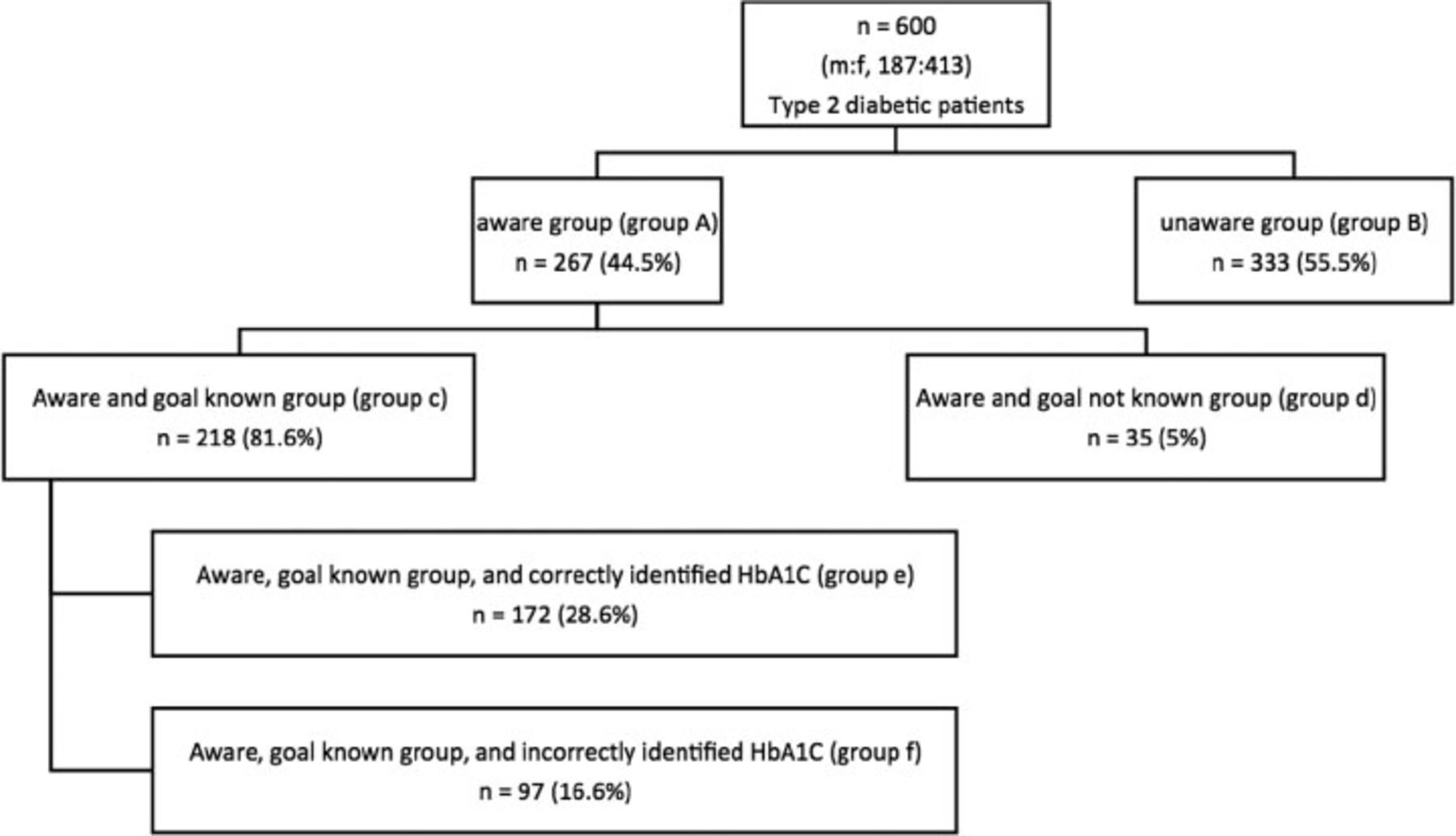
Out of 600 participants enrolled, 68.8% were females. The mean age of the respondents was 54.7 years, where 39% were in the age group of 51-60 years. Approximately 70% were from outside Riyadh. In 54.5% of the participants, the duration of DM was ≤10 years. Approximately 45% were on tablets alone as a treatment for their DM and more than 90% were adhered to their anti-diabetic medications (Table1). Among all participants, the mean HbA1c level was 8.6±1.19 while among those who reported knowing their HbA1c, the mean HbA1c level was 7.6±1.3, which was very close to the self-reported HbA1c levels among this population. With respect to knowledge on HbA1c and control, most participants (55.5%) did not have good HbA1c self-awareness. Only 126 (21.0%) of the participants had HbA1c levels indicative of good glycemic control.
- The frequency distribution of the causes of burns in patients
Figure 1 shows the details of HbA1c self-awareness among the participants. The majority (47.8%) of the participants had heard of the HbA1c test before. Among those respondents who had heard of the test before, 49.2% were not aware of the HbA1c test meaning, 55.9% knew their HbA1c goal target, and 59.9% were aware of their last HbA1c result. Also, the majority of the participants were not educated by their health care providers on the meaning of the HbA1c test and their HbA1c’s target goal.
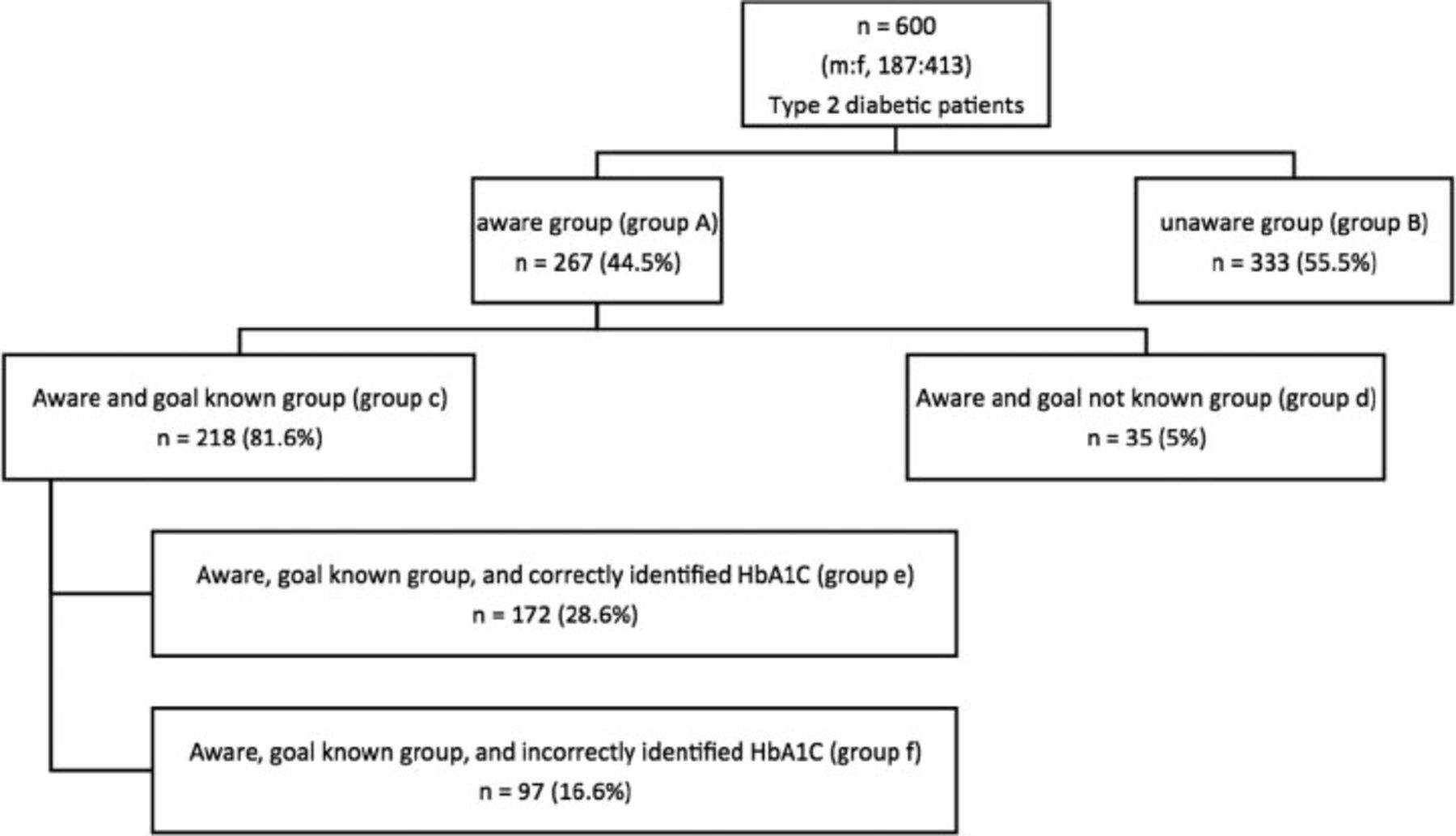
- The details of hemoglobin A1c (HbA1C) self-awareness among study subjects. m: male, f: female
The mean self-reported HbA1c was similar to the actual HbA1c among patients who reported knowing their HbA1c levels (p>0.05). Whereas actual HbA1c levels were significantly lower among those who reported their HbA1c levels compared to those who had not. The mean difference between these 2 groups was 1.8% (p<0.0001, 95% CI: [1.5-2.0]).
The bias between actual and patient reported HbA1c values was assessed using Bland and Altman plot. The mean difference between 2 ways of obtaining HbA1c values was 0.2796% which was statistically significantly different from the ‘0’ of no difference (p<0.0001, 95% CI: [0.203-0.356]).
Table 2 shows that among patients who accurately reported their HbA1c, a small and non-significant difference between their actual and reported HbA1c levels was found. A much larger and significant difference between reported and actual HbA1c values among patients who inaccurately reported their HbA1c levels (p=0.0008).
- A comparison of mean self-knowledge and recorded hemoglobin A1c values between participants who accurately and inaccurately reported.
Out of all the study variables, gender, education level, monthly income, occupation, duration of DM, number of follow-up visits, and glycemic control were statistically significantly associated with participant’s HbA1c awareness (p<0.001). The OR of having good awareness of HbA1c was significantly higher in male participants when compared females. The OR of good HbA1c awareness among educated participants were significantly higher when compared with those who did not attended school and the OR increased as the educational level of participants was higher. Also, the higher monthly income participants were having higher OR of good HbA1c awareness when compared with lower monthly income participants. Higher OR of good HbA1c awareness was observed among the participants who work in government when compared with unemployed. The OR of having good HbA1c awareness were significantly higher in participants who had ≤10 years duration of DM, ≤3 number of follow-up visits, and those who had glycemic control when compared with the participants with >10 years duration of DM, >3 follow-up visits, and who did not have glycemic control (Table 3).
- Association between study variables and study participant’s HbA1c awareness.
Table 4 shows the association between glycemic control and participant’s socio-demographic and clinical characteristics. Glycemic control was significantly associated with gender, educational level, location, monthly income, duration of DM, type of treatment, awareness of HbA1c, and binary responses of educated on meaning of HbA1c, educated on the target of HbA1c, and heard of HbA1c. The OR of having glycemic control was significantly higher in females when compared with males participants. The participants who had Master/PhD of educational level were having glycemic control of significantly higher OR when compared with those who did not attend school. The OR having glycemic control among the participants of outside Riyadh, higher monthly incomes, ≤10 years of duration of DM, taking no treatment, only diet, only tablets, having good HbA1c awareness, those got educated on meaning of HbA1c, educated on the target of HbA1c, and those heard of HbA1c were significantly higher when compared with those who reside in Riyadh, having lower monthly income, >10 years of DM duration, taking tablets and insulin, not good HbA1c awareness, not educated on meaning of HbA1c, not educated on the target of HbA1c, and not heard of HbA1c.
- Association between study variables and study participant’s HbA1c awareness.
There was no significant association between glycemic control and age groups, number of follow-up visits, occupation, and medication compliance. Multivariable stepwise binary logistic regression analysis was used to identity the independently associated factors of HbA1c awareness and glycemic control.
After adjusting the age groups, gender, occupation, location, type of treatment, adherence to treatment, and duration of DM, 4 participants’ characteristics were independently statistically significantly associated with HbA1c awareness. These characteristics were glycemic control, education level, monthly income, and number of follow-up visits. The adjusted OR and its 95% CIs were shown in Table 5. This model with all the above variables against a model with only constant was statistically significant indicating that the above variables as a set distinguishing between the participants with good HbA1c awareness and not good HbA1c awareness (χ2=131.50; df=10; p<0.0001). Hosmer and Lemeshow test which tests for the goodness of fit for logistic regression models (an alternative to model Chi-square test) had a value of 5.557 (df=10; p=0.592). This non-significance indicated that the model prediction did not significantly differ from the observed. Nagelkerke’s R2 of 0.263 indicated a moderate relationship between prediction and grouping. The Wald criterion demonstrated that the variables in the model at the step 4 made a significant contribution to the prediction of good HbA1c awareness. The final model validation was carried out using classification table which summarizes the observed group and predicted group classification. The overall prediction success was 69.8% (Table5).
- Independent factors of awareness of HbA1c and glycemic control (by multivariate analysis).
In this multivariate model it was found that 3 characteristics (type of treatment; diet only, tablets only; duration of diabetes; and awareness of HbA1c) were found as independent factors associated with the glycemic control, after adjusting for age groups, gender, educational level, location, income level, number of follow up visits, educated on the meaning of HbA1c, educated on target of HbA1c, and Heard of HbA1c before. The adjusted OR and its 95% CIs were shown in Table 5. This model with all the above variables against a model with only constant was statistically significant indicating that the above variables as a set distinguishing between the participants with glycemic control and those with no glycemic control (χ2=171.84; df=9; p<0.0001). Hosmer and Lemeshow test which tests for the goodness of fit for logistic regression models (an alternative to model chi-square test) had a value of 7.244 (df=10; p=0.511). This non-significance indicated that the model prediction did not significantly differ from the observed. Nagelkerke’s R2 of 0.388 indicated a moderate relationship between prediction and grouping. The Wald criterion demonstrated that the variables in the model at the step 4 made a significant contribution to the prediction of glycemic control. The overall prediction success was 82.5% (Table5).
Discussion
The key findings of this multicenter study showed that the prevalence of HbA1c self-awareness was approximately 44.5%. Overall, 28.6% of those with the self-knowledge of their own HbA1c levels accurately reported their HbA1c self-knowledge (when compared to their own laboratory value). Furthermore, participants who reported an accurate value for HbA1c self-knowledge had a statistically significant lower mean HbA1c value compared to those participants who report an inaccurate value for their own HbA1c (7.4%; p<0.0008). The prevalence of good glycemic control (defined as HbA1c <7.0%) was 21.0%. Among those who had good HbA1c self-awareness, 77% were found to have good glycemic control (p<0.000). In a multivariate model by controlling several factors, this study has observed 4 variables which were independently associated with self-awareness of HbA1c and 3 variables were independently associated with glycemic control.
In a European study in 2017, over 8 European countries evaluated the prevalence of accurate self-knowledge of a patient’s own HbA1c level and its association with glycemic control. Almost half (49.4%) of the patients reported their HbA1c, and among those patients, 78.3% reported it accurately, while in our study, among the 269 patients who reported knowing their HbA1c level, 28.6% reported it accurately (reported HbA1c within 0.5% of actual measured HbA1c).18 This percentage was substantially lower than that estimated in another study. However, in a study carried out in the United States, only 25% of patients accurately reported their HbA1c, a percentage lower than that reported in this study.22 Both studies indicated that poor HbA1c recall was significantly associated with having a higher recorded HbA1c level, implying that poor self-knowledge of one’s own HbA1c was associated with worse glycemic control. These 2 studies dealt with substantially different sample sizes and populations from each other and from those described in this study.
In our study, the group who had good HbA1c self-awareness was found to have a statistically significantly lower recorded HbA1c Lab (7.5%) compared to the unaware group (9.3%). This finding was consistent with findings in the literature. In studies carried out in India and England, patients with good HbA1c self-awareness were found to have substantially lower HbA1c levels than other patients.18,23 Additionally, there was a statistically significant association of good glycemic control and being educated by health care providers regarding the meaning of current and target HbA1c goals. Also, good control was associated with younger age, less duration of DM, high education level, high monthly income, and location.
The main strength of this study was the assessment of unusual factors that may affect glycemic control within the Saudi Arabian population. It was a multicenter study with a large sample size, randomly chosen participants, and data for a wide variety of different covariates. The availability of this data allowed us to assess whether our findings were confounded. Even when controlling these potential confounders, HbA1c self-awareness remained a significant and substantial predictor of glycemic control.
Study limitations
All data were collected cross-sectionally. Therefore, the causal relationship between the dependent and independent variables cannot necessarily be known for certain. For example, this study’s primary finding was a strong association between HbA1c self-awareness and glycemic control. Therefore, based on these data, we cannot say with certainty that HbA1c self-awareness causes patients to have better glycemic control. A longitudinal study in which data on HbA1c self-awareness was collected first and then the changes were traced in HbA1c among those with and without good self-awareness to finally compare data between both groups, that would be a better way of addressing causality.
These findings have important public health implications and clinical significance. Type 2 DM remains a growing problem around the world and also in Saudi Arabia. Several studies have shown a high prevalence of poor glycemic control worldwide.12,15 Therefore, unless the unusual factors that we described promote glycemic control among those with type 2 DM, the burden of this problem on the health care system will increase.
This study provides valuable prevalence data and can give rise to future prospective randomized controlled studies to examine the effect of HbA1c self-awareness as part of a structured educational program on HbA1c outcomes and suggest that the effort to educate health care providers and patients may have had a beneficial effect.
In conclusion, our study showed a positive association between HbA1c self-awareness and glycemic control. Glycemic control was good among those who were educated on the meaning of the test, their HbA1c level, and their target HbA1c. Awareness among health care providers regarding the role of patient education on their conditions might help provide a patient with optimal care. Further studies with different experimental designs are needed to study this association as a part of a structured educational program.
Acknowledgment
The authors gratefully acknowledge American Manuscript Editors for English language editing.
Footnotes
Disclosure.This study was supported by Deanship of Scientific Research, College of Medicine Research Centre, King Saud University, Riyadh, Saudi Arabia.
- Received November 1, 2021.
- Accepted January 18, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.