


Abstract
Objectives: To assess the frequency of olfactory dysfunction (OD) among individuals afflicted with coronavirus disease of 2019 (COVID-19).
Methods: A comprehensive literature search was carried out across several bibliographical databases (PubMed, Scopus, Google Scholar, and Web of Science) to extract publications in the English language between January 2020 and December 2021 to report the incidence of OD alone or together with gustatory dysfunction (GD) among COVID-19 patients.
Results: Based on eligibility criteria, 84 articles were included from 27 countries, comprising 36,903 patients, of whom 58.1% were females. The generality rates of olfactory impairment alone was 34.60% and in conjunction with GD was 11.36%. Patients with OD were subclassified into various categories, and the prevalence of anosmia was 20.85%, 5.04% for hyposmia, 8.88% for anosmia or hyposmia, 1.84% for parosmia, 0.78% for phantosmia, and 0.02% for hyperosmia, among COVID-19 patients.
Conclusion: Clinical features associated with OD, either isolated or in combination with GD, are common in patients with COVID-19 and consider important signs of COVID-19 that may guide clinicians in the early phase of the disease.
PROSPERO Reg. No.: 417296
The coronavirus of 2019 (COVID-19) pandemic has evolved into a worldwide emergency, posing a substantial public health challenge, with rapid dissemination and increased mortality. The global health crisis continues to affect the world today and is expected to do so in the future. Although, first observed in December 2019 in Hubei Province, China, it has spread rapidly worldwide. On 11 March 2020, COVID-19 was declared a ‘pandemic emergency’ by the World Health Organization (WHO). Currently, 274,628,461 confirmed cases and 5,358,978 deaths have been reported worldwide.1
The COVID-19 is the result of an emerging beta-coronavirus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). These are single-stranded RNA viruses that cause respiratory, hepatic, enteric, and neurological illnesses. The incubation period spans from 1-14 days, during which the most frequently encountered symptoms include fever, cough, shortness of breath, breathing difficulties, and fatigue. Furthermore, some individuals with COVID-19 have reported experiencing olfactory disorder and anosmia.2,3 The intensity of these symptoms varies among individuals and is influenced by factors such as the duration of virus exposure, the patient’s age and gender, and the presence of underlying health conditions.4
Healthcare professionals and researchers around the globe are endeavoring to gather a multitude of evidence aimed at comprehending the epidemiology, clinical characteristics, and predictive elements of COVID-19. The sinonasal tract plays a significant role in the pathogenesis of viral infections.5 The relationship between loss of smell and COVID-19 was first proposed by Mao et al.6 Since then, the number of studies explaining the relationship between olfactory dysfunction (OD) and other symptoms of COVID-19 has increased.7,8 A recent systematic review carried out by Aziz et al2 concluded that OD is a prevalent symptom in patients with COVID-19. On 26 March 2020 the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) reported that the COVID-19 anosmia reporting tool for clinicians which showed that anosmia was present in 73% of cases before the laboratory diagnosis of COVID-19 and was the main presenting symptom in 26.6% of the cases.9,10 Due to the rising occurrence of olfactory symptoms in individuals with COVID-19, the Centers for Disease Control and Prevention have recently included ‘new loss of taste or smell’ in the roster of symptoms that can manifest 2-14 days following exposure to the virus.11
Although OD is one of the most underreported symptoms of COVID-19, it is sometimes the only presenting symptom in these patients.2 Therefore, a comprehensive comprehension of COVID-19 symptoms holds significant importance in early disease detection and transmission prevention. In light of this, this systematic review seeks to consolidate existing literature on OD in COVID-19, emphasizing the role of ear, nose, and throat (ENT) specialists in efforts to mitigate the impact of this severe pandemic.
Methods
The main objective of this study was to carry out a systematic assessment and description of documented instances of anosmia linked to infections caused by SARS-CoV-2. This structured review adhered to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines.12
Eligibility criteria
We systematically combed through clinical evidence, specifically seeking original peer-reviewed journal articles. These articles encompassed observational studies that explored the occurrence of OD in individuals afflicted with COVID-19. The range of publications published between January 2020 and December 2021 was limited. Case reports, case series, letters to the editor and replies, conference papers, book reviews, book chapters, newspaper and newsletter articles, expert opinions, theses and dissertations, and studies written in languages other than English were ruled out.
Data sources and search strategy
We carried out a thorough search of the scientific literature across various electronic bibliographic databases, including PubMed, Scopus, Google Scholar, and Web of Science. We collected all articles published between January 2020 and December 2021. The Scopus database was explored by S. S. S., Google Scholar database by H. S. S., and the Web of Science by N. M. M. Two investigators (A. F. T. and Z. A. Q.) independently examined all articles in a standardised manner to determine their eligibility and subsequently compared the eligible articles. A final review of the selected articles was carried out by all investigators (F. M. K., F. A. M., Amit F. W. H., and R.S.O.). The following search terms were used to screen the different databases: PUBMED (search until 29.12.2021): (anosmia) OR (loss of smell) OR (hyposmia) OR (olfactory dysfunction) AND (COVID 19) OR (coronavirus pandemic) OR (SARS-CoV-2); SCOPUS (search until 27.12.2021): (Anosmia OR hyposmia OR loss of smell OR olfactory dysfunction AND COVID-19 OR coronavirus); Google Scholar (search until 28.12.2021): Olfactory dysfunction or anosmia in COVID-19; Web of Science (search until 25.12.2021): ‘Olfactory dysfunction in COVID-19’ OR ‘Loss of smell in coronavirus pandemic’ OR ‘Anosmia/hyposmia in coronavirus pandemic’.
Data collection
The study followed a 2-phase approach. In Phase I, we commenced with an initial review of the study titles, followed by a subsequent assessment of their abstracts. This screening process adhered to predefined inclusion and exclusion criteria. Articles that met the eligibility criteria based on their titles and abstracts were then subject to a comprehensive evaluation for final eligibility. Any duplicate or irrelevant articles were systematically excluded from the review, and we procured the full texts of all studies with potential relevance.
Following the initial filtering phase, the chosen articles underwent a reference screening in Phase II to identify any new studies that might meet the eligibility criteria. Two independent reviewers carried out a thorough examination of the full-text articles and extracted pertinent data. Furthermore, the references cited in the selected articles were scrutinized for any relevant studies, and the Zotero software was employed to extract additional references. Additionally, we carried out a literature search by examining the reference lists of prior systematic reviews and meta-analyses.2,13-19
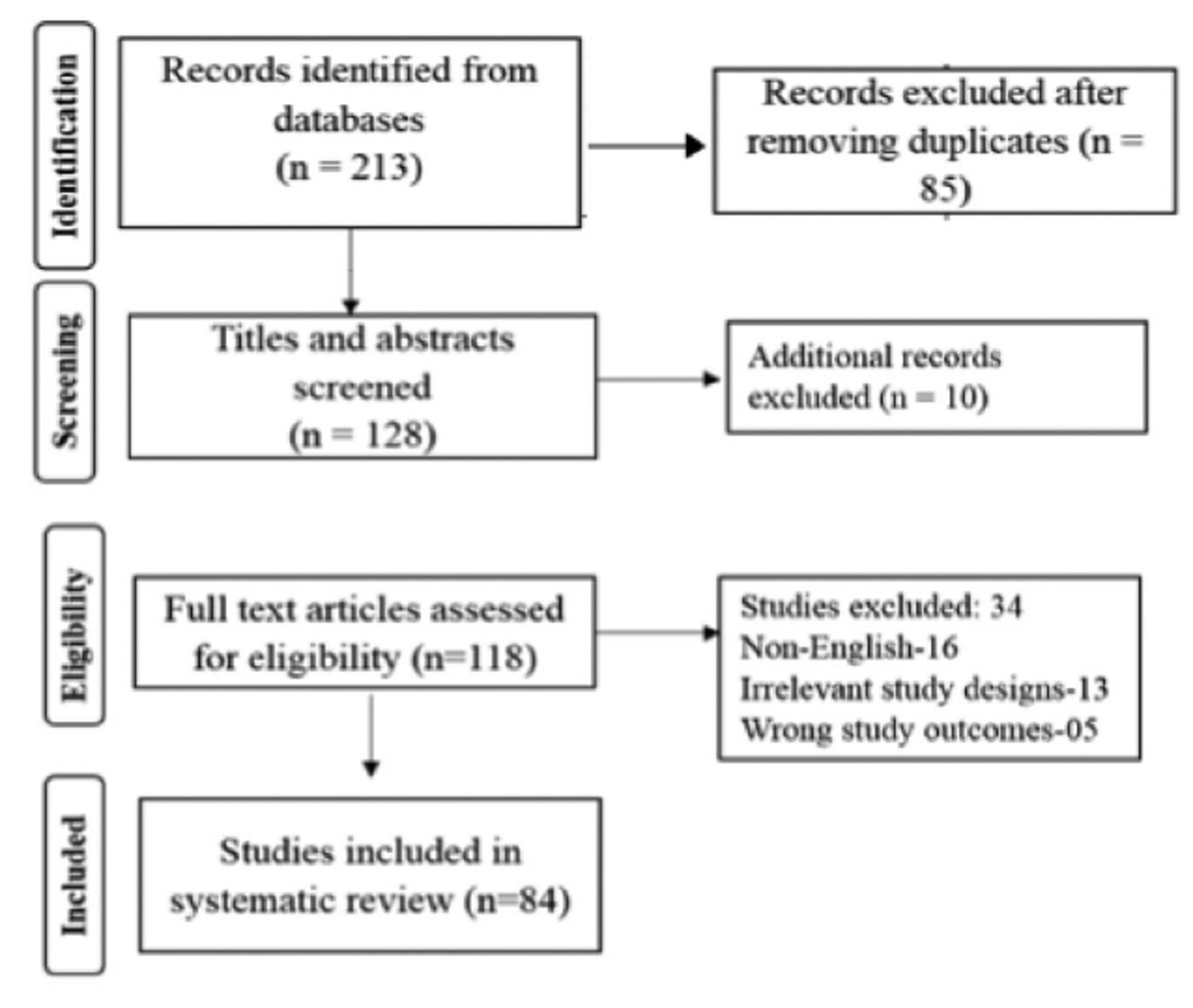
All studies reporting anosmia (alone or in combination with gustatory dysfunction [GD]) in individuals with confirmed laboratory diagnoses of COVID-19 were incorporated. Studies involving patients with suspected, but unconfirmed, COVID-19 were not considered. To create a comprehensive overview, we assessed the included studies based on the following criteria: author, year of publication, country of study, the kind of study, patient information (age and gender), COVID-19 status, number of patients with olfactory impairment alone, number of patients with OD and GD, and data collection method (telephone survey, in-person interview, and elaborate questionnaire focused on olfactory ability), method of olfactory assessment, time of disease onset, duration of olfactory symptoms, time of recovery from olfactory symptoms, and treatment used for OD. In the end, a total of 84 articles met the criteria for inclusion in the systematic review. Figure 1 depicts a flowchart illustrating the article selection process.
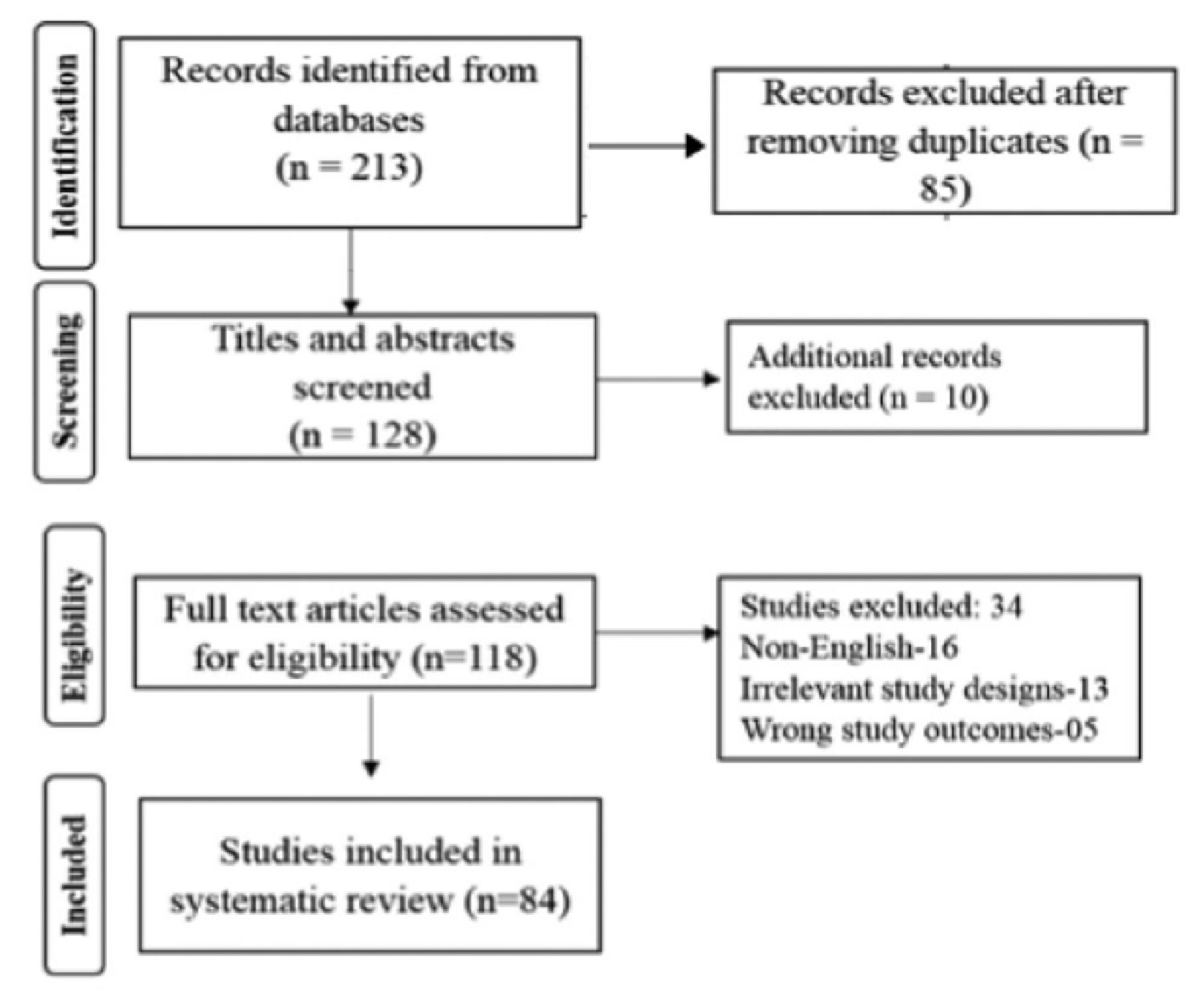
- Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart.
Outcome measures
The primary outcome was to estimate the prevalence of anosmia/hyposmia among patients with COVID-19. The secondary outcome was aimed to estimate the association between hypogeusia or ageusia and anosmia/hyposmia among patients with COVID-19.
Statistical analysis
All data obtained from the included studies were entered into a Microsoft Excel spreadsheet and analysed.
Results
Many studies and literature reviews have evaluated OD in COVID-19 positive individuals. We obtained 213 articles from the preliminary search, of which 84 were included in the final analysis, as shown in Figure 1.
A total of 36,903 patients were included in the 84 studies whose data we obtained.9,20-102 The sample sizes for the different studies ranged from 8-8238.22-79 In 2020, all articles (n=84) were published.9,20-65 However, the majority of the publications (n=47) were published in 2020, 2021, and 2022.66-102 Data from 25 different nations were included in the 84 papers (Table 1), whereas the majority of the 84 research (n=34) were cross-sectional (Figure 2). The age group most commonly represented in the studies (n=41) was 41-49 years. Among the 36,903 participants, 21,474 (58.1%) were women. The descriptive characteristics of the included studies (n=84) are presented in Table 1.
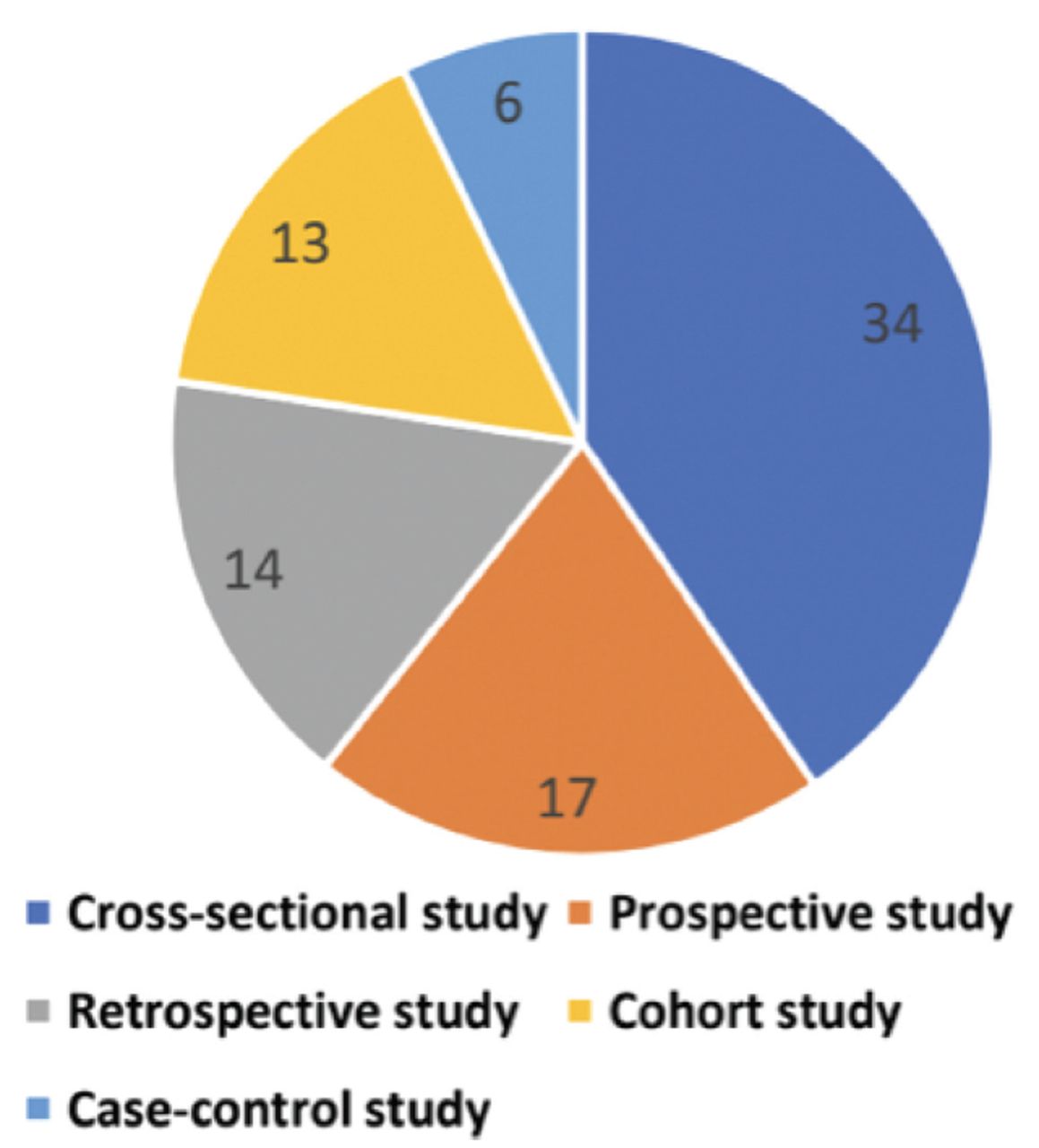
- Classification of the type of studies included in the systematic review (n=84).
- Demographic characteristics of the included studies (n=84).
The prevalence of OD is presented in Table 2. Among the 84 studies, 81 reported only OD, 40 reported the combination of OD and GD as a single entity, and 37 reported both the prevalence of OD alone and the combination of both.9-102 A total of 33,231 patients were identified for the evaluation of OD, among them, 11,499 (34.60%) reported experiencing OD alone, whereas 3777 (11.36%) patients reported a combination of OD and GD. The number of patients with OD in the included studies ranged from 3-179635-60 with the estimated prevalence of OD ranging from 3.9-100%.22,38,42,53,92 Similarly, the patients reporting both OD and GD ranged from 122-517102 with an estimated prevalence ranging from 3.9-90.9%.41,43 The patients with OD were sub-classified into various categories. In our systematic review, among COVID-19 positive individuals, the prevalence rates of anosmia was 20.85%, 5.04% for hyposmia, 8.88% for anosmia or hyposmia, 1.84% for parosmia, 0.78% for phantosmia, and 0.02% for hyperosmia. A detailed description of this process is provided in Table 3.
- Details of olfactory dysfunction experienced by the coronavirus disease-19 positive individuals (n=84).
- Classification of the olfactory dysfunction (n=84).
The most common method used to evaluate OD was the questionnaire (n=43) followed by telephonic conversation (n=15), medical records (n=11), personal face-to-face interview of the patient (n=7), online questionnaire (n=5), and email (n=2), COVID RADAR symptom tracker app (n=1), and COVID-19 anosmia reporting tool (n=1).
In our systematic review, the loss of smell as the first and only symptom was described in 8 studies.36,38,72,77,78,89,90,96 The occurrence of olfactory symptoms before the generalised symptoms of COVID-19 was reported by 14 studies.9,34,35,46,49,52,53,59,60,64,69,74,76,101 The sudden onset of olfactory symptoms was reported by 7 studies.22,42,49,75,89,92,102 Only 4 studies included patients who received treatment for OD.34,35,48,71 Details of the onset time, duration, recovery time, and treatment of OD are shown in Table 2.
Discussion
Coronavirus (SARS-CoV-2) is a global threat, resulting in widespread infections and fatalities across the world. The disease remains an active pandemic and a serious threat to healthcare systems worldwide. At first, the primary classical symptoms of COVID-19 were believed to be fever, cough, fatigue, and shortness of breath. However, more recently, OD has emerged as a prominent symptom that can aid in the detection of asymptomatic carriers of COVID-19.27
This systematic review uncovered a significant body of research documenting the loss of the sense of smell among COVID-19 patients across multiple continents. We included data from 27 countries, of which the studies published in India contributed to 11 (13.09%), 9 (10.71%) in France, 8 (9.52%) in Italy, 8 (9.52%) in Iran, and 7 (8.33%) in the United States of America (US), of the total studies included in this review.9-101 In terms of the study population, India, France, Italy, Iran, and the US carried out substantial contribution to the sample size, accounting for 3388 (9.1%) in India, 2042 (5.53%) in France, 1585 (4.29%) in Italy, 1190 (3.22%) in Iran, and 132 (3.57%) in the US of the participants. A female predominance was observed in our systematic review (58.1%), similar to the results of a meta-analysis carried out by Saniasiaya et al14 (61.4%) and a systematic review carried out by Aziz et al2 (53.1%).
The sense of smell is one of the various special sensations. Olfactory dysfunction is subclassified into complete loss of smell (anosmia), partial loss of smell (hyposmia), distorted sense of smell (parosmia), olfactory hallucinations (phantosmia), and a heightened sense of smell (hyperosmia). Regarding the aetiology of OD in general, nearly 200 causes exist, but the most commonly observed eare related to age, congenital, head trauma, post-viral, toxins (smoking or work-related), drugs (local anaesthesia, nifedipine, antimicrobials, antidepressants, and immunosuppressants), and diseases related to the sinonasal tract (allergic and non-allergic rhinitis, septal deviation, and chronic rhinosinusitis with nasal polyposis).103
In our comprehensive review, all 84 studies consistently demonstrated a robust link between the loss of smell and SARS-CoV-2 infection. Within this set, 81 studies specifically highlighted the occurrence of isolated OD, 40 studies reported a concurrent presentation of OD and GD as a unified symptom, and 37 studies reported the prevalence of both isolated OD and the combined presence of both dysfunctions. The estimated prevalence of loss of smell among 33,231 individuals with COVID-19 included in this review was 34.60% (range of prevalence from 3.9-100%).22,38,42,53,92 Our estimated prevalence was slightly lower than the global pooled prevalence found in systematic reviews carried out by Aziz et al2 (52.0%) with 51 included articles, da Costa et al15 (60.7%) with 6 included articles, Hannum et al17 (50.2%) with 34 included articles, and Agyeman et al18 (41%) with 24 included articles, where the sample size was small, whereas, our systematic review included 84 studies. In a meta-analysis carried out by Saniasiaya et al,14 it was determined that the prevalence of OD among COVID-19 patients stood at 47.85% (95% confidence interval [CI]: [41.20-54.50]).14 Tong et al13 found an overall prevalence of 52.73% (range of prevalence 5.14-98.33%) among 1,627 patients in 10 studies. Ibekwe et al16 reported a global pooled prevalence of 48.47% (ranging from 4.23-98.33%) among 19,424 patients with COVID-19 included in 27 studies. Owing to the increased prevalence of loss of smell among patients with COVID-19, the ENT Society of the United Kingdom stated that individuals complaining of anosmia while not exhibiting other clinical features might be hidden carriers of COVID-19 and are responsible for the rapid spread of COVID-19. Such individuals should self-isolate for 14 days to stop the chain of infection.104
The combined loss of smell and taste was less frequently reported in our systematic review, with only 40 studies including data from 3,777 individuals with COVID-19, resulting in a prevalence of 11.36% (generality ranging from 3.9-90.9%.41,43 A meta-analysis carried out by Tong et al13 revealed that the generality of both dysfunctions ranged from 5.61-92.65% among 626 patients in 9 studies. Ibekwe et al16 demonstrated an estimated pooled generality of 35.04% (range of prevalence from 7.96-75.74%) in 13 studies involving 5,977 patients with COVID-19. A multicentric European study included in the review reported the commonness of OD to be 85.6% and GD to be 88.8%.34 The data regarding the combined prevalence of OD and GD are limited as most systematic reviews have only reported the commonness of either OD or GD.
Pathophysiology
The precise pathophysiological mechanisms underlying the loss of smell in individuals with COVID-19 remain incompletely comprehended, but there are a few hypotheses that have already been presented in the literature. Zhou et al105 unveiled a new SARS-CoV-2 infection on February 3, 2020. Their study elucidated the invasion of human lower respiratory system cells by SARS-CoV-2 through the utilization of ACE2 and transmembrane protease serine 2 receptors. Among these receptors, ACE2 is predominantly located on cells in various tissues, including the lungs, liver, kidneys, gastrointestinal (GI) tract, and even the nasal epithelium.106 Respiratory epithelial cells and supporting olfactory cells act as the chief reservoir site and the second most susceptible site for the replication of this deadly virus, as they harbour the highest concentration of the 2 above-mentioned genes (abACE2 and TMPRSS2) responsible for smell loss.107,108 Based on this hypothesis, 3 mechanisms have been postulated for the loss of smell. First, infection of the nasal mucosa by SARS-CoV-2 triggers the inflammatory process of the respiratory and olfactory mucosa, creating a barrier to the odour of the aromatic particles present in the air between the olfactory neurones and mucosa, leading to disruption of the process of odour detection.109 The second mechanism is the direct attack of the virus to the olfactory mucosa causing inhibition of the transmission of olfactory signals, leading to temporary or permanent dysfunction of the olfactory mucosa.110,111 The final mechanism involves the virus infiltrating the cribriform plate, thereby infecting the olfactory bulb. This allows the virus to follow the olfactory pathway, ultimately reaching the brain and impacting the olfactory cortex in the temporal lobe, leading to a loss of the sense of smell.112 Hence, the involvement of any one or all of these mechanisms is responsible for the temporary or permanent loss of smell caused in COVID-19 positive individuals.
Symptoms
To better understand the prevalence of OD, clinical symptoms, and the correlation between these symptoms and disease progression in individuals with COVID-19, the AAO-HNS has provided a COVID-19 anosmia reporting tool.10 Similarly, in our review, the objective assessment of olfactory symptoms was carried out in 14 studies using the University of Pennsylvania smell identification (UPSIT, n=6), odour threshold Sniffin’ Sticks (n=5), sinonasal outcome (SNOT, n=2), and connecticut chemosensory clinical research center (CCCRC, n=2) tests were used.23,26,33,37,43,53,58,64,66,89,92,99,100 In the meta-analyses carried out by Saniasiaya et al14 of 4 studies and Aziz et al2 of 8 studies (out of 51), utilised objective assessments. Saniasiaya et al14 found a higher prevalence of OD using an objective evaluation (72.10%) rather than a subjective one (44.53%). In another systematic review carried out by Hannum et al,17 6 studies (out of 34) used the objective assessment method, and the prevalence of OD was found to be high using objective methods (77% vs. 44%). A meta-analysis carried out by Tong et al13 reported a higher prevalence of OD using the UPSIT compared to other instruments. Each method has advantages and disadvantages. Objective methods quantify smell loss better because they are standardised, whereas subjective methods, such as questionnaires and interviews, have more flexibility and variability, are easy to use, and are cost-efficient. However, they lack standardisation and are subject to recall bias.
Smell loss is one of the most underreported symptoms in patients with COVID-19, and sometimes it can be the only complaint of the patient. In our systematic review, the occurrence of loss of smell as the first and only symptom was described in 8 studies36,38,72,77,78,89,90,96 and the sudden onset of olfactory symptoms was reported in 7 studies.22,42,49,75,89,92,102 The AAO-HNS found that anosmia was the first symptom in 26.6% of patients.10 The occurrence of olfactory symptoms before the generalised symptoms of COVID-19 was reported in 14 studies.9-101 Giorli et al19 in their meta-analysis reported the early appearance of olfactory symptoms as compared to other ones in 11.8% of patients. While developing the COVID-19 anosmia reporting tool for clinicians, the AAO-HNS reported in their study that the occurrence of anosmia before the diagnosis of SARS-CoV-2 was found in 73% of patients.10 The AAO-HNS also suggested that the possibility of COVID-19 should be considered among individuals with a sudden loss of anosmia or ageusia in the absence of other respiratory symptoms.113
Imaging
Imaging modalities are not routinely required in patients with OD because in most cases, they are negative and of no use. As per the consensus guidelines by the British Rhinological Society (BRS), when a patient exhibits a loss of smell alongside other nasal symptoms persisting for 4-6 weeks (irrespective of COVID-19 status), it is recommended to carry out nasal endoscopy prior to resorting to imaging procedures.114 The BRS states that if patients present with a loss of smell for more than 4-6 weeks along with the presence of neurological manifestations, brain MRI should be carried out regardless of COVID-19 status.114 In the present review, imaging modalities were used in only 3 studies.37,42,92 The utility of these modalities has not yet been proven and they are only reserved for patients with persistent OD.
Prognosis
The treatment of OD depends on the aetiology of smell loss; however, it is required only in cases where OD does not improve spontaneously or persists even after 2 weeks. Generally, the management of OD involves addressing its root cause, employing medical interventions such as oral and topical steroids, and considering surgical options like septoplasty, turbinoplasty, and endoscopic sinus surgery.103 As for the treatment of OD in COVID-19 patients, the BRS has established a set of consensus guidelines. These guidelines encompass various approaches, including olfactory training and support (for patients experiencing a loss of smell lasting more than 2 weeks), the use of intranasal corticosteroid sprays, intranasal corticosteroid drops (recommended for patients with both a loss of smell and nasal symptoms lasting more than 2 weeks), oral corticosteroids (suitable for patients with a loss of smell and other nasal symptoms for 2 weeks, provided they have resolved their COVID-19 symptoms), and the consideration of alpha-lipoic acid or omega-3 supplements (particularly for individuals with isolated loss of smell lasting more than 2 weeks).114 In the present review, 4 studies mentioned specific treatments for smell loss.34,35,48,71 In a systematic review carried out by Saniasiaya et al,14 there was no mention of a particular treatment protocol for addressing olfactory impairment. Similarly, most of the studies included in our review did not employ a specific treatment approach for OD. This choice is influenced by the uncertainty surrounding the effectiveness of oral steroids, as well as concerns regarding their potential to promote upper respiratory tract infections.
The prognosis of OD depends on the underlying cause; however, in most cases, patients recover within 30 days without treatment, suggesting a good prognosis. In our review, the outcome/recovery of olfactory symptoms was mentioned in 48 studies. Of these 48 studies, the persistence of olfactory symptoms after one month was observed in 13.23-102 Hopkin et al25 in their study concluded that an improvement in the loss of smell within a week of onset was observed in 80% of patients. A study carried out by Mendonca et al115 stated that the presence of OD among patients with COVID-19 can be a sign of a good prognosis.
Study strength & limitations
The strength of this systematic review lies in its sample size, as we attempted to include studies from multiple continents. In addition, we depicted the prevalence of OD alone and in combination with GD that has not been previously reported by many studies. Although we carried out an extensive literature search, our systematic review had certain limitations. Since we only included studies published in bibliographic databases and in the English language, excluding unpublished and grey literature, certain biases such as language bias and publication bias are present in the systematic review. Second, we did not consider the role of pre-existing diseases in patients with COVID-19, as they can exaggerate the COVID-19 disease and its symptoms. In addition, objective evaluations were carried out in only a small number of studies. Furthermore, owing to the controversial association between COVID-19 and OD, loss of smell has been underreported in many studies, leading to an underestimation of the overall rampancy of these symptoms. Hence, more studies and systematic reviews should be carried out to overcome these drawbacks.
In conclusion, the rampancy of OD alone was 34.60% and in combination with GD was it was 11.36%, in COVID-19 positive individuals. After classifying OD, variations were observed in the prevalence of anosmia (20.85%), hyposmia (5.04%), anosmia or hyposmia (8.88%), parosmia (1.84%), phantosmia (0.78%), and hyperosmia (0.02%) in patients with COVID-19.
The clinical characteristics linked to OD, whether in isolation or coupled with gustatory impairment, frequently manifest in COVID-19 patients. These manifestations serve as crucial indicators that can facilitate the early detection of the disease. Heightening awareness of these symptoms plays a pivotal role in ensuring the timely diagnosis and treatment of this serious COVID-19 condition.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for their English language editing.
Footnotes
Disclosure. This study was supported and funded by the Deanship of Scientific Research at Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, Saudi Arabia (grant no.: IMSIU-RG23090).
- Received June 6, 2023.
- Accepted September 20, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.
- 22.↵
- 23.↵
- 24.
- 25.↵
- 26.↵
- 27.↵
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.
- 40.
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.
- 46.↵
- 47.
- 48.↵
- 49.↵
- 50.
- 51.
- 52.↵
- 53.↵
- 54.
- 55.
- 56.
- 57.
- 58.↵
- 59.↵
- 60.↵
- 61.
- 62.
- 63.
- 64.↵
- 65.↵
- 66.↵
- 67.
- 68.
- 69.↵
- 70.
- 71.↵
- 72.↵
- 73.
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.↵
- 90.↵
- 91.
- 92.↵
- 93.
- 94.
- 95.
- 96.↵
- 97.
- 98.
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.