


Abstract
Objectives: To evaluate clinical indicators in order to examine the intensity of diabetes ketoacidosis (DKA) episodes in children and adolescents diagnosed with type 1 diabetes mellitus (T1DM).
Methods: Data from 156 T1DM patients aged 6 months to 14 years, who presented with DKA to the emergency room, were retrospectively reviewed from 2018 to 2022. Data on demographic characteristics, economic status, initial clinical presentation, glycemic control, DKA severity, and laboratory evaluations were also collected.
Results: Diabetes ketoacidosis episodes were more prevalent among male patients during the middle childhood age group. Notably, these episodes displayed seasonal patterns. The severity was found to be inversely associated with economic status and positively correlated with early adolescence. Newly diagnosed T1DM patients constituted 52.9%, with a statistically significant connection observed between severe DKA and this subgroup. Furthermore, there was a significant escalation in poor glycemic control with episode severity. Prolonged episode duration also exhibited a statistically significant association with more severity. Gastrointestinal symptoms were commonly reported during the presentation. Moreover, several clinical signs and symptoms, including decreased consciousness, reduced activity, drowsiness, Kussmaul breathing, shortness of breath, vomiting, tachycardia, and severe dehydration, were significantly correlated with the severity of DKA (p<0.05). Hypernatremia was more frequent among children with severe DKA.
Conclusion: Diabetes ketoacidosis was observed to occur more frequently among males in middle childhood with seasonal variations. Furthermore, the severity of DKA was associated with lower economic status, early adolescence, and the presence of hypernatremia.
Type 1 diabetes mellitus (T1DM) is a prevalent endocrine metabolic disorder. The incidence rate of T1DM across the globe was reported to be 15 out of every 100,000 and the prevalence of 95 out of 100,000 individuals.1 Over the past few decades, the incidence and prevalence of T1DM in the Kingdom of Saudi Arabia (KSA) have increased. According to the most recent data, the incidence rate was 29/100,000, whereas the prevalence rate of T1DM in KSA was 109.5 per 100,000.2,3 Diabetes ketoacidosis (DKA) is recognized as a life-threatening acute complication of T1DM characterized by hyperglycemia, ketonemia, ketonuria, and metabolic acidosis.
Patients usually present with nausea, vomiting, abdominal pain, decreased level of consciousness, Kussmaul breathing, and dehydration.4 Previous studies conducted in KSA have shown that the incidence of DKA at the diagnosis of T1DM has decreased from 77% to 37.7%, owing to increased levels of education and awareness among the Saudi population. Furthermore, it was observed that DKA was more prevalent in females and during the winter season.5,6 The severity of DKA is determined by the degree of acidosis, which is classified as mild, moderate, and severe.4 Moreover, there are multiple risk factors for DKA including younger age, low socioeconomic status, and poor glycemic control.7 In the present study we aim to assess clinical indicators in order to examine the severity of diabetes ketoacidosis (DKA) episodes in children and adolescents diagnosed with type 1 diabetes mellitus (T1DM).
Methods
A total of 156 patients’ medical records were retrospectively reviewed by the hospital’s electronic documentation system. Relying on data from the pediatric emergency room, the inclusion criteria included all patients with type 1 diabetes from between the ages of 6 months to 14 years who presented with DKA from January 2018 until December 2022, whether they were known or newly diagnosed with diabetes, whereas other types of diabetes and patients with lost medical records details were excluded, the study was approved by the Ethics Committee of King Abdulaziz University Hospital, Jeddah, KSA.
Data related to patients’ demographics including age were calculated based on their date of birth, categorized in this study into infants (6–12 months), toddlers (13 months–2 years), early childhood (2–5 years), middle childhood (6–11 years), and early adolescence (12¬–14 years) according to the National Institute of Child Health and Human Development.8 Gender is presented as male or female, nationality is categorized as Saudi or non-Saudi, and economic status is documented as low if monthly income is <5300 riyals or good if monthly income is >5300 riyals. This information pertains to the average income in KSA.9 Confidentiality was maintained for all participants throughout our study.
The sample population was stratified into 2 distinct groups, distinguishing between individuals with known diabetes and those who were newly diagnosed. To account for potential seasonal variations, the timing of the presenting episodes was categorized into spring (March, April, and May); summer (June, July, and August); autumn (September, October, and November); and winter (December, January, and February).10 Several additional factors were gathered for analysis, including the duration of T1DM in years, the presence of co-existing chronic conditions and their specific nature, and the duration of acute episode complaints before the patients’ presentation to the emergency department, measured in days. The duration of DKA episodes in hours was categorized as <24 hours, 24–48 hours, and >48 hours. For patients with known T1DM, glycemic control was assessed using hemoglobin A1C (HbA1C) percentages, classifying it as poor (>9%), average (7–9%), and good (<7%).
Additionally, the presentation of signs including—tachycardia, fever, blurry vision, Kussmaul breathing, polyphagia, polyuria, polydipsia, and the Glasgow Coma Scale (GCS), And Symptoms including—convulsions, reduced activity, drowsiness, headache, shortness of breath, abdominal pain, nausea, vomiting, and diarrhea, All were retrospectively documented.11
The degrees of dehydration at the time of presentation were assessed and classified as mild, moderate, and severe.12
According to the International Society of Pediatric and Adolescent Diabetes, the severity of DKA was categorized into mild, moderate, and severe based on blood pH and bicarbonate levels, with pH ranges of 7.2–7.3, 7.1–7.2, and <7.1 and bicarbonate levels of 10–18, 5–10, and <5, respectively.4 The corrected sodium (Na) equation was calculated as the measured Na value plus 1.6 times the difference between plasma glucose in mg/dL and 100, divided by 100, and expressed by mmol/L.13 We referenced normal Na as 135–145.14 Other serum electrolytes including potassium, chloride, and phosphate were evaluated and expressed by mmol/L. Initial random serum glucose level in mg/dL, white blood cell count (WBC) in K/uL, hemoglobin concentration (Hb) in g/dL, and platelet count (PLT) in K/uL were analyzed.
Statistical analysis
Data analysis was performed using RStudio (R version 4.3.0). Categorical data were presented as frequencies and percentages, whereas numerical data were expressed as mean ± standard deviation. The association between different categories of DKA and categorical variables was assessed using a Fisher’s exact test or a Pearson’s Chi-squared test whenever applicable. Differences in numerical variables based on different DKA severity groups were assessed using a Kruskal-Wallis rank sum test. Statistical significance was considered at p<0.05.
Results
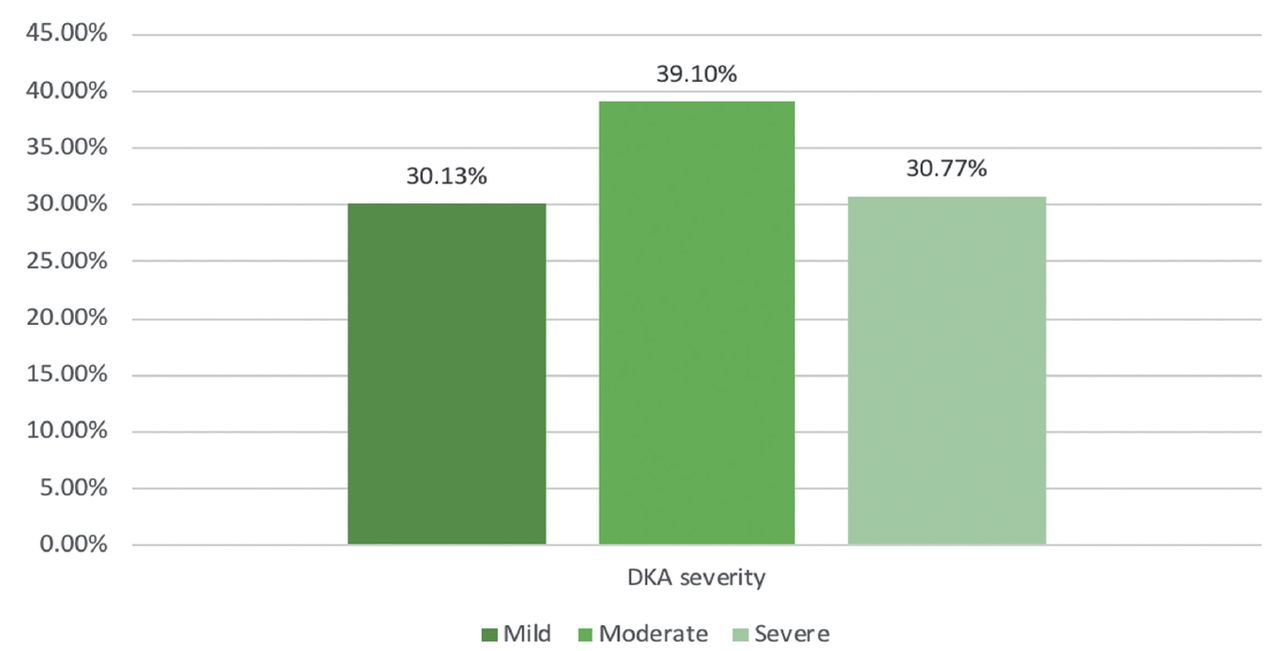
In the current study, we analyzed data of 156 pediatric patients with T1DM. More than half of them were males (54.5%), Saudis (51.9%), and in middle childhood (53.8%). Significantly higher proportions of patients with moderate and severe DKA were in early adolescence (18% and 16.7%, in sequence, compared to those with mild DKA (4.3%, p<0.001). The parents of less than half of patients had a low economic status (46.8%) (Table 1). In general, 47 patients had mild DKA (30.1%), 61 had moderate DKA (39.1%), and 48 had severe DKA (30.8%) (Figure 1).

- The proportions of diabetes ketoacidosis (DKA) severity categories among patients under study.
- Demographic and diabetes-related characteristics by diabetes ketoacidosis (DKA) severity.
In general, 52.9% of patients were newly diagnosed with diabetes, whereas 47.1% of them were known patients. Among patients with known T1DM, the mean duration of the disease was 3.3 ± 2.5 years. Importantly, a substantial proportion of these patients exhibited poor glycemic control (78.3%). The prevalence of poor glycemic control increased significantly with DKA severity among known T1DM patients, ranging from 52.4% for mild DKA to 84.8% for moderate DKA and 100% for severe DKA (p=0.002). Notably, we found a significant association between severe DKA and newly diagnosed (T1DM when compared to moderate and mild DKA (68.1% versus [vs.] 45.9% and 46.8%, consecutively, p=0.049).
The highest frequency of DKA episodes occurred during the autumn followed by the summer season, accounting for 31.4% and 28.8% of cases, in order.
Among the patients, approximately 16% had coexisting chronic diseases. Celiac disease (45.8%), attention deficit hyperactivity disorder (ADHD) (25%), and hypothyroidism (16.7%) were the most frequent, although their association with DKA severity did not yield a significant p-value (Table 2).
- Clinical presentation, associated diseases, and diabetes ketoacidosis severity (DKA).
The acute complaint duration among patients was 3.4 ± 4.1 days. In the majority of cases, DKA episodes resolved in less than 24 hours (90.4%). Diabetes ketoacidosis severity exhibited significant differences for episodes lasting between 24 and 48 hours (20.8% vs. 6.6% for moderate DKA and 0% for mild DKA) and more than 48 hours (2.1% vs. 0.0% for moderate and mild DKA, p< 0.001).
Common symptoms presentation included vomiting (72.4%) and abdominal pain (64.5%). Notably, the proportions of these symptoms increased significantly with higher DKA severity, ranging from mild to moderate and severe DKA. These signs/symptoms included a drop in the GCS score (15.0 ± 0.0, 14.9 ± 0.6, and 13.7 ± 2.0, p<0.001), decreased activity (44.7%, 55.7%, and 87.5%, p<0.001), drowsiness (14.9%, 21.7%, and 79.2%, p<0.001), Kussmaul breathing (8.5%, 27.9%, and 68.8%, p<0.001), shortness of breath (2.1%, 16.4%, and 52.1%, p<0.001), vomiting (51.1%, 77%, and 87.5%, p<0.001), tachycardia (40.4%, 57.4%, and 89.6%, p<0.001), and severe dehydration (2.2%, 11.5%, and 60.4%, p<0.001 (Table 3).
- Initial signs and symptoms, degree of dehydration, and diabetes ketoacidosis (DKA) severity.
Concerning the laboratory parameters, results showed significant increments with higher random serum glucose concentrations (408.7 ± 104.0, 424.2 ± 106.4, and 470.8 ± 100.6, p=0.008) and significant increments in the proportions of hypernatremia (0.0%, 3.3%, and 22.9%, p=0.001) among mild, moderate, and severe DKA, in sequence. Other serum electrolytes showed no significance association with episode severity. Additionally, patients with mild, moderate, and severe DKA had significantly higher counts of WBCs (10.8 ± 5.9, 11.6 ± 5.6, and 23.9 ± 10.1, respectively, p<0.001) and platelets (384.0 ± 120.4, 414.7 ± 135.3, and 493.7 ± 130.3, respectively, p<0.001, Table 4).
- Laboratory evaluation and diabetes ketoacidosis (DKA) severity.
Discussion
The urgency of DKA treatment cannot be overstated because it is a medical emergency that can lead to severe consequences. This study revealed that newly diagnosed children with T1DM were more likely to have severe DKA compared to those with known T1DM cases. In a similar study conducted in West Asia, it was reported that over half (54.4%) of newly diagnosed patients presented with severe DKA.15
This study revealed that moderate DKA was the most frequently observed type, aligning with a previous study in KSA where 67.1% of DKA cases were of moderate severity.16 Similarly, Shaltout et al17 (2016) found that during the time of diagnosis, approximately 24.8% of the children exhibited mild to moderate DKA, whereas severe DKA was present in just 8.8% of the cases.
The occurrence rate of newly diagnosed diabetes patients presenting with DKA as their initial manifestation varies across different countries. In this study, 52.9% of patients were admitted with DKA as their first presentation. A systematic review from 2012 highlighted variations among different countries. The highest frequencies of DKA presentation were observed in the United Arab Emirates (80%), Romania (67%), Taiwan (65%), and KSA (59%), whereas the lowest rates were found in Sweden (14%), Canada (18.6%), Finland (22%), and Hungary (23%).18 However, another systematic review conducted in 2016, which included multiple Arab countries, showed an overall rate of 46.7% of patients presenting with DKA. The rates ranged from as low as 17% in Egypt to as high as 100% in Morocco, Algeria, and Tunisia. Saudi Arabia had a DKA presentation rate ranging from 26-80%.19 A recent study in 2019 conducted in KSA showed that the incidence of DKA at the diagnosis of T1DM had decreased to 37.7%, owing to the increased level of education and awareness among the Saudi population.5
The occurrence of DKA does not exhibit a consistent pattern indicating a higher prevalence in one gender compared to the other. Similarly, this study showed no significant difference between both genders, though we did see a slightly higher prevalence of DKA in males (54.5%), which is consistent with studies conducted in Africa and Europe showing male prevalence of 55.4% and 51%, in order.20,21 In contrast, several studies conducted in KSA and globally have demonstrated a slightly higher incidence of DKA in females compared to males.16,22-24 Previous researchers have consistently documented a higher incidence of DKA among children in the middle childhood age group, which aligns closely with the findings of this study.16,23,25,26 It was shown that severe cases were more commonly observed in the early adolescent age group in the current study.
Several researchers reported higher DKA episodes among patients of Saudi nationality with rates exceeding 50%.23,27 In this particular study, it was noted that although the number of DKA episodes was slightly higher among Saudis, the severity of the episodes was more pronounced in non-Saudis.
Individuals from lower economic backgrounds are at a higher risk of developing severe DKA, attributed to the lack of resources and medication compliance.21 Passanisi et al28 (2023) emphasized that 54% of individuals from low-income populations presented with DKA at the time of diagnosis, and of those, 57.9% experienced a severe DKA episode. In the current study, 46.8% of participants belonged to a low economic status group, and among them, 58.3% had severe DKA.
Different studies were conducted to determine the frequency of hospitalizations for DKA and its correlation with seasonal changes. In this study we found that hospitalizations for DKA were more frequent in the autumn and summer seasons. However, other studies conducted in KSA, the western region, and West Asia showed higher incidence during the summer season.29,30 This may be due to changes in sleep patterns and increased stress levels during the summer months. In contrast, a study conducted at a tertiary care hospital in Pakistan showed that hospitalizations for DKA were higher in the winter season.6 The main reason for this difference was attributed to the length of summer in KSA and West Asia compared to Pakistan.
The present research, along with another study, has demonstrated that more time is required for DKA corrections as its severity progresses.6 This can be attributed to a higher occurrence of medical complications that necessitate medical intervention for individuals with severe DKA.
In this study we found that poor glycemic control is associated with a higher incidence of severe DKA. Fritsch et al24 (2011) demonstrated that patients with recurrent DKA had higher HbA1c levels (10.57% ± 2.09), indicating inadequate metabolic control. These results highlight the importance of effectively managing diabetes to maintain optimal glycemic control and prevent severe DKA episodes.
The severity of acidosis detected during the initial diagnosis of T1DM in children is significantly linked to the development of autoimmune disorders. It can serve as a predictive factor for the emergence of multiple autoimmune conditions. This association can be attributed to either the impact of acidosis on the immune system or the presence of a more aggressive form of diabetes. The prevalent autoimmune diseases commonly observed in these cases include autoimmune thyroid disease and celiac disease, with thyroid disease being the most frequently reported and associated with higher rates of DKA and greater disease severity.31-33 Some instances have also documented the occurrence of nephrotic syndrome.34,35 Furthermore, the presence of Human Leukocyte Antigen genes increases the risk of developing various autoimmune diseases.31 Our study revealed that celiac disease was the most commonly observed autoimmune condition (45.8%), followed by ADHD (25%), and hypothyroidism (16.7%). However, the association between the severity of DKA and these conditions did not yield a statistically significant p-value.
In relation to the initial clinical manifestations, research consistently indicates that a significant proportion of individuals presenting with DKA exhibit symptoms of vomiting and abdominal pain. According to the study conducted by Naeem et al36 in 2015, 74% of patients reported a history of vomiting, and 69% reported experiencing abdominal pain. These findings are consistent with the observations in the present study and align with results from other studies.36,23
Moreover, the severe manifestation of DKA is correlated with more pronounced clinical presentation, including reduced activity levels and a decline in GCS scores. These outcomes closely resemble the observations made in the current study.
In this study, normal Na levels followed by hyponatremia were observed. Nevertheless, another study showed hyponatremia as the most common finding.37 This occurrence of hyponatremia is polyfactorial in origin, factors including elevated triglyceride levels, recurrent vomiting, and the dilutional effect resulting from hyperglycemia, particularly among diabetic patients experiencing DKA.38,39 In this study we found that hypernatremia was more frequent among severe DKA episodes, probably related to the increase in dehydration severity. In a previous study, as DKA became more severe, the researchers noted elevated levels of hemoglobin, WBCs, and platelets, potentially due to hemoconcentration and dehydration.40 These findings imply that as DKA worsens, it leads to more profound dehydration.
Study limitations
The study was conducted at a single center, designed on the retrospective review of electronic medical records, which can introduce biases and limitations associated with data collection and documentation.
In conclusion, in this study we found that moderate DKA was the most common type with a significant number of newly diagnosed diabetes patients presenting with DKA. Severe DKA was more prevalent in newly diagnosed children with T1DM. There was a slight male predominance in DKA cases and the severity of DKA was higher in non-Saudis possibly due to economic factors. Diabetes ketoacidosis was more frequent in middle childhood and early adolescence. Seasonal variations were observed, with higher hospitalizations in autumn and summer. Poor glycemic control and specific symptoms were identified.
We recommend support programs to ensure access to health-care resources and promote medication compliance, especially among economically disadvantaged populations. Effective diabetes management is crucial to maintain optimal glycemic control and prevent severe DKA.
Acknowledgment
The authors gratefully acknowledge Proof Reading Pal (contact{at}proofreadingpal.com) for the English Language Editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 19, 2024.
- Accepted April 6, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.