


Abstract
Objectives: To determine the prevalence of Chlamydia trachomatis (C. trachomatis) infection among Saudi women, its clinical presentation, and its association to infertility.
Methods: This study was conducted between October 2012 and July 2013 at King Khalid University Hospital and King Abdulaziz University Hospital, Riyadh, Kingdom of Saudi Arabia. Female patients aged between 19 and 46 years old with infertility problems seen at both hospitals were recruited to join the study. A separate group of female patients without infertility problems was also recruited from both hospitals to serve as controls for the study. Endocervical swabs were collected from both groups of patients, and samples were analyzed using real time polymerase chain reaction.
Results: There was a statistically significantly greater prevalence of C. trachomatis infection in infertile women (n=8, 8.0%) compared with the fertile group of women (n=1, 1.0%). The C. trachomatis infection was significantly correlated to infertility.
Conclusion: A significant association between infertility and increased prevalence of C. trachomatis infection is shown in this study, thus, we suggest that screening for Chlamydial infection to be part of the routine investigation for infertility.
Infertility is a worldwide health problem among couples with approximately 15% current global infertility rate, translating to one in 6 couples suffering from this condition.1 It is a public health problem with a major economic impact on the health care system in many countries.2 According to the World Health Organization, there is an estimated 448 million new cases of sexually transmitted infections (STI’s) which are acquired worldwide annually.3 There is a multitude of bacterial, viral, and parasitic pathogens that are transmissible sexually.4 Chlamydia trachomatis (C. trachomatis) is a gram-negative bacteria and is one the most frequently reported STI. It has 3 human serovars; serovar Ab, B, Ba or C, which causes trachoma (an eye infection), serovar D to K which causes pelvic inflammatory diseases (PID), ectopic pregnancy and urethritis, and serovars La to L3 which causes lymphogranuloma venereum (LGV).5-9 The C. trachomatis is increasingly being associated with long-term complications, such as asymptomatic endometritis, cervicitis, PID, and tubal factor infertility.5-9 The association between C. trachomatis infection and infertility has been the subject of several research. A study in Iran10 suggested the significant association between C. trachomatis infection and female infertility with a prevalence rate of 15.3%. The same finding was suggested by a study conducted in India, which confirmed the significant association between infertility and the duration of C. trachomatis infection.11 Furthermore, another study suggested that a positive serology screening result for C. trachomatis is predictive for both tubal damage, and a reduced pregnancy rate.12 A prevalence rate of 9.6% was found in female patients attending the infertility clinic in a study carried out in Nigeria.13 Other prevalence rates include studies carried out in the USA (5-15% prevalence rate),8,14 UK (16%),15 Jordan (3.9%),16 Iran (22%),17 and Brazil (10.9%).18 We conducted this study to determine the prevalence of C. trachomatis infection among women attending the infertility clinic in 2 tertiary hospitals in Central Saudi Arabia.
Methods
Patients and selection criteria
This study was conducted between October 2012 to July 2013 at 2 tertiary hospitals, King Khalid University Hospital (KKUH) and King Abdulaziz University Hospital (KAUH) in Riyadh, Saudi Arabia. We recruited married female patients aged between 19 and 46 years old who were attending the infertility clinic of both hospitals. For comparison, we invited married female patients who were attending the gynecology clinic of both hospitals as the control group. The control group were of the same age group as the infertile group, provided that they never consulted the clinic for any infertility problem. Women who had a history of medical or surgical diseases, were pregnant at the time of the study, and who had taken antibiotics 30 days prior to the study were excluded from this study. Both groups fulfilled the inclusion criteria during the period of the study and agreed to participate by signing an informed and written consent. The Institutional Review Board of King Saud University granted the approval for the conduction of this study.
Demographic characteristics of the patients were noted using a preformed data collection sheet. Signs and symptoms including burning micturition, genital bleeding, irregular menstruation, vaginal discharge, lower abdominal pain, history of PID, abortion, ectopic pregnancy, premature delivery, low birth weight, and infertility duration were also obtained. The type and etiologic cause of infertility was also obtained from the infertility group of patients. Physical pelvic examination was conducted by a gynecologist.
Specimen collection
Two endocervical swabbing by speculum examination were carried out to all patients by the attending gynecologist. The first swab was used before sampling to clean off the excess mucus, while the second was rubbed and were rotated several times over the endocervical cells in the cervical canal to collect samples for assay. Swabs were withdrawn from the cervical canal without touching the vaginal surface, and were placed into the Copan universal transport medium (UTM-RT, Copan Medical Diagnostic Laboratories, Hamilton, New Jersey, USA). All swabs were stored at 4°C until transported to the laboratory. The DNA extraction was performed using automated DNA extraction by MagNA Pure Compact Nucleic Acid Isolation Kit and MagNA Pure Compact system by Roche Diagnostics, Indianapolis, Indiana, USA. A 136 bp fragment of the C. trachomatis genome gene was amplified with specific primers and detected with probes labelled with Light Cycler Red 640 (Roche Diagnostics, Indianapolis Indiana, USA). The polymerase chain reaction (PCR) was monitored by an additional PCR product of 278 bp. The master mix for real time PCR was prepared using LightCycler® Fast Start DNA Master HybProbe (Roche Diagnostics, Indianapolis, Indiana, USA). To avoid contamination, mixing of the reagents (except of the DNA template) was performed in a separate room, away from the room where DNA purification were carried out. The reaction mixture was prepared in a cold reaction tube, 15 µl of the reaction mix was transferred to a light cycler 2.0 capillary. A 5 µl of template DNA was added to each capillary for a final reaction volume of 20 µl. One negative control was always included in each run by replacing the template DNA with water. A positive control was included in each run by replacing the template DNA with one of the control DNA from the standard row provided with the light mix kit (TIB Molbiol, Germany). The LightCycler PCR program was composed by: fast start Taq DNA polymerase activation carried out in 95°C for 10 minutes, followed by cycling: 95°C (20°C/second [s]) for 5 seconds, 55°C (20°C/s) for 5 s, and 72°C (20°C/s) for 15 s, repeated 50 times. Melting assay ended the analysis: samples were heated to 95°C (20°C/s) hold for 20 s, cooled to 40°C (20°C/s) hold for 20 s, and then heated slowly at 0.2°C/s up to 85°C, finally cooled to 40°C (20°C/s). The PCR results were obtained within 50 minutes (50 cycles and melting curve); data analysis was performed, as described in the LightCycler instrument operator’s manual.
Statistical analysis
All collected data were encoded and analyzed using the Statistical Package for Social Sciences version 19.0 (IBM Corp., Armonk, NY, USA). We present the frequencies and percentages for different items of nominal variables, and mean, standard deviation and range for numerical variables. We used chi-square test to compare between infertile group and the non-infertile group, and to compare between primary infertility and secondary infertility with respect to all nominal variables. For smaller number of cases, we used Fisher’s exact test to compare between variables. Correlation between variables was carried out using the Pearson correlation. We assumed there was a statistically significant when p<0.05.
Results
A total of 100 infertile women consented to join the study. Another 100 women who were not infertile but attending the gynecology clinic at both hospitals also consented to join the study as a control group. The mean age of all patients was 33.4 ± 4.7 years old (range: 19-46 years old). The mean age of the study patients (the infertile group) was 32.5 ± 4.4 years old (range: 19-46 years old). The mean age of the comparison group (the gynecology patients without infertility) was 34.1 ± 4.3 years old (range: 19-46 years old). There was no statistical difference in the mean age between the study and the comparison group (p>0.05. Eight women (8%) tested positive for C. trachomatis from the infertility group. In the infertility group, 5 patients who tested positive for C. trachomatis had low-seated abdominal pain (19%), all 8 infertile cases had irregular menstruation, and one patient complained of burning sensation (6%). One case who was positive for C. trachomatis complained of abnormal discharge (5%). The single case of previous abortion was positive for C. trachomatis. The distribution of positive cases among infertility factors is shown in Table 1. Women testing positive for C. trachomatis among primary infertility group (5/57, 9%) were higher than positive cases among secondary infertility group (3/43, 7%) with no significant difference (p=0.722). The C. trachomatis infection had the highest prevalence among the age group of 19-25 years (3/16, 19%), one positive case from the age group 26-32(1/43, 3%), 2 positive cases from the age group 33-39(2/35, 6%), and 2 positive cases from the age group 40-46 (2/15, 13%). There was no significant differences between the C. trachomatis positive cases in between the different age groups (p=0.177). Infertility was significantly positively correlated to C. trachomatis infection (Pearson r=5.701, Fisher’s exact p=0.035).
Positive cases according to infertility factor among the studied group.
Melting curve analysis of C. trachomatis samples
Melting curve and melting peak analysis of C. trachomatis isolates was performed. Isolates were identified through the specific melting points at approximately 66°C, and ranged between 66 and 66.5, with the control at 66.3. (Table 2).
Melting curve analysis of Chlamydia trachomatis sample among the studied group.
Absolute quantitative real time PCR results
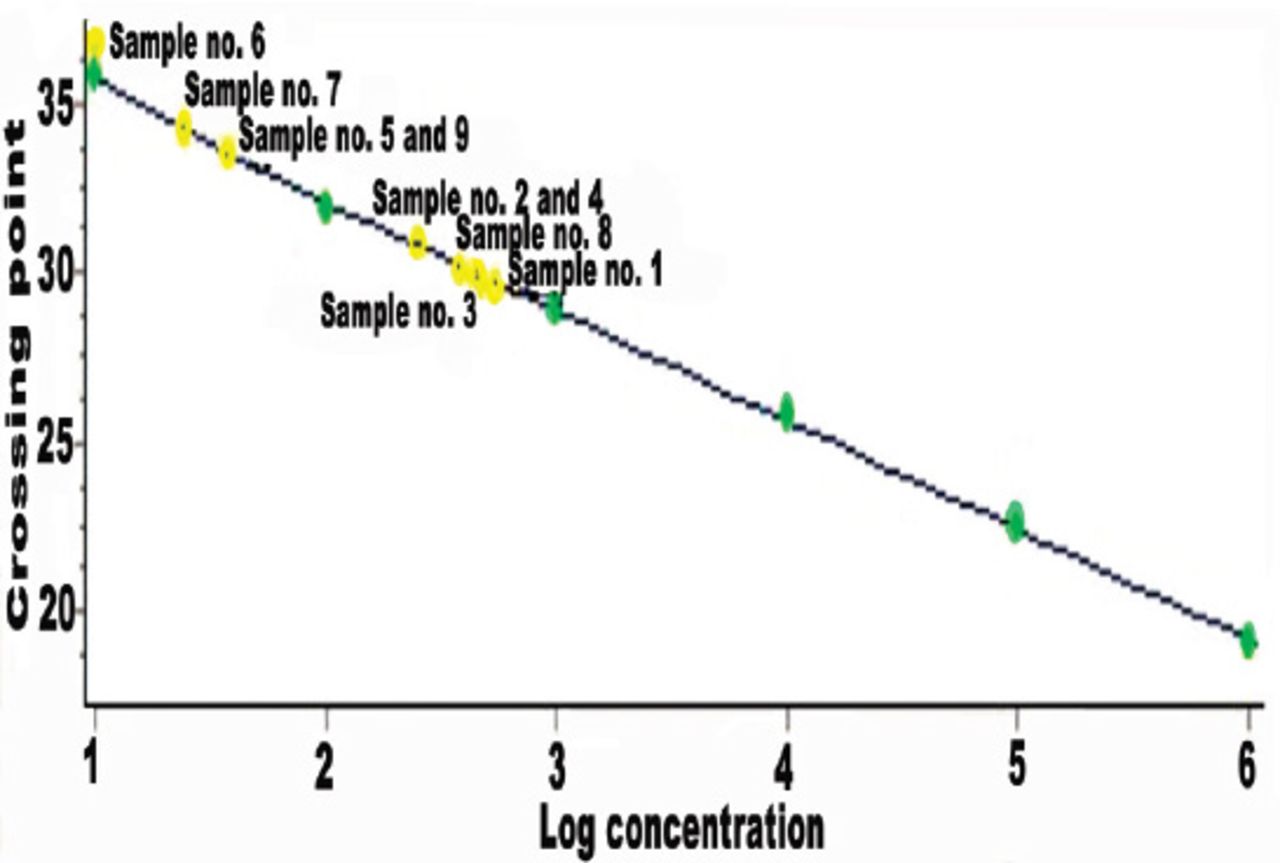
All the positive samples of C. trachomatis were subjected to confirmatory testing to determine the concentration of PCR products. Data analysis was performed as described in the LightCycler instrument operator’s manual. The provided standard row of cloned and purified DNA of C. trachomatis with concentrations in the range from 106 copies/reaction to 101 copies/reactions of DNA were included, and were used to determine the exact amount of template of these positive samples. The cycle number of the crossing point (CP) and the copy number of each sample was calculated automatically. The negative control showed no signal. Samples with high DNA load had low CP values, and low DNA load had high CP values. The absolute quantitative real-time PCR run of C. trachomatis positive results, its CP, and the standard dilution series of standard DNA are shown in Tables 3 & 4. The amplification curves of the standard dilution series along with C. trachomatis positive samples is shown in Figure 1, and the standard curves of C. trachomatis positive samples is shown in Figure 2.
Absolute quantitative real time polymerase chain reaction run of the standard dilution series of standard DNA.
Absolute quantitative real time polymerase chain reaction run of Chlamydia trachomatis positive samples.

Amplification curves of the standard dilution series along with Chlamydia trachomatis positive samples.

Standard curves from standard dilution series 106 copies down to 101. Chlamydia trachomatis positive samples crossing points are shown by yellow dots.
Discussion
The C. trachomatis is not screened by routine examination of endocervical specimens in health laboratories in Central Saudi Arabia. This study employed real time PCR with hybridization probe format by LightCycler PCR protocol with both qualitative and quantitative detection of C. trachomatis. The present study aimed to determine the prevalence of C. trachomatis in women with infertility problems and the prevalence was compared to the prevalence among women without infertility issues as a control group. This study provides some salient points worth highlighting the role of C. trachomatis in the female reproductive organ pathology. The findings of this study highlighted the need for a Chlamydia screening program as C. trachomatis is known to be one of the most frequent pathogen affecting female patients. This study showed a significantly higher prevalence of C. trachomatis infection in the infertility group (8%) versus 1% prevalence in the comparison group. This prevalence is relatively similar to studies conducted in the United States, with prevalence rates ranging from 5-15%.14 Our study showed higher Chlamydial infection rate among infertile and control groups compared to a similar study conducted among Jordanian women with a prevalence rate of 3.9%.16 Some other studies conducted in other parts of the world have shown greater incidence, one example is the 16% prevalence rate found in a UK study,15 40% in Jordan,16 and 22% in Iran.17
The C. trachomatis infection rate among our comparison (control) group was only 1%. This is in contrast to other studies that reported higher prevalence (6% and 8%) of C. trachomatis infection in healthy patients.18,19 The association between Chlamydial infection and low abdominal pain among our patients may be a sign for PID since untreated pelvic infections can spread upward to the uterus and the fallopian tubes. The PID can be silent, or can cause symptoms such as abdominal and pelvic pain.
All our positive samples had melting peaks with Tm values from 660 to 66.50, which determines how well the sequence of probes matches the sequence of template DNA. Melting peaks decreases if mismatched DNA is amplified. A quantification of DNA concentrations was based on standard dilution series with known concentrations of genomic C. trachomatis DNA. As an external reference standard, concentrations of standard dilution series, there was a variation in the DNA copy-number loads, samples with high DNA load had low CP values, and low DNA load had high CP values. Chlamydial positive sample number 1 from the infertile group showed the highest template count copy number of 6880 DNA copies/reaction (1,376,000 copies/ml). The sample was collected from a 34 year-old primary infertile with tubal factor infertility, complaining of low abdominal pain. Chlamydial infection may be a marker for exposure to other STI’s. One possible explanation is an increased risk of PID related to C. trachomatis infections, which are very common.7 However; a low-copy number region was demonstrated with sample number 6 of the infertility group. Sample number 6 had a copy number of 8.45 DNA copies/reaction (1690 copies/ml, showing low concentration, and a melting curve with the melting peak around 66°C, thus was therefore considered as positive.
The significantly positive correlation between infertility and infection with C. trachomatis shown in this study suggests that there is a linear relationship between infection with C. trachomatis, and the greater prevalence of infertility cases in this group of women. This study however was not able to identify other confounding factors, such as the number of sexual partners because the society limits us to do so, and other sociodemographic factors that may play a role in the increase prevalence of C. trachomatis infection among infertile women.
In conclusion, there is a higher prevalence of infertility among women who had C. trachomatis infection, as shown by the significant correlation between infertility and C. trachomatis infection. This calls for a national screening program for the early detection of C. trachomatis infection among infertile couples in Saudi Arabia. Future studies on C. trachomatis is warranted to identify predictors and other confounding factors, which will further enhance our knowledge on the pathophysiologic spectrum of infertility, and STI’s as a whole.
Ethical Consent
All manuscripts reporting the results of experimental investigations involving human subjects should include a statement confirming that informed consent was obtained from each subject or subject’s guardian, after receiving approval of the experimental protocol by a local human ethics committee, or institutional review board. When reporting experiments on animals, authors should indicate whether the institutional and national guide for the care and use of laboratory animals was followed.
Footnotes
Disclosure. This study was supported by a grant from the Research Center of the female Scientific and Medical Colleges, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia.
- Received July 22, 2014.
- Accepted November 23, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.