


Abstract
Objectives: To investigate the origin, prevalence, and possible effects of peroneus digiti quinti muscle (PDQ) on the fifth toe, to find out the variations of PDQ by determining the relationship between peroneus brevis muscle (PB) and PDQ, and to reveal its importance for the applications in foot and ankle surgery.
Methods: This study was conducted at the Faculty of Medicine, Kahramanmaras Sutcu Imam University, Kahramanmaras, Turkey between September 2013 and June 2014. The study was a prospective dissection of cadaveric lower limbs. Twenty-five amputated lower limbs were stored in the freezer at -15°C. The legs were dissected; prevalence and variations of peroneus digiti quinti were investigated.
Results: Peroneus digiti quinti muscle was found in 8 (32%) of 25 dissected lower limbs. However, 2 different tendon extensions were found at 3 (37.5%) of 8, and 5 (62.5%) of them were determined to have a single tendon.
Conclusion: The incidence, dimensions, length, and insertions of peroneus digiti quinti are important in the evaluation and treatment of functional loss of the fifth toe, lateral foot deformities, and tendon problems behind the lateral malleolus of the ankle.
There are 2 peroneal muscles in the lateral compartment of the leg. Peroneus longus muscle (PL) is longer than the 2, passing behind the lateral malleolus (LM), and enters a groove under the cuboid bone and reaches its attachment at the base of first metatarsal bone. Peroneus brevis muscle (PB) is the shorter one, passing behind LM, and attaches the tuberosity of the fifth metatarsal bone.1,2 However, due to developmental factors, it is claimed that the variations, or rather accessory tendons of these muscles are quite common.3 Variationally, there may be various accessory tendons, the incidence of which changes from one population to another, such as peroneus tertius muscle (PT), and peroneus digiti quinti muscle (PDQ), and particularly peroneus quartus muscle (PQ).4-7 Generally, these muscles arise from peroneus brevis but their insertions exhibit variabilities.8 Peroneus quartus muscle inserts on the calcaneus and adjacent structures,9 PT inserts on the base of the fifth metatarsal bone10 and PDQ inserts on the fifth toe.3 The presence of PQ was reported to be approximately 22%,11-13 and PT to be approximately 10%.10 The prevalence of PDQ is so varied in the literature that it was reported by Reimann14 as 79.5%, and by Jadhav et al15 as 51%. Peroneus digiti quinti muscle extends as a small slip from the tendon of PB to the extensor aponeurosis,15,16 or proximal phalanx of the fifth toe.6 Peroneus digiti quinti muscle is innervated by superficial fibular nerve just like PB.17,18 Moreover, in some studies, it is stated that PDQ is innervated by the accessory deep peroneal nerve.18 Generally it is reported that PDQ, the diameter of which varies from 0.7 to 3 mm, does not have any kind of function since it has a really small muscle belly and a thin tendon.14 Generally, accessory muscles are asymptomatic, and they can lead different clinical symptoms related to vessels, nerves, and tendons.17,19 Peroneus digiti quinti muscle is also an asymptomatic accessory muscle, which means that it does not cause any pain, or neurological disorder.15 In a study carried out by Macalister,25 Yammine stated that in cases that PQ developed fully, PDQ arose from PQ, and reached the fifth proximal phalanx and contributed to the extension of the fifth toe.3 According to some other articles,6,15 PDQ is usually separated from PB, and there is insufficient information regarding its function. It has been only stated that PDQ partially pronates the fifth toe.20 Loss of function can be observed at muscle-tendon units of toes due to traumatic or non-traumatic reasons, and the muscle-tendon units can lose their primary functions. Tendon anomalies may confuse the clinicians during evaluation of their functions. In order to evaluate the function and anatomic structure of the foot, it is necessary to know the function, morphology of the muscles and tendons, as well as their anomalies. Peroneus digiti quinti muscle, when present, can be used as an accessory muscle and it can contribute to the extension of the fifth toe, since it ends on the dorsal aponeurosis of the fifth toe. Therefore, the aim of this study was to: 1) investigate the origin, prevalence, and possible effect of PDQ on the fifth toe, 2) to find out the variations of PDQ by determining the relationship between PB and PDQ, and 3) to reveal its importance for the applications in foot and ankle surgery.
Methods
This study was designed as a prospective dissection of cadaveric lower limbs. The prevalence of PDQ, its sites of origin and insertion, as well as its dimensions were documented. This study was conducted at the Faculty of Medicine, Kahramanmaras Sutcuimam University, Kahramanmaras, Turkey between September 2013 and June 2014. Twenty-five adult cadaveric amputated lower limbs (age range 40-65 years) of either gender were stored in the freezer at -15°C until dissection. After removing from the freezer and 12 hours waiting period at room temperature, the legs were carefully inspected, and only the ones without any foot deformity were included in the study group. The legs with bony deformities and severe degree of necrosis were excluded. The dissection procedure was carefully performed from the lateral compartment of the leg to the distal phalanx of the fifth toe. After the skin and subcutaneous tissues were discarded, PL and PB were separated from each other with their fasciae, and the surrounding soft tissues were removed. When PDQ was encountered, its sites of origin, insertion, and dimensions were measured using a millimetrically designed measuring tape. A digital camera from the same distance photographed all specimens. Then the foot was brought to its neutral standing position and measurements of PB were obtained in a standard way. Tendon length and the distance between the insertion and end point of muscle fibers of PB were determined; for the other measurements, the tip of LM was used as the landmark. As a result of the dissections, it was seen that in some extremities PDQ muscle separated from PB as a thin tendon, in the others it splitted off into 2 separate tendons. Data were recorded into the computer and Statistical Package for Social Sciences version 15 (SPSS Inc., Chicago, IL, USA) was used for biostatistical analysis. Means were compared by Student’s t-test. Pearson’s Chi-square test calculated the percentage in presence and absence group. The level of significance was set at p<0.05.
Results
Peroneus digiti quinti muscle was found in 8 (32%) of the 25 dissected lower limbs (Figure 1), with an insertion to the dorsolateral of the fifth toe (involvement of the proximal and middle phalanges, [Figure 2]), and lateral to the extensor digitorum longus muscle-tendon, dorsolateral of the fourth metatarsal, and dorsomedial of the fifth metatarsal bone (Figure 3). However, 2 different tendon extensions were found in 3 (37.5%) of 8, and 5 (62.5%) of them were determined to have a single tendon. There was no significance between the percentage of PDQ’s presence, and the dimensions of the PB tendon (p>0.05).
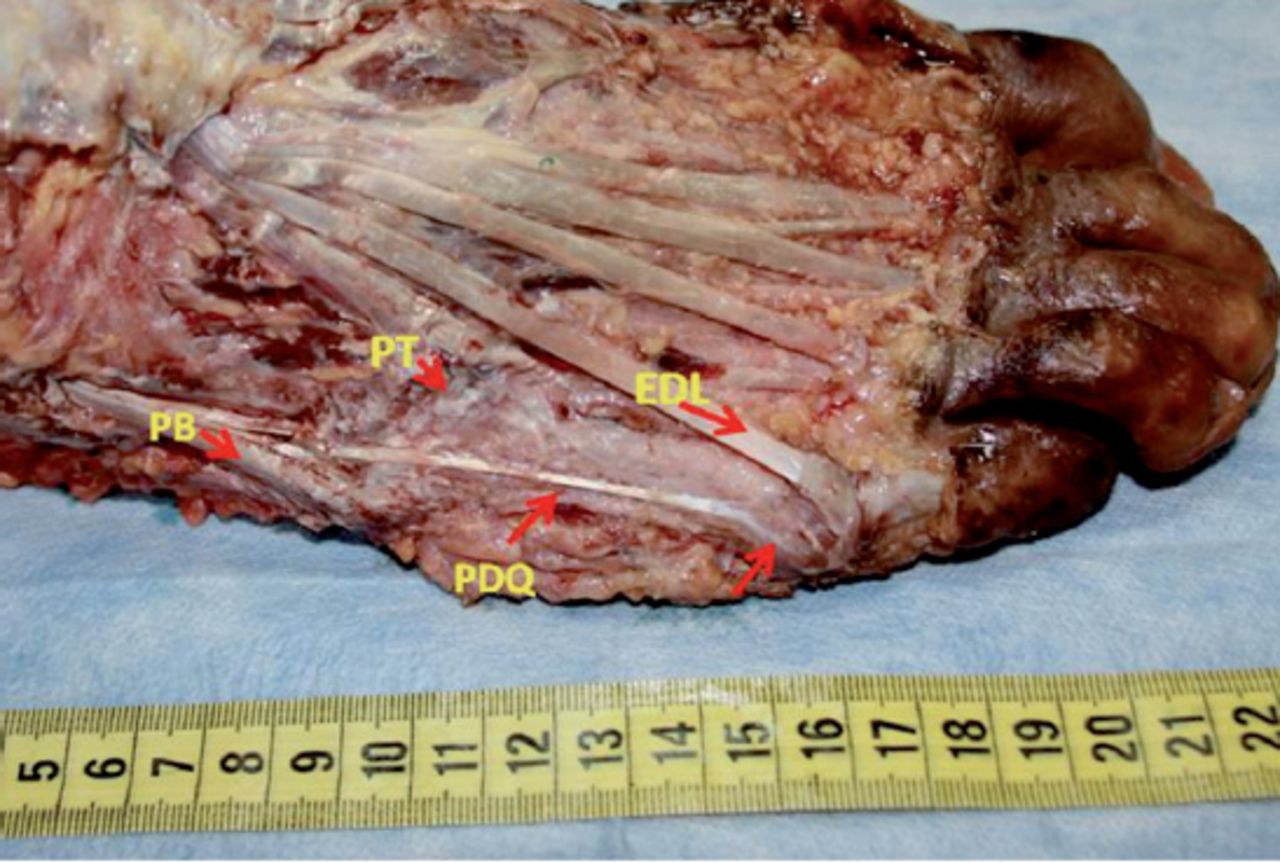
Peroneus digiti quinti muscle (PDQ) separated from peroneus brevis muscle (PB) proximal to its insertion and extended to dorsolateral aspect of the fifth proximal phalanx. EDL - extensor digitorum longus muscle, PT - peroneus tertius muscle
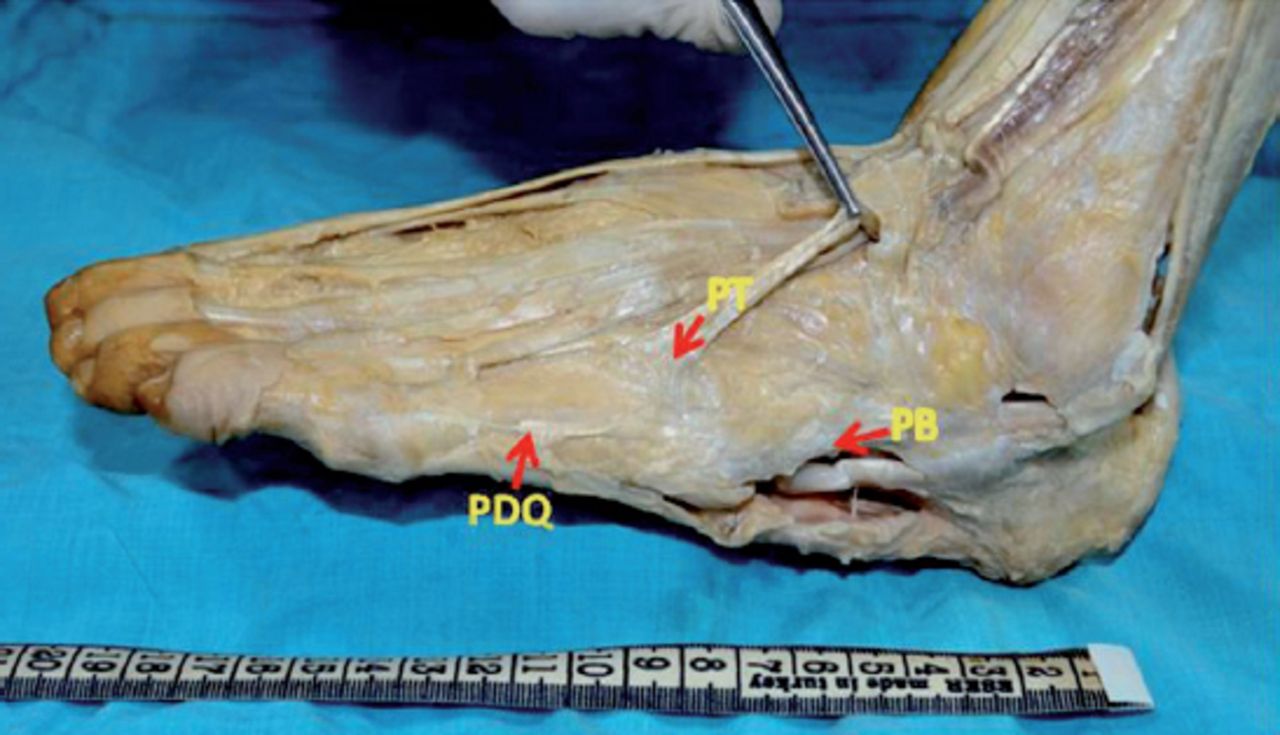
Peroneus digiti quinti muscle (PDQ) extended to dorsolateral aspect of the fifth metatarsal bone more distal to peroneus brevis muscle (PB) insertion. PB - Peroneus brevis muscle, PT - Peroneus tertius muscle

Peroneus digiti quinti muscle (PDQ) ended more distal to insertion of peroneus brevis muscle (PB) between dorsolateral aspect of the fourth and fifth metatarsal bones. PL - peroneus longus muscle
Peroneus brevis tendon length, the size at insertion point, and the size at the level of LM were measured (Table 1). While PB tendon length was found as 223±23 mm, the distance between the beginning of the tendon and LM was found to be 149±16 mm. Thus, the distance between LM and PB insertion was determined approximately 74±16 mm. Peroneus brevis muscle was in the size of 12×4 mm at the point one cm proximal to the insertion and thicker at its site of insertion than it was at the level of LM or above. It was detected that PDQ separated from PB posterior to the LM as single or double tendinous bands, which arose from the dorsolateral side of the PB tendon. Peroneus digiti quinti muscle separated from PB at 40 mm proximal to LM. Single tendons were in the size of 3×2 mm, 2×1 mm, and 1×1 mm. The PDQ extended as 2 tendons in 3 limbs, and these tendons were somehow larger than the single tendons (Table 2). The insertion of PDQ also varies. It was observed that PDQ attached to the dorsolateral aspect of the fifth metatarsal bone, or extended to the dorsolateral aspect of the fifth toe in 3 extremities. In addition PDQ was found to extend to the fourth metatarsal bone in parallel with fourth extensor digitorum longus (EDL) tendon and terminated on the dorsal aponeurosis between the fourth and fifth metatarsal bones in one extremity (Table 3).
Measurements obtained from the peroneus brevis muscle (PB) in this study.
Measurements taken on peroneus digiti quinti muscle (PDQ).
The insertions of peroneus digiti quinti muscle (PDQ).
Discussion
Extensor muscle of the fifth toe is EDL, and this muscle has evolved from extensor hallucis longus muscle in collaboration with PT and PB muscles.21 However, PB makes eversion of the foot and plantar flexion, while PT is participating in foot extension, since it is attached to the dorsum of the fifth metatarsus.22 Peroneus brevis muscle does not usually send extensor tendon to the fifth toe. Extra tendon extensions were detected with a rate of 32% during our dissections, which coursed distally and ended on the dorsal aponeurosis of the fifth toe, and when traction was applied to PB, partial extension of the fifth toe was observed (Table 4). Tendon pathologies constitute an important part of musculoskeletal problems in the foot and ankle. When situations like tendon ruptures, tenosynovitis, or tendinopathies occur, the muscle weakens and cannot perform its function fully.23 In such cases, if the subject has PDQ then it may partially extend the fifth toe or may have suspensory (tenodesis) effect on it. The pain behind the LM on the ankle is not a rare complaint and some of the painful conditions stem from tendon problems. Peroneus digiti quinti muscle has tendon slip(s) splitted up behind the LM. Hence, it may confuse clinicians while evaluating and treating some of the foot and ankle problems.
Characteristics of studies on the prevalence of peroneus digiti quinti muscle.
There are no precise data on the incidence of PDQ in the literature, and the studies are mainly based on the findings of many years ago.24 Bhargava et al25 gave the incidence of PDQ as 15.5%. Reimen14 reported the presence of PDQ as 79.5%. Based on these data, Yammine3 stated that there were differences regarding incidence of PDQ and declared that ethnicity was important in considering the incidence of PDQ in each community. We found the incidence of PDQ as 32% in our specimens. However, unlike other studies, we identified that PDQ sometimes can be found as 2 separate tendons, and that insertional sites can vary from each other. Besides, there is no clear information on the function of PDQ in mentioned studies. For example, we identified that PDQ arose from PB as 2 separate tendons, one of them attached to the dorsal aponeurosis of the fifth toe, and the other one attached to the base of the fifth metatarsal bone, and when a traction force was applied to both tendons, the fifth toe was brought into extension. Jadhav et al15 studied on 100 lower limbs and declared that the incidence of PDQ was 51% in India. In their study, the insertion location of PDQ was classified as well, but there was no information regarding its probable presence as in the form of 2 separate tendons.
In our study, we tried to determine the dimensions and length of PDQ and PB. The width and thickness of PB at the level of LM and the distance between LM and its insertion were measured. The distance between tendon starting point and insertion of PB was 233 mm; the distance between tendon starting point and LM was 149 mm. Since PB expands and attaches to the base of the fifth metatarsal bone, its width was 12×4 mm at a point one cm proximal to its insertion and 10×4 mm behind LM. While we measured the width x thickness of PDQ as 3×2 mm, 2×1 mm, and 1×1 mm, Jadhav et al15 measured corresponding sizes between 0.7 and 3 mm. According to Bergman et al,16 insertions of PDQ were dorsal aponeurosis of extensor digitorum brevis muscle or head of the fifth metatarsal bone and moved together with dorsal aponeurosis of the fifth toe or PT.16 However, we observed that PDQ attached to dorsolateral of the fifth toe in 36%, to the base of the fifth metatarsal bone in 27% and moved together with EDL tendon in 18% of cases. Since 25 cases were dissected in an East Mediterranean city of Turkey, the results may represent only the population in that region, but not the whole Turkish population. Further dissections in other regions of Turkey will contribute to the collection of nation-wide data.
In conclusion, variational tendon anomalies may exist in lateral compartment of the leg, as well as on the dorsum of the foot. Primarily PDQ can contribute to the extension of the fifth toe and interfere with the functions of EDL. Furthermore, these extra tendons may exert tenodesis effect that prevents flexion posture of the toe in EDL tendon injuries. These anatomic variations, which are the causes or consequences of developmental abnormalities, must also be taken into account in the evaluation and treatment of functional loss of the fifth toe, lateral foot deformities and also tendon problems behind the LM on the ankle.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received July 1, 2015.
- Accepted October 5, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.