


Abstract
Brain abscess due to Entamoeba histolytica (E. histolytica) may pose a diagnostic problem or a therapeutic challenge, as evidenced by the paucity of papers reporting complete recovery after treatment. An 11-year-old girl presented with progressive drowsiness, diminished movements of the left upper limb, and swallowing problems. Cranial MRI showed multiple, contrast-dense masses with fluid content. She was started on meropenem. Surgical drainage was performed. No bacterial or fungal growth was observed in drainage samples. Entamoeba histolytica trophozoites were detected in the tissue sample. Intravenous metronidazole was started and continued for 6 weeks, at the end of which abscesses were found and to have shrunk considerably. Intravenous therapy was switched to oral metronidazole, which was continued for 2 weeks. She regained all her preexisting abilities. Multiple brain abscesses due to E. histolytica is a very rare occurrence, and histopathologic evaluation is important in diagnosis.
Brain abscess, a rare form of Entamoeba histolytica (E. histolytica) infection, is characterized by an abrupt onset of symptoms and rapid progression and early death if untreated. Although many erroneously consider it as a disease of economically-developing countries, brain abscess due to E. histolytica may pose a diagnostic problem or a therapeutic challenge as evidenced by the paucity of papers reporting complete recovery after treatment. Extra-abdominal amebiasis, including cerebral amebic abscess, develops as a complication of hepatic amebiasis, rather than direct dissemination from the intestine. Cerebral amebic abscess disease has an incubation period starting from a few days to several months. As cerebral bacterial infections have a medical profile similar to that of protozoans (including partial muscular weakness, lethargy, and headache) differential diagnosis is difficult. The aim of the current study is to present a case of a brain abscess not associated with hepatic amebiasis.1-3 Multiple brain abscesses due to E. histolytica is a rarely seen occurrence. Serological and histopathological evaluations may prove to be very important in the diagnosis.
Case Report
An 11-year-old girl with cerebral palsy presented with progressive drowsiness, diminished movements of the left upper limb, and swallowing problems for the last 7 days. She was hospitalized with a prediagnosis of encephalitis. Physical examination revealed an unconscious child with spontaneous and non-uniform movements. She was unresponsive to verbal stimuli, but tried to avoid painful stimuli with flexion. Her white cell count was 22,600/µL (4600-10200/µL) with a predominance of neutrophils. The C-reactive protein was 4.4 mg/dL (0.5 mg/dL) and erythrocyte sedimentation rate was 51 mm/hour (20 mm/hour). The EEG did not show any epileptiform activity. Cranial MRI revealed multiple, contrast-dense masses with fluid content and circumferential edema in the right frontotemporoparietal region (Figure 1). The right lateral ventricle was entirely closed and there was a 2-cm shift. She was started on meropenem and surgical drainage was performed. The drainage fluid showed abundant leukocytes. Bacterial and fungal cultures yielded no growth. She had to undergo another surgical drainage due to abscess, shift and persistent cerebral edema.

Cranial MRI revealed multiple, contrast-dense masses (abscesses) with fluid content and circumferential edema in the right frontotemporoparietal region (arrows).
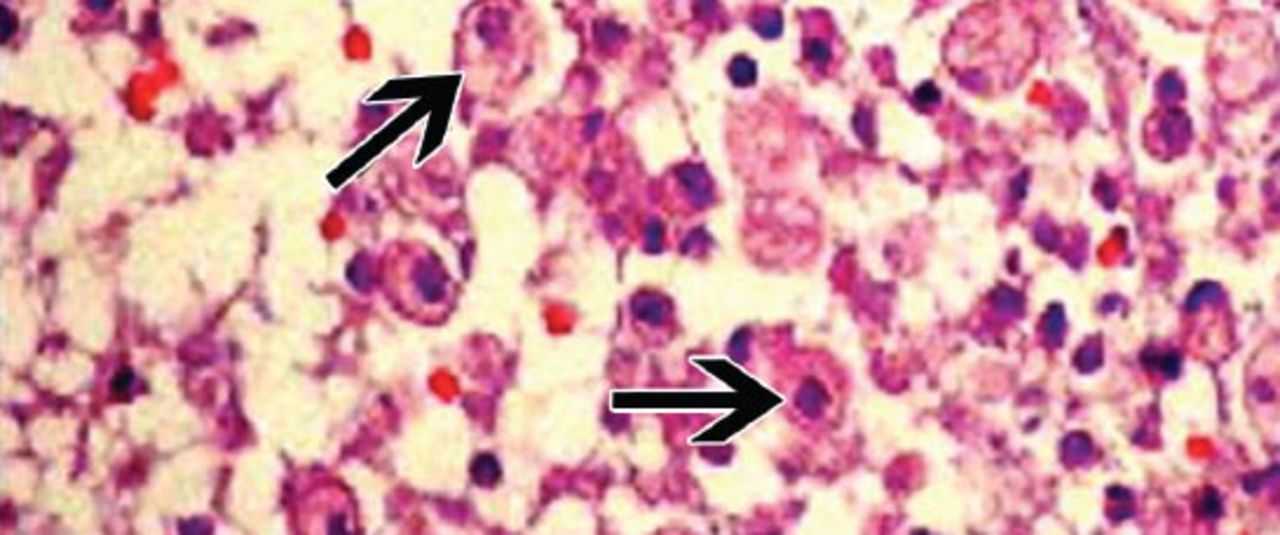
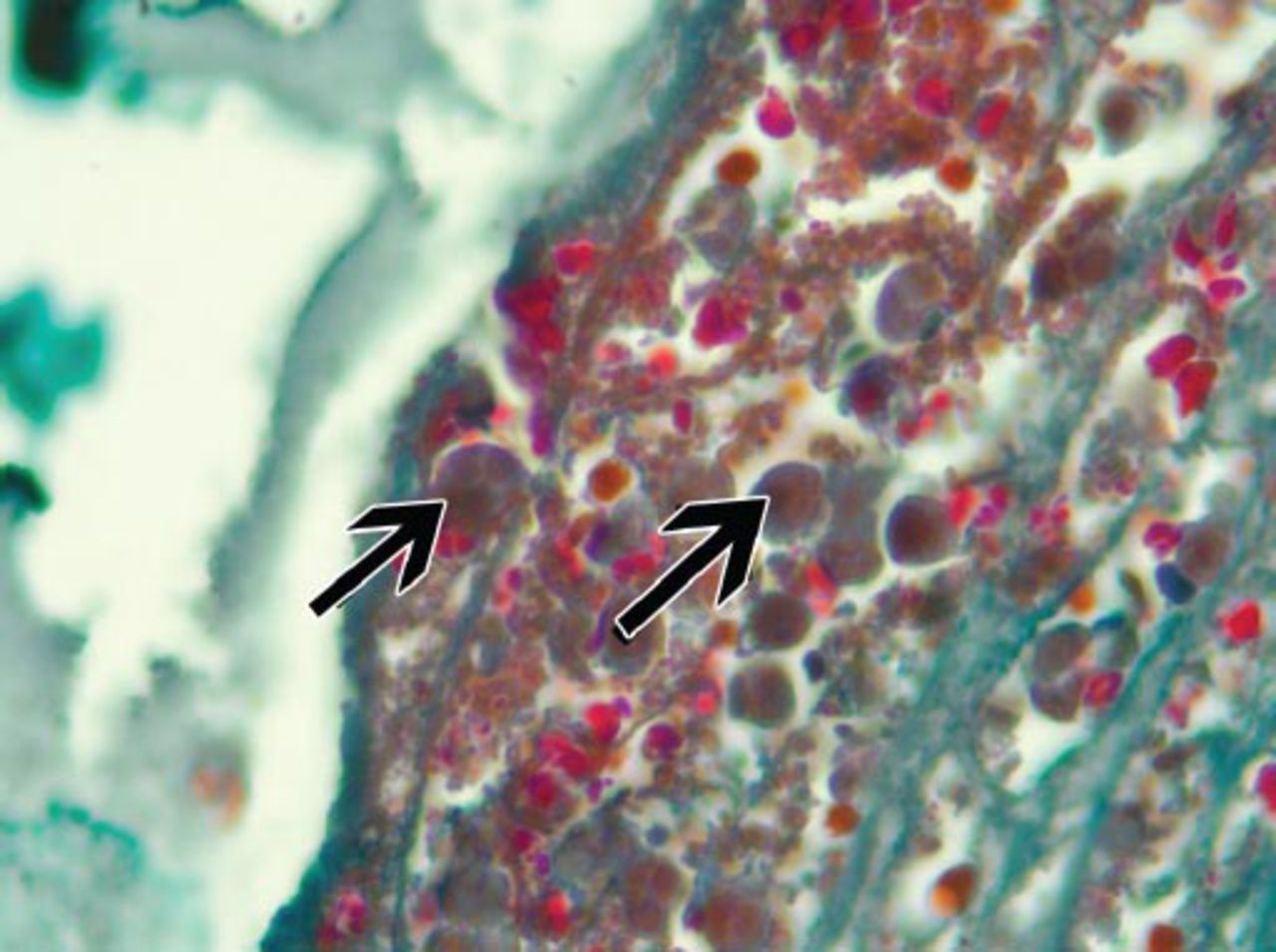
No bacterial or fungal growth was observed in the drainage samples. The histopathologic examination of the abscess capsule revealed necrotic material with a diffuse infiltrate of polymorphonuclear leukocytes, lymphomononuclear cells, foamy histiocytes, rare esinophils, and Masson’s trichrome-positive, spheric structures, measuring 20-25 µm in diameter with eccentrically placed nuclei and ingested erythrocytes, consistent with E. histolytica trophozoites (Figures 2 & 3). Parasitologic stool examination and abdominal ultrasonography was normal. Intravenous metronidazole was started and continued for a period of 6 weeks (the first 3 weeks in hospital), at the end of which the abscesses were found to have shrunk considerably, but not resolved completely. Another surgical drainage of the brain abscesses was planned; however, this was rejected by her family. The intravenous therapy was switched to oral metronidazole, which was continued for 2 weeks. At the time of cessation of the antimicrobial therapy, she regained all her preexisting abilities, such as making eye contact with her parents, smiling, and even handshaking. A CT with contrast enhancement showed no pathologic signs except for a residual abscess cavity, which made it clear that the infection had disappeared.

Amebic trophozoites as shown with arrows. Note the neutrophilic and lymphomononuclear infiltrates (Hematoxylin & Eosin) (x400).

Entamoeba histolytica trophozoites as shown with arrows (Masson’s trichrome stain x400).
Discussion
The diagnosis of amebic brain abscesses is difficult.4-6 History of headache or sensorial disturbances and cranial nerve involvement, such as the swallowing difficulty seen in our patient, is frequent. Symptoms and signs of CNS infection, such as the progressive drowsiness and diminished upper limb movements observed in our patient, may also occur. Cerebral palsy was a considerable addition to the diagnostic challenge in this patient. Amebic brain abscesses may be single or multiple, their most common sites of involvement being the frontal lobes, as in our case, and basal ganglial regions. Left brain, contrary to the site in our patient, is more commonly involved than the right side. The CT images of E. histolytica abscesses are indistinguishable from those CT images due to other organisms. Intestinal symptoms have been found in 50% of the cerebral amebiasis cases. Our case is one of the very few cases reported in the electronically searchable literature. Entamoeba histolytica is the only member of the Entamoeba genus recognized to cause brain abscess. Entamoeba moshkovskii may cause diarrhea, and Entamoeba dispar is nonpathogenic.2 The absence of evidence of amebiasis in the abscess fluid and elsewhere in the body may cause the erroneous presumption of bacterial etiology with starting and continuing antibacterial therapy, as was the case in our patient. Currently, diagnosis of cerebral amebiasis is accomplished with a combination of CT or MRI findings and the use of serological methods. Recently, the usefulness of polymerase chain reaction, especially in the absence of microscopic demonstration of the parasite, has been reported.7-9 Serologic and nuclear acid detection techniques were not available for our patient. Pathologically, amebic abscesses range from early lesions, which have poorly defined, irregular borders to mature lesions, which are “true” abscesses with central tissue necrosis and inflammatory cells (made up of mainly round cells). Trophozoites typically measure approximately 25 µm in diameter and contain a single, round nucleus (5 µm), and a vacuolated cytoplasm. The presence of ingested red blood cells is considered to be pathognomonic for E. histolytica. It was noteworthy to witness the curative efficacy of oral metronidazole in the treatment of an amebic brain abscesses, at least following several weeks of intravenous therapy. Although amebic brain abscess is a rare form of invasive amebiasis, it must be diagnosed in a timely manner to preserve the life of the patient. Therefore, E. histolytica should always be considered in the etiologic diagnosis of a brain abscess. The person assessing the tissue specimen (the pathologist or in this case, the parasitologist) should be vigilant since she/he may be the only person to establish the diagnosis of an amebic brain abscess, and the clinical diagnostician may be the only person to draw and canalize the attention of the laboratory diagnostician to a possible amebiasis.
New Peer Reviewers
Join our team of expert peer reviewers for the Saudi Medical Journal by sending an enquiry and summarized CV to info{at}smj.org.sa. Note that SMJ reviewers, whose reviews are returned on time and are judged satisfactory by the Editors, may receive 1 CME credit per review, with a maximum of 5 credits per year, from the Saudi Council for Health Specialties.
Acknowledgment
We would like to thank Dr. Halil İ. Ada from the Department of Radiology for reviewing the cranial images.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 10, 2014.
- Accepted December 28, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}